










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.102 n.6 Pretoria Jun. 2012
FORUM
REFLECTIONS
Anaesthesia - what has the University of Cape Town contributed?
Jennifer M ThomasI, II; Anthony R ReedI; Peter C GordonI, III; Robert A DyerI, IV; Michael F JamesI, V
IAll authors hail from the Department of Anaesthesia, Faculty of Health Sciences, University of Cape Town
IIProfessor Jenny Thomas is Head of Anaesthesia at Red Cross War Memorial Children's Hospital. Dr Anthony Reed is Head of Anaesthesia at New Somerset Hospital
IIIAssociate Professor Peter Gordon recently retired as Head of Clinical Services at Groote Schuur Hospital and is the archivist of the SA Society of Anaesthesiologists
IVProfessor Robert Dyer is the 2nd Chair of Anaesthesia
VEmeritus Professor Michael James, recently retired as Chair of Anaesthesia and Head of Department
ABSTRACT
From humble beginnings, the Department of Anaesthesia of the University of Cape Town has played a major role in the development of anaesthesia as a speciality, in South Africa and internationally. We highlight these contributions in clinical service, teaching and research, with particular emphasis on the department's leading role in the evolution of anaesthetic safety in adults and children: from the development of the treatment of malignant hyperthermia, to unique studies in mortality associated with anaesthesia, and modern contributions to improved drug safety. Innovations in anaesthetic techniques have contributed to significant surgical developments, including the first heart transplant. Furthermore, our research has contributed to major advances in obstetric and endocrine anaesthesia, and training in the department is recognised as being among the best in the world.
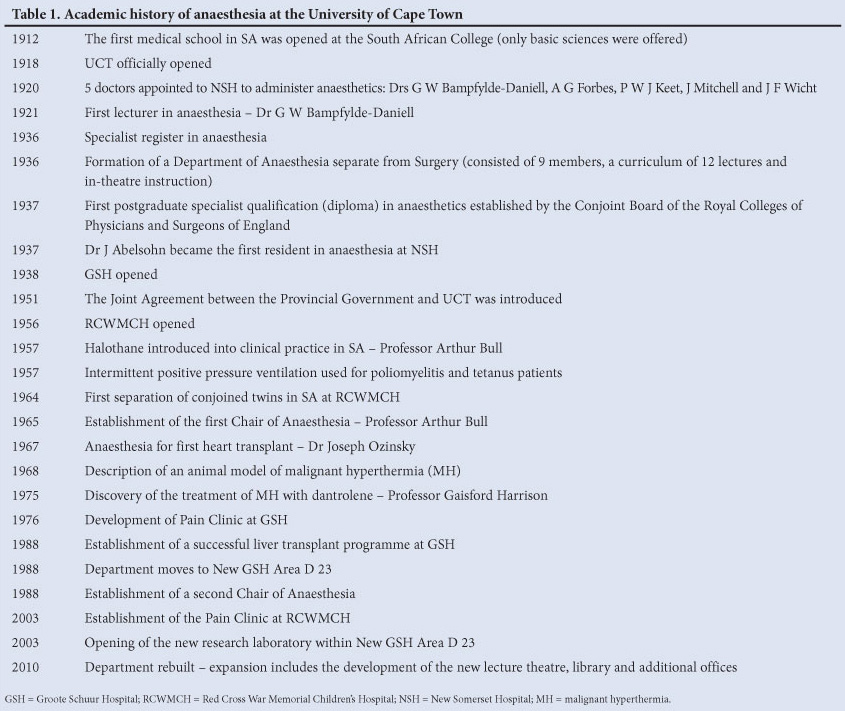
Over the past 100 years, the specialty of anaesthesia has evolved from a 'rag and bottle' administration of chloroform/ether, with minimal monitoring and little formalised teaching and training, to that of extreme sophistication and safety. Spectacular advances in anaesthetic equipment and pharmacology have been seen in the past 50 years; specialist training has advanced the discipline and allowed the development of far more complex and higher risk surgery. The history of anaesthesia in South Africa (SA) is well captured in the Nagin Parbhoo History of Anaesthesia Museum, housed in the Department of Anaesthesia at Groote Schuur Hospital (GSH).
The department originated in Somerset Hospital, moved to GSH in 1938 and gradually expanded over the years to include New Somerset Hospital (NSH), Red Cross War Memorial Children's Hospital (RCWMCH), Mowbray Maternity Hospital and others (Table 1).
Prior to the establishment of the SA specialist qualification, doctors wishing to specialise were required to travel to the United Kingdom, Ireland or the USA. In 1952 the SA Society of Anaesthetists strongly supported the formation of a Faculty of Anaesthesia within the proposed College of Medicine of SA. The College was established in 1954 and the Faculty of Anaesthetists shortly thereafter. The first successful individuals to qualify as specialists from the University of Cape Town (UCT) graduated in 1955. Early in the College's history, Jack Abelsohn donated a sum of money for an award to the best candidate in the clinical part of the final Fellowship - the prize is still awarded today. Since then, UCT has played a prominent role in the Faculty and was one of the prime movers in the development of a semi-independent College of Anaesthetists within the reconstituted Colleges of Medicine of SA. Numerous UCT individuals have functioned as president of the Faculty and subsequently the College.
Anaesthesia specialisation now requires 4 years of certified registrar training in an appropriate institution, a Fellowship of the College of Anaesthetists of SA, or equivalent, and an MMed degree.
Safety in anaesthesia
Patients requiring surgery in the 21st century expect to survive the operation. Only 50 years ago this was not the case. The world's longest longitudinal study into anaesthetic mortality over 3 decades was undertaken at UCT between 1956 and 1987; this landmark study documented a decrease in death attributable to anaesthesia at GSH, from 3.3/10 000 anaesthetics in 1956 - 1965, to fewer than 1/10 000 between 1977 and 1987.1 The reduction in mortality can be attributed to numerous factors including:
(i) improved monitoring of patient physiological status and equipment such as ventilators
(ii) the establishment of recovery rooms, allowing surgery in sicker patients and postoperative stabilisation before return to the ward
(iii) advances in anaesthetic training and expertise
(iv) the development of intensive care units with multidisciplinary medical staff, including anaesthetists who applied protocols and practices that formed the basis of critical care medicine
(v) the development of shorter-acting, less toxic and more predictable drugs leading to more rapid emergence from anaesthesia and a decrease in postoperative complications
(vi) improved acute pain management with regional anaesthetic techniques, multimodal anaesthesia and patient-controlled anaesthesia equipment
(vii) good clinical skills and vigilance, as confirmed by Dr Joseph Ozinsky's anaesthetic technique for the world's first human-to-human heart transplant operation; the technique was performed safely without the monitoring and drugs regarded as essential for cardiac surgery today
(viii) the development of sub-specialties in anaesthesia, such as paediatric, cardiothoracic and obstetric anaesthesia.
These advances went hand-in-hand with the establishment of pioneering national and international organ transplant programmes for heart, kidney and liver transplants in Cape Town. This necessitated improved anaesthetic skills to provide peri-operative care and anaesthesia for critically ill transplant recipients (adult and paediatric). The liver transplantation programme, regarded by many as inappropriate for the SA environment, proved to be extremely successful in both adult and paediatric patients. Further positive benefits included the acquisition of point-of-care equipment in theatre, such as thrombelastography and blood gas analysers.
In January 2008 one of the authors (PG) attended the World Health Organization (WHO) meeting to finalise the Surgical Safety Check List (SSCL). The check-list was implemented at GSH and across the Western Cape (WC) province, and was recently adopted as a national core standard for hospitals by the national Department of Health (DoH).
In 2006 the WC DoH initiated a system of co-ordinating clinicians for major disciplines. In this role, one author (AR) was able to assess anaesthetic services in hospitals across the province. For many district hospitals, this was the first opportunity to gain access to support from the resource of specialists in the province. Together with a Provincial Anaesthetic Coordinating Committee, an opportunity was created for specialist practitioners to support services provided by medical officers, resulting in an improvement in the quality of equipment and standards of anaesthetic practice in district hospitals. This has enormous potential to expand the UCT teaching platform to a more appropriate level for undergraduate training.
Research and development
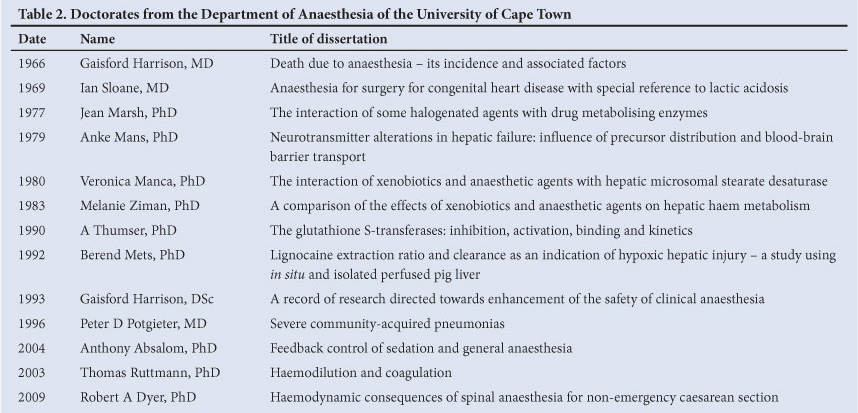
The department has played a leading role in anaesthetic research, producing 13 doctoral degrees (Table 2), approximately 800 peer-reviewed papers and international book chapters, and an international text book.
As an evolving specialty, research in anaesthesia has played a major role. In 1965 - 1967 the Taurus blood warmer - named after Professor Bull - to prevent hypothermia after major blood transfusion was developed.2 This device, still in use today, was one of the first to use radiofrequency induction heating technology. The pressure-cycled Bird ventilator was modified for use in both paediatric and adult anaesthesia.3 Many other innovative modifications of anaesthetic equipment followed to render them safe for use in children.
Research on malignant hyperthermia (MH) put the department on the world stage. A porcine model of MH enabled elucidation of the pathophysiology of this condition in conjunction with the Department of Chemical Pathology.4 Later it was demonstrated that the intravenous use of dantrolene was life-saving in treatment of this previously fatal metabolic storm.5
Much of the current safe practice in porphyria, particularly the pharmacological management of affected individuals, stemmed from work on liver transplantation performed in the animal laboratory at UCT; anaesthetists were part of the multidisciplinary research team.
In the field of critical care, research contributions included the control of infection, severity scoring in sepsis, treatment of various types of poisoning and new ventilator techniques for the critically ill.6,7
Magnesium was established as the treatment of choice for the control of hypertensive response to tracheal intubation in pre-eclampsia,8 haemodynamic instability in tetanus and in the peri-operative management of phaeochromocytoma.9 The first double-blinded randomised comparison of crystalloids versus colloids for resuscitation in trauma was the product of many years of research in the field of fluid management.10 Landmark studies were published on the role of fluid therapy in coagulation.11
The department's specialist interest in obstetric anaesthesia has resulted in many research publications, covering various aspects of spinal anaesthesia for caesarean section. Particular areas of importance are fluid management,12 the haemodynamic effects of vasopressors and oxytocin in healthy and pre-eclamptic patients,13,14 and neonatal outcomes. There is on-going international collaboration in this field.
Landmark studies on drug safety and errors in anaesthesia culminated in the first prospective multicentre study of drug administration errors in anaesthesia in SA.15
Research in paediatric anaesthesia at RCWMCH in the management of conjoined twins,16 and of the burned child, has gained international recognition. Numerous other projects are underway involving pain management, coagulation studies in burn patients, and antibiotic pharmacokinetics in children undergoing cardiac surgery.
The focus of the laboratory of the department has changed from primarily animal-based research in the period 1965 - 1970s to pharmacological studies using the department's gas chromatography laboratory in the 1970s - 1980s. The opening of the department's thrombelastography laboratory in the mid-1990s led to significant contributions in the field of coagulation.
National leadership
Many members of the department have played significant leadership roles within the anaesthetic community in SA, predominantly through the Colleges of Medicine and the SA Society of Anaesthesiologists (SASA). The following members of the department served as president of SASA: Royden Muir, Thomas Fuller, Jack Abelsohn, Eric van Hoogstraten, 'Buck' Jones, Arthur Bull, David Morrell, Peter
Gordon, David Linton and Michael James. A former member of the department, Professor David Morrell, served as president of the Colleges of Medicine of SA.
Teaching and training
Prior to the introduction of the community service medical officer (COSMO) year of medical practice in SA, anaesthesia training at UCT was regarded primarily as a postgraduate specialty. In the 6-year medical school curriculum, only a 2-week period was allocated to anaesthesia. The need for COSMOs to provide a safe anaesthetic service with limited supervision, particularly for caesarean sections in rural areas, has led to a major revision of the curriculum in anaesthesia offered to students. There is a more extensive undergraduate experiential training in anaesthesia, in the 4th and 5th years, and the 2-year internship now includes 2 months of anaesthetic training.
The department has an excellent record in teaching and training: 2 colleagues are the recipients of the UCT Distinguished Teacher award; our post-graduate students have an enviable record of success at the College examinations, with many obtaining prizes in the primary and final fellowship examinations.
Pain Clinic
In 1976, together with the Department of Neurosurgery, a multidisciplinary chronic pain clinic was formed at GSH. Originally dealing with cancer pain, the clinic soon attracted patients with pain of multiple aetiologies. The clinic's current director is an anaesthetist.
Red Cross War Memorial Children's Hospital
An anaesthetic service at the new RCWMCH was set up in 1956, under Dr Arthur Bull. Use of the new inhalational agent, halothane, occurred in the following year. During the polio epidemic in 1956/7, positive pressure ventilation was introduced. Subsequently, use of curare for the ventilation of infants with tetanus reduced mortality from 90% to 20%, and later to 10%.
Safe and paediatric-appropriate anaesthetic equipment was developed at RCWMCH and many adaptations to conventional adult equipment undertaken to facilitate safer paediatric anaesthesia have only recently been superseded. The anaesthetic management of conjoined twins is internationally renowned.
Conclusion
The UCT Department of Anaesthesia has grown enormously from an ancillary section of the Department of Surgery to a sturdy, independent department with a strong teaching and research record. The enormous demand for admission to our postgraduate programmes from doctors of a very high standard, together with a new leadership structure, presages a future of even greater promise for this proud organisation.
Acknowledgements
This article would not have been possible without extensive use of the works of Dr Nagin Parbhoo.17,18
References
1. Harrison GG. Anaesthetic contributory death - its incidence and causes. S Afr Med J 1968;42:544-549. [ Links ]
2. Du Plessis JM, Bull AB, Besseling JL. An assessment of radio frequency induction heating of blood for massive transfusion. Anesth Analg 1967;46:96-100. [ Links ]
3. Voss TJ. The adaptation of ventilators for anesthesia, with particular reference to paediatric anaesthesia. S Afr Med J 1967;41:1079-1082. [ Links ]
4. Harrison GG, Saunders SJ, Biebuyck JF, et al. Anaesthetic-induced malignant hyperpyrexia and a method for its prediction. Br J Anaesth 1969;4:844-855. [ Links ]
5. Harrison GG. Control of the malignant hyperpyrexic syndrome in MHS swine by dantrolene sodium. Br J Anaesth 1975;47:62-65. [ Links ]
6. Potgieter PD, Hammond JM. The intensive care management, mortality and prognostic indicators in severe community-acquired pneumococcal pneumonia. Intensive Care Med 1996;22:1301-1306. [ Links ]
7. Linton DM, Potgieter PD, Davis S, Fourie AT, Brunner JX, Laubscher TP. Automatic weaning from mechanical ventilation using an adaptive lung ventilation controller. Chest 1994;106:1843-1850. [ Links ]
8. James MF. Magnesium in obstetrics. Best Pract Res Clin Obstet Gynaecol 2010;24(3):327-337. [ Links ]
9. James MF, Cronje L. Pheochromocytoma crisis: the use of magnesium sulfate. Anesth Analg 2004;99:680-686. [ Links ]
10. James MF, Michell WL, Joubert IA, Nicol AJ, Navsaria PH, Gillespie RS. Resuscitation with hydroxyethyl starch improves renal function and lactate clearance in penetrating trauma in a randomized controlled study: the FIRST trial (Fluids in Resuscitation of Severe Trauma). Br J Anaesth 2011;107(5):693-702. [ Links ]
11. Ruttmann TG, James MF, Aronson I. In vivo investigation into the effects of haemodilution with hydroxyethyl starch (200/0.5) and normal saline on coagulation. Br J Anaesth 1998;80(5):612-616. [ Links ]
12. Dyer RA, Farina Z, Joubert IA, et al. Crystalloid preload versus rapid crystalloid administration after induction of spinal anaesthesia (coload) for elective caesarean section. Anaesth Intensive Care 2004;32:351-357. [ Links ]
13. Dyer RA, Reed AR, van Dyk D, et al. Hemodynamic effects of ephedrine, phenylephrine, and the coadministration of phenylephrine with oxytocin during spinal anesthesia for elective cesarean delivery. Anesthesiology 2009;111:753-765. [ Links ]
14. Dyer RA, Piercy JL, Reed AR, Lombard CJ, Schoeman LK, James MF. Hemodynamic changes associated with spinal anesthesia for cesarean delivery in severe preeclampsia. Anesthesiology 2008;108:802-811. [ Links ]
15. Llewellyn RL, Gordon PC, Wheatcroft D, et al. Drug administration errors: a prospective survey from three South African teaching hospitals. Anaesth Intensive Care 2009;37:93-98. [ Links ]
16. Thomas JM, Lopez JT. Conjoined twins - the anaesthetic management of 15 sets from 1991-2002. Paediatr Anaes 2004;14(2):117-129. [ Links ]
17. Parbhoo N. The Department of Anaesthesia, UCT 1920-2000. MD Thesis, University of Cape Town, 2002. [ Links ]
18. Parbhoo N. Five Decades, the South African Society of Anaesthetists 1943-1993. Cape Town: National Book Printers, 1993. [ Links ]
Accepted 22 March 2012.
Corresponding author: P C Gordon (peter.gordon@uct.ac.za)


{kind=link}
{kind=link}