










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 no.2 Pretoria feb. 2013
FORUM
CLINICAL PRACTICE
'But it's just a spinal': Combating increasing rates of maternal death related to spinal anaesthesia
Z FarinaI; C RoutII
IChief Specialist at the Pietermaritzburg Metropolitan Department of Anaesthesia, and an honorary lecturer in Anaesthesia at the College of Health Sciences, School of Clinical Medicine, UKZN
IIProfessor of Anaesthesia at the College of Health Sciences, School of Clinical Medicine, University of KwaZulu-Natal (UKZN)
ABSTRACT
The number of women dying as a result of spinal anaesthesia during caesarean section in South Africa is steadily increasing in the triennial reports of the National Committee on Confidential Enquiry into Maternal Deaths (NCCEMD). This article postulates some of the reasons behind this phenomenon. The concern is raised that spinal anaesthesia is being undertaken inappropriately by poorly trained practitioners. A case is made for the rigorous application of known safety standards and for doctors to be appropriately trained in anaesthesia and to be solely responsible for the care of the mother during caesarean section. The need for doctors to be trained and prepared to administer general anaesthesia when required is noted.
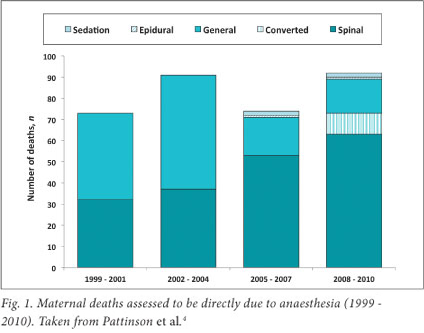
The South African National Confidential Enquiry into Maternal Deaths is unique in that over the last 13 years1-4 an increasing proportion of deaths associated with spinal anaesthesia for caesarean section has been reported (Fig. 1).
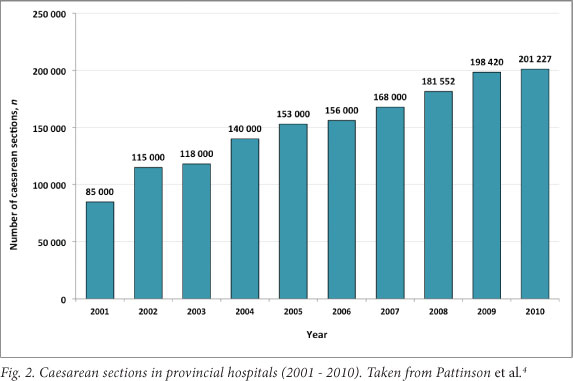
This article is a position statement based on the findings of the fifth Saving Mothers Report (2008 - 2010) published by the National Minister of Health.1 We suggest possible causes for this phenomenon. Due to a lack of denominator data, the reasons for this increase remain speculative, but probably incorporate a combination of factors:
- A rising rate of caesarean sections in SA (Fig. 2).
- Advocacy of regional anaesthesia as being a safer option during caesarean section.56
- A misconception among SA doctors that spinal anaesthesia is inherently safe, leading to two issues which cause mortality and morbidity:
- administration of spinal anaesthesia by doctors who are not fully trained or competent in managing anaesthetic complications
- administration of spinal anaesthesia to patients, not because it is the best form of anaesthesia for the clinical scenario, but because it is the only form of anaesthesia that the doctor feels 'competent' to provide.
In the 2008 - 2010 report, for the first time, sufficient data were available to analyse deaths on an intention-to-treat basis. The analysis reveals a significant number of complications of general anaesthesia occurring in patients in whom spinal anaestheia was intended. This emphasises the dangers of a loss of the skills needed to provide safe general anaesthesia, a phenomenon observed by Tsen.7 This is not an indictment of the move towards increased use of spinal anaesthesia, which internationally is recognised as having a lower mortality rate in appropriate cases and trained hands.6 This, however, does not mean that spinal anaesthesia is absolutely safe.
The misconception that spinal anaesthesia can be performed safely by a doctor in the absence of general anaesthesia skills is seen in advertisements placed for medical officers in SA. For example, one district hospital listed 'perform spinal anaesthesia' as a key competency.8 A more appropriate competency would be 'capable of providing anaesthesia' and include all forms of anaesthesia relevant to the procedures required to be performed at a district hospital.
Another relevant concept is that of 'normalisation of deviance'.9 Substandard care may be provided so often, without apparent consequence, that eventually inferior care becomes the new standard. Spinal anaesthesia is frequently started without first performing an adequate airway examination and considering the possibility of failed intubation. Similarly, oral antacid prophylaxis is no longer administered in many cases. The suggestion that these are important components of safe spinal anaesthesia is regarded as bizarre by many junior doctors attached to our training programme.
Similarly, it is often viewed as acceptable to inject spinal local anaesthetic, then leave the anaesthetised patient under the care of medically unqualified personnel while the doctor performs the surgery or assists. This occurred in 7/92 deaths due to anaesthesia listed in the 2008 - 2010 confidential report.4 This abandonment of the patient was deemed the primary event that led to death in 6/7 cases (86%). Abandonment was also documented in 7/169 deaths due to non- anaesthetic causes assessed for quality of anaesthesia.
In all these cases, the assessors could clearly identify abandonment. The numerous cases where documentation is too inadequate to reveal this problem are not included, and the real magnitude of abandonment in SA may be far higher. No hospital providing an operative obstetric service should place physicians in a situation where this is even considered as an option. Units that cannot provide adequate numbers of appropriately trained staff to avoid this practice should refer their operative obstetrics cases to the nearest available unit that can do so.
Conclusion
The provision of safe anaesthetic services at district-level hospitals must be made a healthcare priority. It is the responsibility of medical managers and hospital chief executive officers to ensure that their staff possess adequate training and skills in both general and spinal anaesthesia. Although performance management contracts place considerable pressure on management to deliver in certain key areas, the threat posed by inadequately trained anaesthetists is sufficiently grave to justify this requirement.
All pregnant patients deserve a high standard of anaesthesia in every facility. The basic minimum standards of obstetric anaesthesia practice are:
- An appropriately equipped operating theatre with all equipment and disposable items checked and in functioning order, as though the patient was receiving general anaesthetia (NCCEMD 2005 -2007 equipment list).3
- Full pre-anaesthetic examination by the doctor providing anaesthesia, including an airway assessment.
- Administration of 0.3 M sodium citrate (30 ml) 0 - 30 minutes before the induction of anaesthesia.
- Provision of anaesthesia appropriate to the patient and her clinical condition (although in most cases this will be spinal anaesthesia at a district hospital, provision must be made for safe general anaesthesia).
- The use of an obstetric wedge to provide appropriate lateral tilt of the gravid uterus in all cases.
- A doctor who has the exclusive responsibility of monitoring and stabilising the patient during anaesthesia (of whatever variety) and who must not be given the additional tasks of assisting the surgery or resuscitating the baby.
References
1. Pattison RC, ed. Saving Mothers. Fifth Report on Confidential Enquiry into Maternal Deaths in South Africa 2008 - 2010. Pretoria: DoH, 2012. http://www.doh.gov.za/docs/reports/2012/savingmothersexec.pdf (accessed 27 September 2012). [ Links ]
2. Pattinson RC, ed. Saving Mothers. Second Report on Confidential Enquiry into Maternal Deaths in South Africa 1999 - 2001. Pretoria: DoH, 2002. [ Links ]
3. Pattinson RC, ed. Saving Mothers. Third Report on Confidential Enquiry into Maternal Deaths in South Africa 2002 - 2004. Pretoria: DoH, 2006. [ Links ]
4. Pattinson RC, ed. Saving Mothers. Report on Confidential Enquiry into Maternal Deaths in South Africa 2005 - 2007. Pretoria: DoH, 2009. [ Links ]
5. Hawkins JL, Koonin LM, Palmer SK, Gibbs CP. Aneasthesia- related deaths during obstetric delivery in the United States, 1979 - 1990. Anesthesiology 1997;86:277-284. [ Links ]
6. National Institutes of Health. Clinical Guideline 132: Caesarean Section. Place: NIH, 2011. http://www.guidance.nice.org.uk/cg132 (accessed 10 September 2012). [ Links ]
7. Tsen LC, Pitner R, Camann WR. General anesthesia for caesarean section at a tertiary care hospital 1990 - 95: Indications and implications. Int J Obstet Anesth 1998;7:147-152. [ Links ]
8. Lamacraft G. Obstetric anaesthesia in Level 1 and 2 hospitals in the Free State. A study and audit And remedial interventions. PhD thesis. Bloemfontein: University of the Free State, 2010. [ Links ]
9. Banja J. The normalization of deviance in healthcare delivery Bus Horiz 2010;53(2):139-148. [ Links ]
Accepted 25 September 2012.
 Corresponding author:
Corresponding author:
Z Farina (zane.farina@kznhealth.gov.za)

