










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.102 no.12 Pretoria Jan. 2012
RESEARCH
Antenatal depression and its risk factors: An urban prevalence study in KwaZulu-Natal
L Manikkam; J K Burns
Department of Psychiatry, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban
ABSTRACT
OBJECTIVE: There has been a recent increase in interest in antenatal depression, which is associated with adverse obstetric, neonatal and maternal outcomes and has been overlooked and underdiagnosed. Local data on prevalence and risk factors are lacking.
AIM: To determine the prevalence and risk factors associated with antenatal depressive symptoms in a KwaZulu-Natal population.
METHODS: The Edinburgh Postnatal Depression Scale and a socio-demographic questionnaire in English and isiZulu were administered to 387 antenatal outpatients at King Edward VIII Hospital in Durban.
RESULTS: Of the participants, 149 (38.5%) suffered from depression and 38.3% had thought of harming themselves in the preceding 7 days. Risk factors for depression included HIV seropositivity (p=0.02), a prior history of depression (p=0.02), recent thoughts of self-harm (p<0.000), single marital status (p=0.04) and unplanned pregnancy (p=0.01).
CONCLUSION: The high prevalence of antenatal depressive symptoms and thoughts of deliberate self-harm supports a policy of routine screening for antenatal depression in South Africa, especially in HIV-seropositive women.
Pregnancy is usually viewed by the public and the medical profession as a period of emotional well-being that is protected against mental disorder. Antenatal care traditionally focuses on physical health rather than on emotional health. Consequently, antenatal depression is regularly overlooked and underdiagnosed, locally and globally.1 In contrast, there has long been a focus on depression in the postpartum period, with considerable literature and public awareness. Only during the past decade have studies of antenatal psychiatric morbidity become more common.2,3
Studies show that the prevalence of antenatal depression is higher than that of postnatal depression.2,3 Low rates are reported from developed countries (4% in Hong Kong4 and 8% in Finland5), but higher rates have been found in low socio-economic settings.6-10 In community- and clinic-based populations, rates of 39% have been reported from two African urban sites (Cape Town6 and Tanzania7) and 47% from an African rural site (KwaZulu-Natal8). Similar rates have been reported from Bangladesh (33%)9 and Pakistan (48%).10
Antenatal depression is associated with adverse fetal, obstetric and neonatal outcomes, including intra-uterine growth retardation (IUGR), low birth weight, preterm delivery and infant behavioural problems.11-13 Nutritional deprivation and poor maternal weight gain during pregnancy are risk factors for IUGR, and when depression is associated with weight loss, fetal growth may be negatively affected. Physiological mechanisms underlying the negative impact of antenatal depression on fetal growth and neonatal development include hyperactivity of the hypothalamo-pituitary axis and increased cortisol secretion.
Apart from physiological effects on the fetus, depression in pregnancy can affect a mother's functional status and cause cognitive distortions that affect her decision-making capacities. This may be associated with poor attendance at antenatal clinics and lack of motivation to follow physician care regimens,5 and lead to other problems such as maternal substance abuse.5 These factors invariably increase the risk of adverse pregnancy outcomes.12 Depression may also amplify somatic symptoms of pregnancy.14
Severe depression carries a risk of psychosis, and of self-injurious and impulsive behaviours. Few data are available on suicidality during pregnancy, which is a further possible outcome of antenatal depression.3,9
Antenatal depression is an independent risk factor for postpartum depression.2,15 Untreated antenatal depression may be associated with a 50 - 60% risk of a postpartum disorder. Up to 50% of cases of antenatal depression are undetected, which coupled with an unwillingness to use medication in pregnant patients makes it likely that most depressed pregnant women will not be on treatment for depression.1
Infants of mothers with postpartum depression may exhibit depression-like behaviours, e.g. fewer expressions of interest, excessive crying and inferior excitability prior to substantial mother-baby interactions.11,12 They have been reported to have inferior performance on the orientation, reflex, excitability and withdrawal clusters of the Brazelton Scale, which assesses neonatal behaviour.13
In developed and developing countries, socio-demographic factors associated with risk of depression during pregnancy include a previous history of depression, low self-esteem, low social support, single status, intimate partner violence, low income, younger age and unplanned pregnancy.6,7,10,15,16 The only previous South African study to investigate risk factors found that lack of partner support, intimate partner violence, low household income and younger age were the strongest predictors of antenatal depression.6
Improving maternal and child health are international and national priorities. The United Nations Millennium Development Goals17 list child health and maternal health as two of the eight goals, while the South African National Department of Health has identified maternal and child health as one of four priority programmes.18 Dealing with depression during pregnancy is relevant to achieving better outcomes for mothers and infants in South Africa. In KwaZulu-Natal, the province with the highest antenatal HIV prevalence rate (39%) and the highest teen pregnancy rate, it is particularly important to investigate the burden of depression in pregnancy and its associated risk factors. We aimed to determine the prevalence of antenatal depressive symptoms and associated socio-demographic risk factors, including HIV status, at King Edward VIII Hospital, Durban.
Methods
Site and study population
The study comprised women attending the antenatal clinic at King Edward VIII Hospital, one of the largest hospitals in South Africa and providing district, regional and tertiary services to KwaZulu-Natal province. It is a teaching hospital to the Nelson R Mandela School of Medicine and serves an ethnically diverse population, mainly of lower socio-economic status. The antenatal clinic offers primary-level care to patients who live locally and serves as a referral clinic for high/medium-risk pregnancies that cannot be managed at primary healthcare level (e.g. previous caesarean sections, multiple pregnancies, and maternal medical conditions such as hypertension, diabetes, epilepsy and asthma). Approximately 1 150 patients attend the clinic each month, most of whom are in the third trimester, as patients are typically referred during the later stages of pregnancy for appropriate delivery planning.
Consecutive pregnant women attending the clinic and literate in English or isiZulu during the month of November 2011 were included until a sample of 390 was reached, a size considered adequate to detect associations between depressive symptoms and risk factors. Owing to missing data on 3 individuals, the analysis was conducted on 387 women.
Instruments
The Edinburgh Postnatal Depression Scale (EPDS), a 10-item self-report scale assessing the symptoms of depression, was used to assess the presence of depression. Each item is scored on a 4-point scale with a total score range of 0 - 30. Its strength is that it omits somatic symptoms that are often associated with depression and may be confounded by pregnancy-related changes, i.e. changes in appetite and weight, energy, nausea and headaches. Rather, it focuses on cognitive and affective symptoms. The scale assesses symptoms in the past 7 days. On the basis of previous studies, a cut-off score of >13 was used to indicate depression. The EPDS was completed in English or using a translated Zulu version developed for the study using standard translation methods.
The EPDS was developed to detect postpartum depression,19 but it has since been validated for use in pregnant women and has satisfactory sensitivity (79%) and specificity.20 It is the only self-report scale that has been validated for use postnatally and during pregnancy. It has been translated into many languages and was validated in postnatal South African women at Coronation Hospital in Johannesburg after being translated into six different South African languages.21 In that study it was validated against the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for depression, and a score of 11 identified 100% of cases of major depression and 70% of cases of minor depression (sensitivity was 80% and specificity 76.6%). The authors concluded that it is a valid screening instrument in the South African urban community.
Participants were also required to fill in a 12-item socio-demographic questionnaire including age, number of pregnancies, gestational age, reason for referral, education, employment, household income, relationship status, HIV status, and whether the pregnancy was planned and initially wanted or unwanted (at the time of 'diagnosing' pregnancy).
Ethics
Ethical approval was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal and institutional approval from King Edward VIII Hospital. All participants signed a written informed consent form. Use of research codes ensured confidentiality and anonymity.
Data collection
The data were collected during November 2011. Consecutive sampling was used, as random presentation of patients was assumed. While women were waiting for their routine antenatal appointments, the purpose and nature of the study was explained to the whole group. They were then given individual patient information sheets in English or isiZulu and invited to participate. Participants self-completed the EPDS and socio-demographic questionnaire. Women who scored 13 and above or who gave a positive answer to an item on deliberate self-harm (DSH) were offered referral to the psychiatric clinic at King Edward VIII Hospital.
Data analysis
Data were analysed using SPSS version 18.0.22 Spearman's correlation coefficients were generated to examine the relationship between depression (a score of 13 or more on the EPDS) and various social, obstetric and clinical variables. Frequencies and odds ratios (ORs) were also calculated. ANOVA was used to determine the relationship between depression outcome and age and gestational age (continuous variables.) Significant variables on bivariate correlation were entered into a logistic regression analysis. A p-value of <0.05 was considered statistically significant.
Results
Social, obstetric and clinical demographics
Unemployed women comprised 65.0% of the sample; 52.9% had completed secondary education; 70.9% were married or had a partner; over half (53.7%) had a gross household income of <R5 000 a month; and the mean age was 27.0 years (range 14 - 46 years, standard deviation (SD) 6.1).
Of the participants 42.2% had high/medium-risk pregnancies (e.g. twins, previous caesarean section, diabetes or hypertension) and 20.2% had low-risk pregnancies; in the remaining 37.6% the reason for referral to the clinic was unknown. Sixty-nine per cent were in their third trimester, with a mean gestational age for the sample of 28.6 weeks (range 2 - 41 weeks, SD 8.4). While 55.1% of the women had not planned to fall pregnant, 57.0% stated they had wanted the pregnancy at the outset.
With regard to HIV status, 27.6% of the participants reported being HIV-seropositive and 53.2% negative; 19.3% did not know their status. Only 6.8% had a previous history of depression, but 38.3% reported having had thoughts of DSH during the previous 7 days.
Prevalence and correlates of depression
Of the sample of 387 women, 149 (38.5%) had an EPDS score of 13 or more, indicating probable depression. When the cut-off EPDS score was changed to 12 or more (consistent with some studies), 174 (44.9%) were depressed. The former was used for statistical analyses.
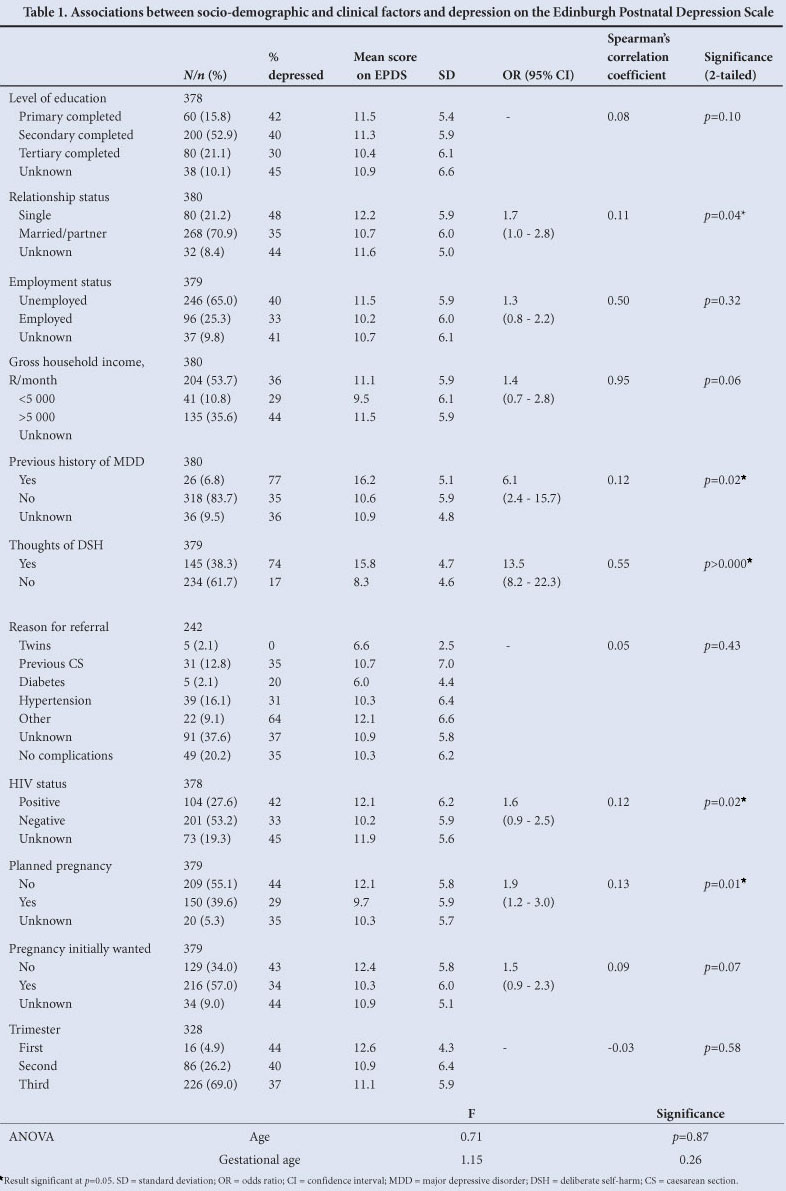
Bivariate correlations using depressed versus non-depressed individuals showed a significant association between being depressed and single marital status, being HIV-positive, having an unplanned pregnancy, having thoughts of DSH, and having a past history of depression (Table 1). ORs for the latter two risk factors were high -women with a prior history of depression were therefore over 6 times more likely to be depressed, with a mean EPDS score of 16.2 (SD 5.1), while those with thoughts of DSH were nearly 14 times more likely to be depressed, with a mean EPDS score of 15.8 (SD 4.7). There were also trend associations between being depressed and having a mean household income <R5 000 per month, and the pregnancy being unwanted at the outset.
In the logistic regression, in which all significant variables from the bivariate analysis were entered, only thoughts of DSH remained a significant predictor of depression (p<0.000) with an OR of 16.7.
Discussion
Consistent with studies from developing countries,6-10 a high estimated prevalence of depression was detected in this KwaZulu-Natal urban population. Notably, when using a conservative EPDS cut-off score of 13 or more, the rate of 38.5% is almost identical to the rate of 39% detected in Khayelitsha, Cape Town, where an EPDS cutoff score of 14 or above was used.6 When we used a less conservative EPDS cut-off score of 12 or more (consistent with some literature), the prevalence rate (44.9%) is higher and approximates the 47% rate in a study in rural KwaZulu-Natal where depression was determined using a structured clinical interview (the SCID).8 Arguably the latter method of detecting depression is superior to a rating scale - our rate of 38.5%, and the Khayelitsha rate of 39%, may therefore be conservative figures. Importantly, our result adds further support to the evidence for an increased prevalence of antenatal depression in developing countries. A meta-analysis of antenatal depression prevalence, in which all but one study was from a developed country, reported rates between 7.4% and 12.8%.2 Rates from developing countries are far higher, approximating 50%.
One might speculate about the reasons for apparently higher rates of antenatal depressive symptoms in developing contexts. The brief on maternal mental health published by the Perinatal Mental Health Project in Cape Town suggests that the high rates of maternal depression in developing countries may be linked to HIV/ AIDS, violence, lack of social support, refugee status, substance abuse and teen pregnancy.23 The World Health Organization states that 'The burden of both reproductive and mental ill-health is greatest in the poorest countries, where health services tend to be dispersed or physically inaccessible, poorly staffed, resourced and equipped, and beyond the reach of many poor people,' and that 'High rates of maternal depression constitute a major public health problem.'24
Risk factors for antenatal depression
We found that the strongest risk factor for depression was having had thoughts of DSH within the last 7 days. While there is an association between being depressed and having thoughts of DSH, depression is not usually a significant predictor of DSH. The strongest predictors of DSH are a history of childhood physical or sexual abuse and certain personality structures.25 Why does this population have such a high rate of thoughts of DSH and why may this be associated with the presence of depression? We suggest that these women have many risk factors that compound their risk of antenatal depression: high HIV prevalence, low income, a high-risk pregnancy in most cases, and a high proportion of unplanned pregnancies. We speculate that among the women with depression in this sample, the compounding effect of these risk factors worsens the severity of the depression, resulting in associated thoughts of DSH.
Other predictors of depression in the bivariate analysis included single marital status, being HIV-positive, having an unplanned pregnancy, and having a past history of depression. These associations with antenatal depression (other than HIV seropositivity) have been demonstrated in the literature, and our findings add further support to them in this urban South African population.
To our knowledge, this is the first time this important association between HIV-positive status and depression in pregnancy has been demonstrated. Studies in rural KwaZulu-Natal8 and in the USA26 found no difference in the rate of depression between HIV-positive and HIV-negative pregnant women. In our study, being HIV-positive places a mother at a significantly increased risk of depression in pregnancy. Notably, while HIV status was 'unknown' in 19.3% of women, we do not consider that this factor undermines our result, since the mean EPDS score in the 'unknown' group was 11.9, which is intermediate between those of HIV-positive women (12.1) and HIV-negative women (10.2). This apparent association is extremely important, especially in a context such as KwaZulu-Natal, where the prevalence of HIV seropositivity in antenatal women is 39%. The association between HIV seropositivity and increased risk for depression has profound implications for evaluating both the direct and indirect negative impact of HIV seropositivity on maternal, perinatal and infant outcomes.
Interestingly, there was no significant relationship between level of education and depression, although the mean EPDS score was higher for those with only primary education compared with those with secondary or tertiary education. Such a relationship might have been expected, as most studies of depression indicate that higher education protects against depression. Most participants fell into the intermediate category of secondary education, which may explain our failure to show a significant differential effect between the primary-and tertiary-educated groups. Similarly, with respect to employment status, while the mean EPDS score for the unemployed group was higher (11.5) than that of the employed group (10.2), this difference was not statistically significant. The failure to attain significance may be because the size of the two groups differed substantially, with 65.0% of women being unemployed. Studies have shown that being employed may be protective against depression.
Limitations
Our study has several important limitations. In terms of sample selection, we excluded illiterate women. While this might have biased our sample (illiterate women may be more vulnerable to depression), the adult literacy rate in South African women in the general population approximates 90%; our sample therefore closely reflected the literacy of the general population.
Our study population was to a significant degree a select population of antenatal women. King Edward VIII Hospital antenatal clinic is a primary healthcare clinic for those who live locally, but is also a referral centre for high/medium-risk pregnancies (including multiple pregnancies, previous caesarean sections, maternal diabetes and maternal hypertension). Our results therefore cannot be generalised to all primary care antenatal clinics or to women not seeking antenatal care. The differing sample sizes for each trimester may have confounded our analysis of depression versus trimester. A systematic review of antenatal depression showed that the risk of depression is highest in the second trimester (12.8%), followed by the third trimester (12%), with the lowest rates in the first trimester (7.4%).2 Our study detected the reverse, but sample sizes were unequal, with 69.0% of our respondents being in the third trimester; our result (which was not significant) should therefore be viewed with caution.
The literature varies regarding the optimal cut-off value for depression on the EPDS. Some studies advocate a score as high as 14 and above, while others use a score as low as 9 and above. We opted to use 13 and above on the basis of the findings of a large systematic review that included 37 studies validating the EPDS in peripartum women. Nevertheless, our results may have been different had we used a different cut-off score.
While the EPDS allows us to assess the likelihood of current depression, it is merely a rating scale - not a diagnostic tool. In the absence of confirmation of the presence of depression by means of a diagnostic clinical interview, we cannot be certain that individuals scoring 13 or above had a depressive illness. We therefore regard this as a preliminary study.
We stress that associations found in this study between socio-demographic, obstetric and clinical factors and depression tell nothing about causality. The cross-sectional design of the study prevents conclusions being drawn regarding causal relationships between exposures and outcomes.
Conclusion and recommendation
Our results confirm studies indicating high rates of antenatal depressive symptoms in developing countries. Recent studies in South Africa, including this study, indicate that more than a third of women have significant depressive symptoms during pregnancy. Thoughts of DSH also often appear to be associated with depressive symptoms. This is of concern, as self-harming ideation is often predictive of self-harming behaviours and should warn of potential danger to mothers and their infants. Maternal suicide is often paired with homicidal intentions and even behaviours towards the infant.
This study also provides evidence that HIV infection may place mothers at additional risk of depression during pregnancy. Such an association, if confirmed by subsequent studies, has major implications for managing peripartum risk in HIV-positive women.
Several recent studies have provided sufficient evidence for depression in pregnancy to be regarded as a significant public health problem in South Africa. Furthermore, it is almost invariably overlooked and remains undiagnosed and untreated in most cases. To realise the national and international objectives of improving maternal and child health, a policy of routine screening for depression in antenatal women should be developed and implemented without delay in South Africa.
Declaration of interests. The authors declare that there is no conflict of interest.
Acknowledgments
The authors acknowledge the women who participated in the study, and also the management and staff of King Edward VIII Hospital for supporting it.
References
1. Alder J, Fink N, Urech C, Hosli I, Bitzer J. Identification of antenatal depression in obstetric care. Arch Gynecol Obstet 2011;284:1403-1409. [http://dx.doi.org/10.1007/s00404-011-1872-3]
2. Bennett HA, Einarson A, Taddio A, Koren G, Einarson TR. Prevalence of depression during pregnancy: systematic review. Obstet Gynecol 2004;103:698-709. [http://dx.doi.org/10.1097/01.AOG.0000116689]
3. O'Keane V, Marsh MS Depression during pregnancy. BMJ 2007;334:1003-1005. [http://dx.doi.org/10.1136/bmj.39189.662581.55]
4. Lee DT, Chan SS, Sahota DS, Yip AS, Tsui M, Chung TK. A prevalence study of antenatal depression among Chinese women. J Affect Disord 2004;82:93-99. [http://dx.doi.org/10.1016/j.jad.2003.10.003] [ Links ]
5. Pajulo M, Savonlahti E, Sourander A, Helenius H, Piha J. Antenatal depression, substance dependency and social support. J Affect Disord 2001;65:9-17. [http://dx.doi.org/10.1016/s0165-0327(00)00265-2]
6. Hartley M, Tomlinson M, Greco E, et al. Depressed mood in pregnancy: prevalence and correlates in two Cape Town peri-urban settlements. Reprod Health 2011;8:9. [http://dx.doi.org/10.1186/1742-4755-8-9] [ Links ]
7. Kaaya SF, Mbwambo JK, Kilonzo GP, et al. Socio-economic and partner relationship factors associated with antenatal depressive morbidity among pregnant women in Dar es Salaam, Tanzania. Tanzanian Journal of Health Research 2010;12:23-35. [http://dx.doi.org/10.4314/thrb.v12i1.56276]
8. Rochat TJ, Tomlinson M, Barnighausen T, Newell ML, Stein A. The prevalence and clinical presentation of antenatal depression in rural South Africa. J Affect Disord 2011;135:362-373. [http://dx.doi.org/10.1016/j.jad.2011.08.011. [ Links ]
9. Gausia K, Fisher C, Ali M, Oosthuizen J. Antenatal depression and suicidal ideation among rural Bangladeshi women: a community-based study. Arch Womens Ment Health 2009;12:351-358. [http://dx.doi.org/10.1007/s00737-009-0080-7]
10. Shah SM, Bowen A, Afridi I, Nowshad G, Muhajarine N. Prevalence of antenatal depression: comparison between Pakistani and Canadian women. J Pak Med Assoc 2011;61:242-246. [ Links ]
11. Evans J, Heron J, Patel RR, Wiles N. Depressive symptoms during pregnancy and low birth weight at term. Br J Psychiatry 2007;191:84-85. [http://dx.doi.org/10.1192/bjp.bp.105.016568]
12. Wisner KL, Sit DKY, Hanusa BH, et al. Major depression and antidepressant treatment: impact on pregnancy and neonatal outcomes. Am J Psychiatry 2009;166:557-566. [http://dx.doi.org/10.1176/appiajp.2008.08081170] [ Links ]
13. Field T, Diego M, Hernandez-Reif M. Prenatal depression effects on the fetus and newborn: a review. Infant Behaviour and Development 2006;29(3):445-455. [http://dx.doi.org/10.1016/j.infbeh.2006.03.003] [ Links ]
14. Kelly RH, Russo J, Katon W. Somatic symptoms among pregnant women cared for in obstetrics: normal pregnancy or depression and anxiety symptom amplification revisited? Gen Hosp Psychiatry 2001;23:107- 113. [http://dx.doi.org/10.1016/S0163-8343(01)00129-3] [ Links ]
15. Robertson E, Grace S, Wallington T, Stewart DE. Antenatal risk factors for postpartum depression: a synthesis of recent literature. Gen Hosp Psychiatry 2004;26:289-295. [http://dx.doi.org/10.1016/j.genhosppsych.2004.02.006] [ Links ]
16. Leigh B, Milgrom J. Risk factors for antenatal depression, postnatal depression and parenting stress. BMC Psychiatry 2008*24. [http://dx.doi.org/10.1186/1471-244X-8-24] [ Links ]
17. United Nations. Millenium Development Goals. http://www.un.org/millenniumgoals/ (accessed 12 May 2012). [ Links ]
18. Department of Health, Republic of South Africa. Health Priorities. http://www.doh.gov.za/ (accessed 12 May 2012). [ Links ]
19. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10 item Edinburgh Postnatal Depression Scale. Br J Psychiatry 1978;150:782-786. [http://dx.doi.org/10.1192/bjp.150.6.782] [ Links ]
20. Cox JL, Chapman G, Murray D, Jones P. Validation of the Edinburgh Postnatal Depression Scale in non-postnatal women. J Affect Disord 1996;39:185-189. [http://dx.doi.org/10.1016/0165-0327(96)00008-0] [ Links ]
21. Lawrie TA, Hofmeyr GJ, De Jager M, Berk M. Validation of the Edinburgh Postnatal Depression Scale on a cohort of South African women. S Afr Med J 1998;88:1340-1344. [ Links ]
22. SPSS Inc. PASW STATISTICS 18.0 Command Syntax Reference. Chicago: SPSS Inc., 2009. [ Links ]
23. Perinatal Mental Health Project. Maternal mental health: addressing key vulnerabilities. Policy Brief 15. http://www.health.uct.ac.za/usr/health/research/groupings/mhapp/ policy_briefs/MHPB15.pdf (accessed 16 May 2012. [ Links ])
24. World Health Organization. Mental Health Aspects ofWomen's Reproductive Health: a Global Review ofthe Literature. Geneva: WHO Press, 2009. [ Links ]
25. Fliege H, Lee JR, Grimm A, Klapp BF. Risk factors and correlates of deliberate self- harm behaviour: a systematic review. J Psychosom Res 2009;66:477-493. [http://dx.doi.org/10.1016/j.jpsychores.2008.10.013]
26. Rubin LH, Cook JA, Grey DD, et al. Perinatal depressive symptoms in HIV-infected versus HIV-uninfected women: a prospective study from preconception to postpartum. J Womens Health 2011;20:1287-1295. [http://dx.doi.org/10.1089/jwh.2010.2485] [ Links ]
Accepted 26 September 2012.
Corresponding author: J K Burns (burns@ukzn.ac.za)


{kind=link}