










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.102 no.7 Pretoria Jul. 2012
FORUM
ISSUES IN CHILD HEALTH
The South African Paediatric Tumour Registry - 25 years of activity
Daniela C StefanI; David K StonesII
ISouth African Paediatric Tumour Registry and Head of Paediatric Haematology Oncology at Tygerberg Children's Hospital and Stellenbosch University, W Cape
IISouth African Childhood Cancer Study Group and Head of Paediatric Haematology Oncology at Universitas Hospital, University of the Free State, Bloemfontein
ABSTRACT
The South African Children's Tumour Registry was established 25 years ago as it was essential to collect data on malignant disease in the paediatric population that can be used for statistical research in an efficient and sustainable way. The Registry is a useful and significant repository of specific paediatric data, along with the recently revitalised National Cancer Registry, to serve the needs of the cancer research community.
Childhood cancer is relatively rare, representing about 1% of cancers in the total population. The cumulative risk of developing cancer below the age of 15 years has been estimated to be between 1 and 2.5 per 1 000.1 Childhood cancer is generally potentially curable, and progress towards cure has been made in developed countries where the overall survival rate for some common malignant tumours is about 80%.2 In South Africa, where children under 15 years (who constitute the paediatric population) represent 31% of the population,3 600 - 700 new cases of childhood malignancies have been reported yearly for the last 25 years to the South African Children's Tumour Registry.
The Registry is essential for collecting data on malignant disease in the paediatric population. It is a central repository of data provided by individual, hospital-based registries throughout the country. These registries record data on all patients presenting to paediatric oncology services; however, children who die without being seen at a hospital, and those treated by private oncologists and other paediatric subspecialists (e.g. neurosurgeons), might not be recorded. Although a central registry of hospital-based registers cannot be complete, it nevertheless has data that can be used for statistical research in an efficient and sustainable way.
The Registry commenced in 1987 as an initiative of the South African Children's Cancer Study Group (SACCSG). Paediatric oncology units in the country collaborate, and data also come from several oncologists and interested parties in private practice. All units have ethical approval to collect and submit data to the Registry. The Registry was hosted over time by various paediatric oncology units in the country; for the last 15 years, it has been kept at Stellenbosch University.
There is no other dedicated children's cancer registry in Africa, although the International Association of Cancer Registries has 60 African members. However, only 17 of these are national registries; the rest are regional or hospital-based registries.4 The data in these registries include children and adults; therefore, some meaningful children's data could be missed.
The Registry's objectives
The objectives of the Registry are to determine: age-specific incidences; relative frequencies of various neoplasms; prevalence of childhood cancer; and individual tumours and their distribution according to age, sex, ethnicity and geographical area. It is used to assess subtype, stages of malignancies, and their outcomes in children. The collected information can assist in scientific analysis, planning and research.
The data collected in a hospital-based registry are: demographic information (name, age, sex, and address); tumour type, localisation and stage; histological type; treatment and outcome; and yearly follow-up results. Data should include the date and cause of death, if the patient died.5
Data are presented regularly at national and international meetings, and are used in Master's dissertations or to provide information for analysis of specific tumours in different regions of the country. Data are accessible to all collaborating paediatric centres and released on written request to paediatric oncologists or other doctors working in the units.
Registry results
The Registry does not require substantial expenditure; it started and existed for more than 20 years without any financial support. The Childhood Cancer Foundation of South Africa has covered the Registry's costs during the last 3 years, including salaries of 3 parttime data capturers and a data manager; R30 000 for a computer, printer and scanner; and the data capturers' training. The costs of the data capturers and data manager are currently R13 600 monthly.
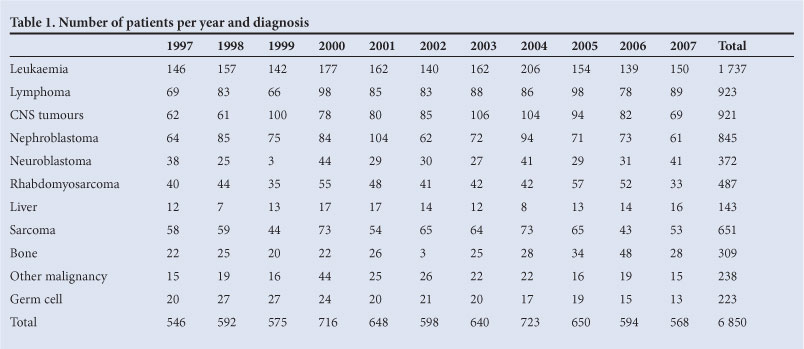
Table 1 shows the childhood cancers recorded in the Registry from 1997 to 2007 by year and tumour type. The annual incidence of tumours in South African children aged 0 - 14 years varied between 33.4 and 47.2 per million from 2003 to 2007, which is much lower than in the USA or Europe. In Europe, the annual incidence of cancer in this age group was 140 per million in 1990, increasing by 1% per year for the last 3 decades. This marked discrepancy is probably related to several factors, including failure to diagnose cancers, lack of referrals to oncology units, and failure to report them to the Registry.
In South Africa, leukaemia is the most common childhood cancer (25.4% of all cancers), which is similar to rates in other countries. While brain tumours and leukaemia comprise almost half of childhood cancers in developed countries, brain tumours represent only 13.4% of the total cancers diagnosed in children in South Africa.
This discrepancy can be explained by failure to consider or make the diagnosis, especially in smaller and rural hospitals.
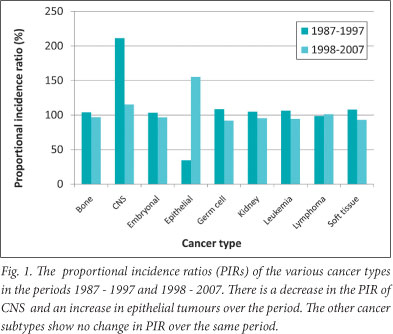
Fig. 1 shows the distribution of the various childhood cancers for 2 10-year periods. When these 2 periods are compared, the number of brain tumours decreased by half while epithelial tumours doubled, almost exclusively owing to the rising incidence of Kaposi's sarcoma.
National Cancer Registry
Until April 2011, the Registry was the main source of statistical data for epidemiological studies in this field. An alternative source of cancer information was the National Cancer Registry, a pathologybased registry of the National Health Laboratory Service, established in 1986. However, this source had shortcomings regarding children's cancer: an unknown number of cases were not registered as they were diagnosed clinically, sometimes assisted by identifying tumour markers (e.g. hepatocellular carcinoma); and children were on the same register as adults (child-specific data may be missed). Clinical data were seldom communicated in full to the laboratories. Over time, many private laboratories discontinued contributing to the Register for fear of consequences arising from disclosure of information that might be private and confidential.6
Plans to revitalise the National Cancer Registry, initiated by the Department of Health, were finalised on 26 April 2011 with Government Notice No. R.380, which introduced new regulations in terms of the National Health Act, 2003 (Act No. 61 of 2003). All cancers in children and adults have to be reported to the National Cancer Registry. 'The person in charge of a health establishment, where diagnosis is confirmed, must ensure that Annexure A is completed and submitted to the NCR within 3 months of diagnosis.' Further, 'The head of a laboratory must, on a quarterly basis, ensure that Annexure A, as well as the accompanying laboratory report, is completed and submitted to the NCR.' The regulations stipulate that a population-based cancer registry will be established incrementally.
Conclusion
The SACCSG regards the Department of Health's decision as an important step towards better understanding of the burden of disease owing to cancer and taking appropriate measures at national level to improve its management. Paediatric oncologists fully support the National Cancer Registry and report cases as requested. Nevertheless, we believe that the Registry remains a useful and significant repository for specific paediatric data that will, along with the National Cancer Registry, adequately address the needs of researchers in paediatric oncology.
1. Stiller CA, Parkin DM. Geographic and ethnic variations in the incidence of childhood cancer. Br Med Bulletin 1996;52(2):682-703. [ Links ]
2. Kellie SJ, Howard SC. Global child health priorities: what role for paediatric oncologists? Eur J Cancer 2008;44(16):2388-2396. [Epub 15 September 2008]. [ Links ]
3. Statistics South Africa. Mid-year population estimates, 2009. http://www.statssa.gov.za/publications/statspastfuture.asp?PPN=P0302&SCH=781 (accessed 24 February 2010). [ Links ]
4. International Association of Cancer Registries. Membership list. http://www.iarc.com.fr (accessed 25 February 2010). [ Links ]
5. Young JL. The Hospital Based Tumor Registry. In: Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG, eds. Cancer Registration Principles and Methods. Lyons: IACR Publications, 2006. [ Links ]
6. National Health Laboratory Service. National Cancer Registry. http://www.nhls.ac.za/div_ncr.html (accessed 25 February 2010). [ Links ]
Corresponding author: D Stones (StonesDK@ufs.co.za)


{kind=link}