










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 no.4 Pretoria abr. 2013
RESEARCH
Gastric adenocarcinoma in Zambia: A case-control study of HIV, lifestyle risk factors, and biomarkers of pathogenesis
V KayambaI; A W AsombangII, VII; V MudendaVIII; M M LisuloIII; E SinkalaIV; S MwanamakondoV; I MweembaIX; P KellyVI, X
IMMed. Tropical Gastroenterology and Nutrition Project, Department of Medicine, University of Zambia School of Medicine, Lusaka, Zambia
IIMD, MPH. Tropical Gastroenterology and Nutrition Project, Department of Medicine, University of Zambia School of Medicine, Lusaka, Zambia
IIIMSc. Tropical Gastroenterology and Nutrition Project, Department of Medicine, University of Zambia School of Medicine, Lusaka, Zambia
IVMMed. Tropical Gastroenterology and Nutrition Project, Department of Medicine, University of Zambia School of Medicine, Lusaka, Zambia
VRN. Tropical Gastroenterology and Nutrition Project, Department of Medicine, University of Zambia School of Medicine, Lusaka, Zambia
VIMD, FRCP. Tropical Gastroenterology and Nutrition Project, Department of Medicine, University of Zambia School of Medicine, Lusaka, Zambia
VIIMD, MPH. Washington University School of Medicine, St Louis, Missouri, USA
VIIIMD, MRCPath. Department of Pathology and Microbiology, University Teaching Hospital, Lusaka, Zambia
IXDipBiomedSci. Department of Pathology and Microbiology, University Teaching Hospital, Lusaka, Zambia
XPMD, FRCP. Blizard Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, London, UK
ABSTRACT
BACKGROUND: Gastric cancer is a leading cause of cancer deaths worldwide but there are few data from Africa. We recently observed a trend towards diagnosis in younger patients.
OBJECTIVE: To test the hypothesis that HIV might have altered risk factors for acquisition of gastric cancer, in a case-control study in the University Teaching Hospital, Lusaka, Zambia.
METHODS: Patients (n=52) with confirmed gastric adenocarcinoma and controls (n=94) undergoing endoscopy but with no macroscopic gastric pathology. Established risk factors and HIV status were compared.
RESULTS: HIV status did not differ significantly between cases and controls (odds ratio 1.03; 95% CI 0.2 - 4.3; p=1.00) and seroprevalence in cases was similar to that of the Zambian population. Smoking, regular alcohol intake, and gastric atrophy were all associated with cancer in univariate and multivariate analysis. Helicobacter pylori serology was positive in 84% of patients studied and cytotoxin-associated gene A (cagA) serology in 66%; neither serological marker was associated with cancer. Atrophy was common in cases (57%) and controls (30%) and associated with both smoking and alcohol use. Intestinal metaplasia was present in 17% of the controls, but was not associated with atrophy.
CONCLUSIONS: HIV was not associated with gastric cancer and does not explain the apparent younger age distribution. Atrophy was common and was not essential for the development of intestinal metaplasia, suggesting that gastric carcinogenesis in Africa does not always follow the pathway from atrophy to intestinal metaplasia to gastric carcinoma (the so-called Correa pathway).
Gastric cancer is one of the most epidemiologically significant cancers in the world. It is the fourth most common cancer, and second only to lung cancer as the leading cause of cancer deaths worldwide.[1] The incidence of gastric cancer varies in different regions of the world; the highest is in Japan and Korea.[2,3] In 2008, GLOBOCAN estimated the incidence in Eastern Asia at 42.4 per 100 000 per year in men and 18.3 in women, and in Western Europe at round 8.6 and 4.2 respectively.[1] Accurate data on the incidence of most cancers in Africa are lacking and gastric cancer is no exception.[4] It has been estimated that the incidence is 5.6 and 4.0 per 100 000 per year in men and in women respectively in East Africa (the region that includes Zambia), and it was reported as the ninth leading cause of cancer mortality in Africa.[1]
Gastric cancer has been shown to be influenced by many factors, no single factor being identified as being causal,[5] though Helicobacter pylori infection is a dominant permissive factor. Lifestyle and environmental factors are implicated in the marked geographical variation of gastric cancer incidence.[4] Known risk factors for gastric cancer include infection with H. pylori, smoking, alcohol and diet.[4] The prevalence of H. pylori in the adult population of Lusaka is 81%[6] but there are no data on the interaction between H. pylori infection, lifestyle, gastric atrophy and other risk factors.
We previously observed that gastric cancer in Zambia seems to occur frequently in young adults7 but the reason for this is unclear.
A retrospective audit of endoscopy unit records at the University Teaching Hospital (UTH) in Lusaka, which is the largest referral hospital in Zambia, revealed that, in 1980 and 1982, all patients with gastric cancer were over the age of 50 years, but a 5-year audit between 2002 and 2007,[7] and an audit in 2009 (Kayamba, unpublished observations), showed that the proportion of young patients with gastric cancer was 20 - 25%. Changes in referral pattern or better endoscopic equipment, or alternative secular trends over the last 30 years, might explain this alarming observation; but there exists the possibility that it reflects exposure to a major biological health hazard. Since its recognition in Zambia in 1984, the HIV pandemic has had a major effect on public health, and has been causally related to malignancies such as lymphoma and Kaposi's sarcoma. Notably, HIV predominantly affects adults in the age range 15 - 45 years.
We report on a case control study designed to investigate a possible association between gastric cancer and HIV infection. We also evaluated the presence of H. pylori infection, the virulence factor cytotoxin-associated gene A (cagA), and gastric atrophy measured by the pepsinogen 1 to 2 ratio and fasting gastrin-17 levels alongside other known risk factors for gastric cancer.
Methods
We carried out a prospective case-control study at UTH from November 2010 to January 2012. Ethics approval was obtained from the Biomedical Research Ethics Committee of the University of Zambia (reference number 008-02-10). Only adults 18 years or older presenting to the endoscopy unit were eligible for inclusion. Cases (n=52) were defined as patients with histopathologically proven adenocarcinoma, while controls (n=94) were patients with symptoms of dyspepsia but no mucosal abnormality seen at endoscopy. Two controls were selected for each case, and these were matched for sex; we attempted to achieve matching for age in the following age bands: <30 years, 31 - 45 years, 46 - 60 years and >60 years. Patients who declined consent for an HIV test were excluded from the study, with all patients included giving written consent.
Endoscopic evaluation
Biopsies (>6) were taken from any gastric lesion suspected to be malignant, and any adenocarcinoma was classified as diffuse, intestinal or of mixed type, according to the Lauren classification. In controls, duplicate biopsies were obtained from the antrum, body and cardia of the stomach and evaluated for inflammation (acute or chronic), atrophy and intestinal metaplasia. Biopsies were evaluated by an experienced pathologist (VM) and processed using haematoxylin/eosin and Giemsa stains and, where requested by the pathologist, periodic acid-Schiff (PAS). Five patients elected to take their biopsies to private histopathology services, and in 2 cases no Lauren classification was available.
Blood tests
Blood was collected to obtain serum which was then separated into aliquots and stored at -80ºC until further analysis. For the H. pylori serology, pepsinogen 1 and 2 and gastrin-17 assays, Biohit Gastro Panel ELISA kits were obtained from Biohit (Helsinki, Finland), and for CagA, ELISA kits were obtained from Genesis Diagnostics (Cambridgeshire, UK) and used according to the manufacturer's instructions. The presence of HIV infection was determined using Determine (Alere, Chiba, Japan) for screening and Unigold (Trinity Biotech, Wicklow, Ireland) for confirmation.
Data analysis
Data were anonymised and coded, then analysed using STATA 10.1 (Stata Corp, College Station, USA). For continuous variables showing a non-Gaussian distribution (i.e. all serological data), median and interquartile range is reported, and the Kruskal-Wallis test was used to compare the two groups; for categorical variables, Fisher's exact test was used. Correlations were examined using Spearman's rank correlation coefficient. An odds ratio (OR) with 95% confidence interval (CI) was used to express relative risk. A probability value <0.05 was considered statistically significant. For multivariate analysis, backwards stepwise unconditional logistic regression was used to assess the relative contributions of different exposure variables to the risk of gastric cancer. Conditional models were also assessed but, in view of the imperfect matching by age and the sparse data problem[9] consequent on having matching by 8 possible categories of age and sex, unconditional logistic regression was selected for the final model. In the end, both models gave very similar results.
Role of the funding source
The funding organisation had no role in the design and conduct of the study, in the collection, analysis and interpretation of the data, or in the preparation, review and approval of the manuscript.
Results
A total of 105 patients with suspected gastric cancer at endoscopy were initially enrolled. The suspicion was based on the presence of a gastric ulcer with raised edges or an obvious tumour mass. On histological analysis, 52 had confirmed adenocarcinoma, 8 had gastric lymphoma, 2 Kaposi's sarcoma (KS) and 1 malignant gastro-intestinal stromal tumour (Fig. 1). The remaining samples did not show any evidence of malignancy and were treated as benign gastric ulcers and followed up as such. For the analysis, only patients with confirmed adenocarcinoma were included. None of the patients with gastric cancer declined to give consent for participation in the study.

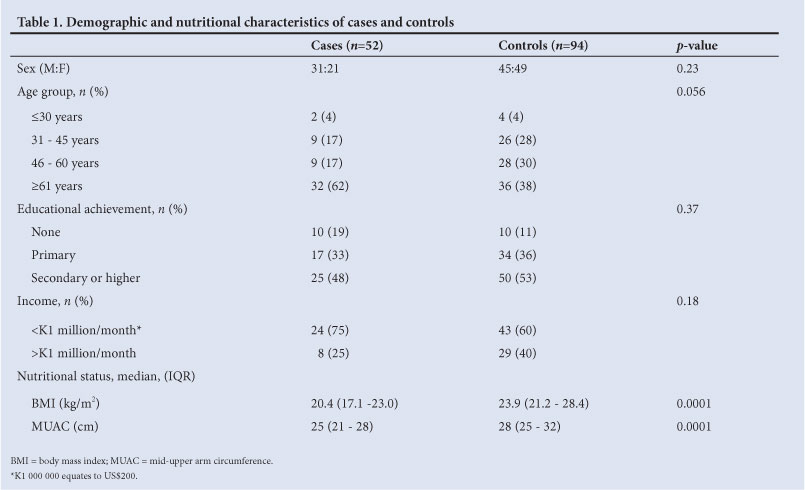
We were unable to recruit 2 controls contemporaneously for each case in the correct age band, largely owing to the small number of patients above the age of 60 years with normal findings at oesophagogastroduodenoscopy, but there was no statistically significant difference in the baseline characteristics between the cases and controls (Table 1). The average age among the cases was 60.6 years, and among the controls 54.1 years. Eleven (21%) of the gastric cancer patients were 45 years of age or younger. As expected, cases had significantly lower body mass index (BMI) and middle upper arm circumference (MUAC) than the controls (Table 1).
Histology revealed that up to 82% of the cancers were of the intestinal type, 17% were of the diffuse type, and 2% were mixed. Stratification by site showed that 62% of the cancers involved the antrum; of those that involved the cardia, the majority (6/10) were of the diffuse type. The mixed type of adenocarcinoma was only found in the antrum of 2 patients.
HIV testing
In total, 4 (8%) cases and 7 (7%) controls were seropositive for HIV (OR 1.03, 95% CI 0.2 - 4.3; p=1.00). There was no association with HIV when only younger patients were analysed (2 of 11 cases <45 years old and 3 of 30 controls; OR 2.0; 95% CI 0.1 - 20.3; p=0.60).
Lifestyle and serological risk factors in cases and controls
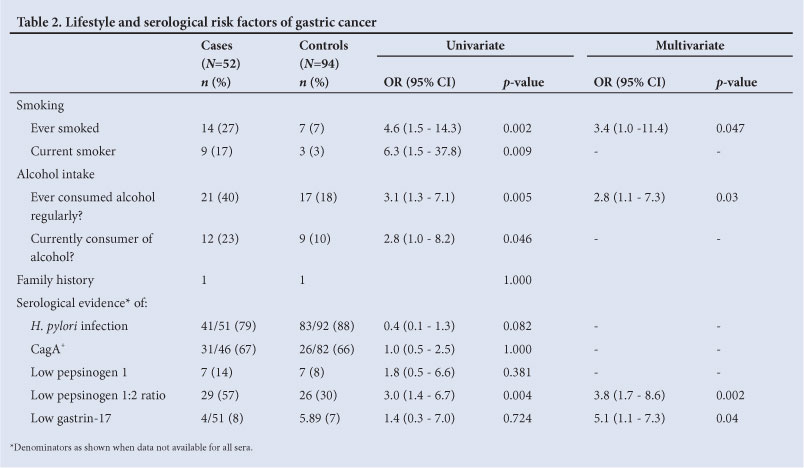
Some of the known risk factors of gastric cancer were also assessed in this patient population and compared between cases and controls (Table 2). Alcohol and cigarette smoking were found to increase the odds of developing gastric cancer in univariate and multivariate analysis. Low reported household income (dichotomised around K1 000 000 (US$200) per month) was not found to increase the odds of developing gastric cancer, though it approached significance (Table 1).
Serological markers of gastric cancer were also evaluated in these patients. The ratio of pepsinogen 1 to 2, a marker of gastric atrophy in the proximal stomach (fundus and corpus), was significantly lower in cases than the controls in both univariate and multivariate analysis (Table 2). The average age of the controls with low pepsinogen 1:2 ratio was 55.5 years. Overall, 84% of all patients had antibodies to H. pylori infection (79% in cases, 88% in controls; p=0.08). Most patients had normal serum levels of serum gastrin-17, a marker of distal (antral) atrophy, and pepsinogen 1.
In multivariate analysis using unconditional logistic regression (Table 2), a statistically significant increase in risk was demonstrated in smokers, in patients with a history of ever having consumed alcohol on a regular basis, and in patients with markers of atrophy (low pepsinogen 1:2 ratio and low gastrin-17).
Precursor lesions in controls
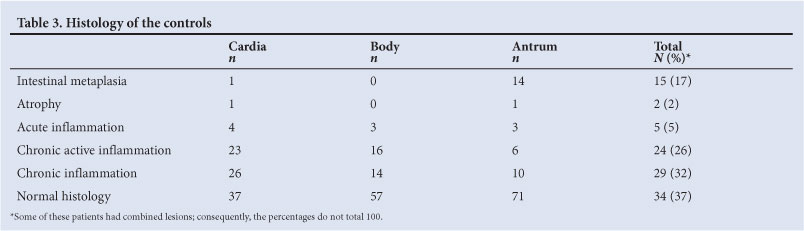
None of the controls showed any evidence of dysplasia on histological analysis. Histologically, the prevalence of intestinal metaplasia in controls was found to be 17%, with over half of the controls having acute or chronic gastric inflammation (Table 3, Fig. 1). Only 2% of all the controls had histological evidence of gastric atrophy. Intestinal metaplasia was not restricted to patients with a background of gastric atrophy. Using low pepsinogen 1:2 ratio as a marker of atrophy, 6/14 (43%) of patients with intestinal metaplasia did not have atrophy, and none of the patients with intestinal metaplasia had atrophy as assessed by low serum gastrin-17.
Serological markers of proximal gastric atrophy were also associated with lifestyle risk factors. Median (IQR) pepsinogen 1:2 ratio was lower in current smokers (cases and controls combined, as few controls were smokers) than in non-smokers (1.96 (1.1 -3.5) v. 3.9 (2.3 - 6.3); p=0.02). Similarly, current alcohol drinkers had lower median (IQR) pepsinogen 1:2 ratios than non-drinkers (1.87 (1.2 - 4.1) v. 4.0 (2.4 - 6.3); p=0.01). No such differences were found in gastrin concentrations between smokers and drinkers. Low pepsinogen 1:2 ratio in controls was not correlated with H. pylori status (OR 1.33; 95% CI 0.22 - 14.4; p=1.0) though only 2 (8%) of the controls with evidence of atrophy were seronegative for H. pylori. This was also true for cagA (p=0.31); 27% of patients with atrophy were seronegative for cagA. We also checked for correlation among the serological parameters. Serum levels of pepsinogen 1 were found to correlate with pepsinogen 2 in controls (Spearman's ρ =0.44, p<0.0001) but not cases (Spearman's ρ=0.22, p=0.12). Conversely, an inverse correlation was found between serum gastrin-17 and pepsinogen 1:2 ratio in the cases (Spearman's ρ=-0.29, p=0.038) but not controls (Spearman's ρ=-0.02, p=0.84). We also calculated the ratio of gastrin-17:pepsinogen 2 as an alternative index of antral atrophy. Gastrin-17:pepsinogen 2 ratio was found to correlate with pepsinogen 1:2 ratio in controls (Spearman's ρ=0.31, p=0.004) but not in cases (Spearman's ρ=0.12, p=0.40).
Discussion
Gastric cancer is one of the most common causes of cancer-related mortality worldwide, yet data from Africa are very limited.[4, 10]-Our data do not support the hypothesis that gastric cancer is associated with HIV, which we had proposed to explain our clinical observations. In this study, 11 (21%) of 52 cases were <45 years of age, in contrast with 6.4% in the USA.[11] We do not believe that this is due merely to the difference in population age distribution.[7] Males also seem to be affected more than females in a ratio of 1.5:1, which is consistent with data from around the world. The male predominance held true in young patients (8:3), which suggests that in Africa, in contrast with industrialised countries, adenocarcinomas in the young are not dominated by diffuse cancers related to familial cancer syndromes. Indeed, 10/11 of these cancers in the young were of the intestinal type, and only one was diffuse. Smoking and alcohol intake appear to contribute to cancer risk, just as in other populations. H. pylori infection is common in cases and controls alike, and appears to be slightly less common in cases, which we surmise may be due to reduced colonisation in the achlorhydric stomach during malignant transformation. Ingestion of acid suppressants to relieve symptoms is another possibility. Most of the cases of adenocarcinoma were found to be associated with gastric atrophy as evidenced by the low pepsinogen 1:2 ratios, and to be of the intestinal type that is more influenced by environmental factors.
Our data seem to confirm that cancer in young adults is a significant proportion of the overall burden, consistent with data from South Africa.[12] We found no suggestion that HIV explains these gastric cancers in the young adult. The overall prevalence of HIV infection found in this study was lower than the national prevalence of 14%.'131 This can be explained by the fact that the average age of the patients enrolled was 60.6 years and, in Zambia, the prevalence of HIV infection in that age group is much lower than 14%. In the present study, the proportion of HIV infection among young patients (<45 years) is similar to the prevalence recorded in the Zambian demographic and health survey of 2007,[13] in which the prevalence of HIV infection in the 18 - 45 age group varied between 12% and 26% across the country. If HIV were the dominant explanation of the changing epidemiology of gastric cancer in Zambia, the proportion of patients with the infection would have been significantly higher among the cases.
Smoking and alcohol intake were found to be strongly associated with gastric cancer in both univariate and multivariate analysis, and associated with gastric atrophy in the controls. Information was obtained on which patients were still smoking or taking alcohol at the time of enrolment and which patients had stopped. However, the type or the duration of exposure to these risk factors was not evaluated. Cigarettes in Zambia are often made by the consumer and of variable (often formidable) strength; and alcohol is consumed as either home-brewed millet beer or home-distilled maize spirit. Consequently, exposure is difficult to quantify and, while current tobacco intake could be estimated from cotinine concentrations, this does not indicate past exposure. Such biomarker measurements would also be of limited value owing to behaviour modification as a result of ill-health.
H. pylori is a known carcinogen and may explain two-thirds of all gastric cancers worldwide.[14] Its prevalence in Zambia is known to be high[6] and, if the only factor at play, the incidence of gastric cancer might also be expected to be high. We found no significant difference in H. pylori seroprevalence between the cases and the controls, but in a case-control study we cannot obtain information on duration or intensity of exposure. As H. pylori infection is related to socio-economic and housing conditions, it is probable that intensity of exposure is high. A relationship between infection and cancer is further obscured when the risk factor is so common in the control group and when the onset of disease is likely to affect intensity of bacterial colonisation (through hypochlorhydria) and therefore the sensitivity of the diagnostic test.[15-17] The H. pylori virulence factor cagA likewise did not differ in cases and controls, which is consistent with other studies in high-prevalence areas.[18] The prevalence of intestinal metaplasia in healthy people in African studies varies from 4% to 28%;[4] our data fall into the middle of this range.
In a setting dominated by intestinal-type cancers, as in Zambia, gastric atrophy is an important precursor lesion leading to intestinal metaplasia and then cancer as suggested by Correa et al.[19] Atrophy, as assessed by serum pepsinogen 1:2 ratio,[20] was strongly associated with cancer, which is consistent with previous work. This was not true of low gastrin-17, which largely reflects antral atrophy. In a recent review, we found the prevalence of atrophy to be high (25% or more) in 5 out of 9 studies from Africa,[4] and our serological data are consistent with a high prevalence of atrophy compared with 12% in Finland[21] and 27.6% in Japan.[22] We found no evidence that atrophy is more prevalent in patients with the intestinal type of gastric cancer, which differs from recent work in Germany.[19] Our data suggest that intestinal metaplasia can occur independently of gastric atrophy, whether assessed histologically or serologically. If this suggestion is confirmed by other studies in Africa that use multiple measures of atrophy simultaneously, the Correa model of gastric carcinogenesis may require further refinement.
Our study has clearly demonstrated the need for more work on gastric cancer in Africa, as the reasons for early onset of the cancer have not been established.
Author contributions. The study was designed by PK, AWA, VK and VM. VK, AWA, ES, SM and PK enrolled patients. VM and IM performed histopathological analysis. VK, AWA, VM, MML, ES, SM, IM and PK interpreted the data, and prepared the initial draft and the final manuscript. PK performed statistical analysis. PK is the guarantor of the study.
Acknowledgements. We are grateful to Mrs Rose Soko and Mr Themba Banda for their work in the endoscopy unit. The work was funded by a Fogarty fellowship to AWA, through NIH grant #R24TW007988 and the American Relief and Recovery Act.
References
1. Ferlay J, Shin H, Bray F, Forman D, Mathers C, Parkin DM. Estimates of world burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893-2917. [http://dx.doi.org/10.10024/ijc.25516; [ Links ]
2. Yamamoto S. Stomach cancer incidence in the world. Jpn J Clin Oncol 2001;31:471. [http://dx.doi.org/10.1093/jjco/31.9.471; [ Links ]
3. Ahn YO, Park BJ, Yoo KY, et al. Incidence estimation of stomach cancer among Koreans. J Korean Med Sci 1991;6:7-14. [ Links ]
4. Asombang AW, Kelly P. Gastric cancer in Africa: what do we know about incidence and risk factors? Trans Roy Soc Trop Med Hyg 2012;106:69-74. [http://dx.doi.org/10.1016/j.trstmh.2011.11.002; [ Links ]
5. Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol 2006;12:354-362. [ Links ]
6. Fernando N, Holton J, Zulu I, Vaira D, Mwaba P, Kelly P. Helicobacter pylori infection in an urban African population. J Clin Microbiol 2001;39:1323-1327. [http://dx.doi.org/10.1128.jcm.39.4.1323-1327.2001Links ] Arial, Helvetica, sans-serif" size="2">;
7. Kelly P, Katema M, Amadi B, et al. Gastrointestinal pathology in the University Teaching Hospital, Lusaka, Zambia: review of endoscopic and pathology records. Trans Roy Soc Trop Med Hyg 2008;102:194-199. [http://dx.doi.org/10.1016/j.trstmh.2007.10.006] [ Links ]
8. Lauren P. The two histological main types of adenocarcinoma: Diffuse and so-called intestinal type of adenocarcinoma. Acta Path Microbiol Immunol Scand 1965;64:31-49. [ Links ]
9. Greenland S, Schwartzbaum JA, Finkle WD. Problems due to small samples and sparse data in conditional logistic regression analysis. Am J Epidemiol 2000;151:531-539. [ Links ]
10. Parkin DM, Sitas F, Chirenje M, Stein L, Abratt R, Wabinga H. Part I: Cancer in indigenous Africans -Burden, distribution, and trends. Lancet Oncology 2008;9:683-692. [http://dx.doi.org/10.1016/s1470-2045(08)70175.x] [ Links ]
11. Howlader N, Noone AM, Krapcho M, et al., eds. SEER Cancer Statistics Review, 1975-2009. Bethesda, MD: National Cancer Institute, 2012. http://seer.cancer.gov/csr/1975_2009_pops09 (accessed 12 March 2012). [ Links ]
12. Matley PJ, Dent DM, Madden MV, Price SK. Gastric carcinoma in young adults. Ann Surg1988;208:593-596. [ Links ]
13. Central Statistical Office (CSO), Ministry of Health (MOH), Tropical Diseases Research Centre (TDRC), University of Zambia and Macro International Inc. Zambia Demographic and Health Survey 2007. Calverton, Maryland, USA: CSO and Macro International, 2009. [ Links ]
14. Parkin DM.The global health burden of infection associated cancers in the year 2002. Int J Cancer 2006;118:3030-3044. [http://dx.doi.org/10.1002/ijc.21731] [ Links ]
15. Kokkola A, Kosaune TU, Puolakkain P, Sipponen P, Harkonen M, Laxen F. Spontaneous disappearance of Helicobacter pylori antibodies in patients with advanced atrophic corpus gastritis. APMIS 2003; 11:619-624. [http://dx.doi.org/10.1034/j1600-0463.2003.1110604.x] [ Links ]
16. Gao L, Weck MN, Nieters A, Brenner H. Inverse association between a pro-inflammatory genetic profile and Helicobacter pylori seropositivity among patients with chronic atrophic gastritis: enhanced elimination of the infection during disease progression? Eur J Cancer 2009;45:2860-2866. [http://dx.doi.org/10.1016/j.ejca.2009.04.015] [ Links ]
17. Peleteiro B, Lunet N, Barros R, La Vecchia C, Barros H. Factors contributing to the underestimation of Helicobacter pylori associated gastric cancer risk in a high prevalence population. Cancer Causes Control 2010;21:1257-1264. [http://dx.doi.org/10.1007/s10552-010-95532] [ Links ]
18. Klusters G, van Vliet AH, Kuipers EJ. Pathogenesis of Helicobacter pylori infection. Clin Microbiol Rev 2006;19:449-490. [http://dx.doi.org/10.1128/cmr.00054-05] [ Links ]
19. Correa P, Haenszel W, Cuello C, Tannenbaum S, Archer M. A model for gastric cancer epidemiology. Lancet 1975;2:58-60. [http://dx.doi.org/10.1016/50140-6736(75)90498-5] [ Links ]
20. Bornschein J, Selgrad M, Wex T, Kuester D, Malfertheiner P. Serological assessment of gastric mucosal atrophy in gastric cancer. BMC Gastroenterology 2012;12:10. [http://dx.doi.org/10.1186/1471-230x-12-10] [ Links ]
21. Cook MB, Dawsey SM, Diaw L, et al. Serum pepsinogens and Helicobacter pylori in relation to the risk of esophageal squamous cell carcinoma in the alpha-tocopherol, beta-carotene cancer prevention study. Cancer Epidemiol Biomarkers Prev 2010;19:1966-1975. [http://dx.doi.org/10.1158/1055-9965.epi-10-0270] [ Links ]
22. Toyoda K, Furusyo N, Ihara T, Ikezeki H, Urita Y, Hayashi J. Serum pepsinogen and Helicobacter pylori infection - a Japanese population study. Eur J Clin Microbiol Infect Dis 2012;31:2117-2124. [http://dx.doi.org/10.1007/s10096-011-1543-0] [ Links ]
Accepted 30 November 2012.
 Corresponding author: P Kelly (m.p.kelly@qmul.ac.uk)
Corresponding author: P Kelly (m.p.kelly@qmul.ac.uk)


{kind=link}
{kind=link}
{kind=link}