










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 no.3 Pretoria mar. 2013
FORUM
ISSUES IN MEDICINE
Risks identified in implementation of district clinical specialist teams
R NathanI; P RautenbachII
IPublic Health Medicine specialist at the University of Limpopo (MEDUNSA campus); her interests include health systems management
IIHead of the Department of Community Medicine at the same campus
ABSTRACT
The District Clinical Specialist Team (DCST) is a strategy implemented by the South African National Department of Health to strengthen district health systems. An amount of R396 million per annum will be required to fund posts in all 52 districts. During implementation, numerous risks were identified, the major one being the most expensive category of DCST personnel, i.e. Head of Clinical Unit. Similar risks will probably apply to other categories of personnel within the DCST. To achieve the objectives of the DCST strategy, risk reduction strategies need to be promptly applied.
The District Clinical Specialist Team (DCST), each managed by a Head of Clinical Unit (HOCU), is one of the strategies within the three streams of primary healthcare (PHC) re-engineering that is being implemented to strengthen health systems. The aim is to establish a DCST in each of the 52 districts of South Africa (SA).[1] A DCST comprises a family physician (FP), PHC nurse, an obstetrician and gynaecologist, advanced midwife, a paediatrician, paediatric nurse[1] and an anaesthetist to oversee emergency and peri-operative care.[1]
The objective of the DCST is to improve quality of healthcare and outcomes for mothers, new-borns and children by performing clinical and non-clinical functions.[1] In terms of the Ministerial Task Team Report, it is recommended that only 10 - 20% of the workday (i.e. about 1 - 1.5 hours per day) be spent on maintaining clinical competency.[1] In practice, the time spent on clinical work by a specialist would translate into a maximum of 2 consultations per day or 1 surgical procedure per day, for an entire district.
The Ministerial Task Team has proposed a conditional grant to fund and sustain the costs of the DCST strategy. The salaries of the doctors involved are compatible with that of a HOCU.[1] An additional budget of approximately R396 million per annum will be required to fund posts in all 52 districts in South Africa.
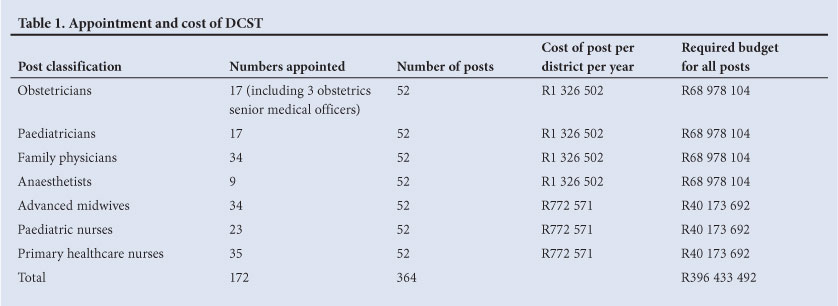
In September 2012, Health Minister Aaron Motsoaledi announced that, of a total of 364 posts created, 172 appointments had been made, i.e. 47% of posts had been filled (Table 1).[2]
In assessing the DCST strategy with specific reference to HOCUs, numerous risks were identified.
Identified risks
Risk 1: Failure to retain HOCUs in DCSTs may bring about human resource and financial imbalances in the public health system
Despite HOCUs being successfully recruited in some districts, doubts have been expressed about the length of their retention.[1] The authors forecast that, once HOCUs have obtained the commensurate remuneration scale, they will tend to move from one district to another, or to secondary and tertiary facilities, and ultimately to urban areas and facilities in the health system with better working conditions. The Department of Public Service and Administration (DPSA)'s policy entitled 'Transfer Framework to Facilitate Transfers of Personnel between Spheres of Government' states that 'employee entitlements as embodied in their conditions of service are protected and the conditions of service of transferred employees may not, on the whole, be less favourable than those received from the old employer.'[3] This transfer policy prescript will enable transfers by HOCUs.
In addition, the number of specialist posts far exceeds the number of HOCU posts within the public health system, making it easier to obtain a specialist post than a HOCU post. A HOCU may retain that salary level, even if deciding to occupy a specialist post in urban districts, or secondary or tertiary hospitals. If this does occur, it will place an additional financial burden on the part of the health system receiving the HOCU in a specialist funded post.
Risk 2: HOCUs will ultimately perform their commuted overtime duties in district facilities if the regional or tertiary hospital is too far away from their district-based location
The authors expect the above situation to occur in rural districts. PHC costs will increase since all HOCUs (except FPs) will require the support of a medical officer while performing commuted overtime, to deal with generalist cases that fall outside the specialist's scope of practice. FPs are the only category of specialists who are equipped to deal with generalist cases. In other words, commuted overtime costs for both a generalist (i.e. the FP and/or the medical officer) and an additional specialist will be incurred, when the need is for generalists only.
According to the Commuted Overtime Policy in Gauteng,[4] HOCUs are restricted to 12 hours of commuted overtime per week; in exceptional cases, 16 - 20 hours may be granted. This amount of overtime can be completed in one night, if not properly negotiated with the facility manager. Using the DCST model, specialist services at a district hospital can only be rendered for a maximum of two nights before the 16 - 20 hours of commuted overtime is exhausted for that specialist. If the overtime hours are spread over the course of the week, other debatable issues may arise, e.g. willingness of the specialist to perform commuted overtime; cost, time and availability of the specialists' services; etc.
It is neither feasible nor practical for a HOCU other than an FP to perform overtime at the district level. Any other HOCU will be limited by the scope of practice of his/her specialist discipline. The current need of district facilities favours generalist over specialist medical skills and expertise. If HOCUs other than the FP perform commuted overtime at district level facilities, it will have the ripple effect of creating an inequity of availability, time and access to specialist care within SA.
Risk 3: HOCUs (the FP excepted) will be restricted in their scope of practice, especially in rural districts, resulting in skills loss
District budgets are rationalised for the provision of a standardised and finite PHC package to address the burden of disease. To curb costs, essential drug lists (EDLs), essential test lists (ETLs) and essential equipment lists (EELs) were developed and aligned with the PHC package. A medical specialist is trained to render primary, secondary and tertiary care. If the HOCU is based in the district and is restricted to primary level use of pharmaceuticals, diagnostics and equipment as prescribed by the essential lists, the secondary and tertiary level skills of the specialist will remain under-used, and skills losses will occur. Secondary and tertiary skills transfer from the HOCU to other doctors may also deteriorate over time.
Risk 4: The pool of existing practising clinical specialists will be diminished by the promotion of 52 specialists of each category on the DCST to HOCU posts
To maintain clinical competency, only 10 - 20% of the time of specialists (i.e. 1 - 1.5 hours per day) should be spent on clinical care at a regional or tertiary hospital.[1] The remaining duties are non-clinical. One of the objectives of the Occupation Specific Dispensation (OSD) was to attract doctors and nurses back to public sector facilities to render clinical patient care, and also to deter them from non-clinical management positions, to reduce staff shortages and improve health outcomes. When OSD was implemented, the demand for clinical expertise far outweighed the demand for management expertise, as it still does. Appointment of specialists to HOCU posts will result in the loss of 52 specialists rendering patient care in each specialty proposed on the DCST. SA currently does not have an adequate supply of doctors[5,6] to prioritise management demand over clinical demand, which is what the DCST currently appears to do.
Furthermore, it is neither practical nor feasible to expect one specialist to perform a greater percentage of clinical work in an entire district; the simple realities of long distances deter this. It is inevitable that the specific category of specialist takes on greater non-clinical functions - including management, mentoring and epidemiological analysis - at a district level rather than at a facility level where the need is arguably greater.
The above-mentioned perceived risks, as identified by the authors, need prompt attention if the DCST is to be successfully implemented as envisaged.
Reduction of risks
A retention strategy for HOCUs, especially in rural districts, needs to be developed urgently. All managers must be made aware of the potential movement of HOCUs within the health system.
In future, instead of appointing HOCUs at the district level, FPs, entry level specialists or medical officers with specialist diplomas (diplomates) should be appointed within district hospitals. However, entry-level specialists should be reserved for the larger district hospitals; this tactic will lower PHC costs, increase access, and reduce time to specialist clinical care within districts. The non-clinical functions (performing assessments on the quality of clinical services; monitoring and evaluation; supporting district level organisational activities, health systems and logistics; collaboration; communication; reporting; teaching; research; facilitation, integration and coordination of staff, services, programmes and packages of care; surveillance; supportive supervision and mentorship[1]) should be performed by HOCUs based at secondary and tertiary hospitals. Until there is a full complement of specialists within the district, appointment of HOCUs should be reserved for secondary and tertiary facilities. HOCUs can provide the necessary clinical governance, outreach and support to district specialists from these higher-level facilities.
Additional FPs and trainee registrars should be injected into the districts. Their posts and budgets should be decentralised from higher-level facilities to the districts. Private sector FPs and general practitioner diplomates may also be utilised on a sessional basis to cover potential gaps in service hours to promote equity, availability, affordability and accessibility to specialist care. The engagement of private FPs and other categories of specialist will assist in bridging the public-private divide, paving the way for the NHI. In the medium to long term, the district might be considered as a worthy training platform in appropriate generalist specialties.
To accommodate specialist expertise in districts, taking into account the burden of disease, the PHC package offered and all essential lists (EDL, ETL and EEL) need to be revised accordingly. There is also a need for the standardisation of definitions/classification and staffing norms of a mobile service, satellite clinic, clinic, community health centre, community day centre and midwife obstetric unit; this should be gazetted.
A strategy of continuous medical education and periodic rotations through higher-level facilities for specialists should be considered to improve specialists' versatility in functioning across all levels of care.
We suggest that Public Health Medicine (PHM) specialist posts be created within each district. PHM specialists together with FPs may be considered as a complementary partnership on the DCST. While the PHM category of HPCSA-registered specialists number only approximately 100, they represent an under-utilised resource. Their scope of practice is ideally suited to the majority of the current functions of a HOCU on a DCST, since it includes, but is not limited to, demography, epidemiology, biostatistics, health systems management, public administration, social sciences, communicable and non-communicable disease control, disease outbreak management and co-ordination, and environmental and occupational medicine. Since PHM specialists are predominantly non-clinical in their scope of practice, and can function across all spheres of government, various sectors and medical disciplines (in a non-clinical manner), they are the resource that should be utilised to achieve the objectives demanded of the DCST strategy.
Those FPs who qualified prior to the promulgation of their specialty in August 2007 should be re-assessed to ascertain their surgical, anaesthetic, obstetric, gynaecological and paediatric skills. Any identified competency gaps should then be addressed by means of mentoring programmes and supervised clinical rotations at higher-level facilities. More of the new category of FPs should be deployed to districts.
Conclusion
The primary role of the DCST is supportive supervision and clinical governance, and not the direct delivery of clinical services.[1] To improve non-clinical medical management at a district level, PHM specialists, whose work is more non-clinical than clinical in nature,[7] are ideally suited. To improve patient care and health outcomes at a facility level, FPs, entry-level specialists and medical officer diplomates are required. HOCUs, other than the FP currently envisaged, are probably misplaced at the district level where, currently, there are few or no specialists to offer supervision. We contend that the DCST requires urgent re-assessment.
References
1. Ministerial Task Team. District Clinical Specialist Teams in South Africa: Ministerial Task Team Report to the Honourable Minister of Health, Dr Aaron Motsoaledi. 2012. http://www.doh.gov.za/list.php?type=Reports (accessed 10 October 2012). [ Links ]
2. Speech for the Minister. Launch of the induction programme of the clinical specialist teams. 27 September 2012. http://www.info.gov.za/speech/DynamicAction?pageid=461&sid= 31283&tid=86339 (accessed 10 October 2012). [ Links ]
3. Department of Public Service and Administration. Transfer Framework to Facilitate Transfers of Personnel between Spheres of Government. Pretoria: Department of Public Service and Administration, 2004. [ Links ]
4. Provincial Department of Health and Social Development. Commuted Overtime Policy. Personnel Circular Minute 43 of 2011. Johannesburg: Department of Health and Social Development: Gauteng Province, 2011. [ Links ]
5. Wildschut A. Doctors in the public sector too few for too many. HSRC Review 2010;8(4). [ Links ]
6. Shortage of doctors beyond critical. 2011. http://www.bonitasmedicalfund.co.za/Health/News/articleType/ArticleView/ articleId/130/Shortage-of-doctors-beyond-critical.aspx (accessed 12 December 2012). [ Links ]
7. Medical and Dental Professions Board of the Health Professions Council of South Africa. Handbook on Ethical Rulings. Pretoria: HPCSA, 2002:106. [ Links ]
Accepted 16 December 2012.
 Corresponding author:
Corresponding author:
R Nathan (ritanathan111@gmail.com)


{kind=link}