










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.12 Pretoria dic. 2011
ORIGINAL ARTICLES
Acute renal failure in four Comrades Marathon runners ingesting the same electrolyte supplement: coincidence or causation?
Jeremy BoulterI; Timothy D NoakesII; Tamara Hew-ButlerIII
IMB ChB. Medical Team, Comrades Marathon, Scottsville, KwaZulu-Natal
IIMB ChB, MD, DSc. Medical Research Council/University of Cape Town Research Unit for Exercise Science and Sports Medicine, Department of Human Biology, University of Cape Town
IIIDPM, PhD. School of Health Science, Oakland University, Rochester, MI, USA
ABSTRACT
OBJECTIVES: To evaluate common factors associated with the development of acute renal failure (ARF) in Comrades Marathon runners.
METHODS: This was a retrospective case series of 4 runners hospitalised post-race with ARF in the 89 km 2010 Comrades Marathon. The outcome measures were incidence of analgesic use, levels of creatine phosphokinase (CPK) and degree of electrolyte supplementation (sodium, potassium, calcium and magnesium).
RESULTS: The prevalence of ARF was 1/4 125 runners. They presented with rhabdomyolysis (mean admission CPK of 36 294 IU) and hyponatraemia (mean admission blood sodium level of 133 mEq/l). All had ingested an analgesic during the run (3 ingested a non-steroidal anti-inflammatory drug) and the same readily available anti-cramp electrolyte supplement. The average amount of supplemental sodium (452 mg), potassium (393 mg), calcium (330 mg) and magnesium (154 mg) ingested via this particular electrolyte supplement before and during the run did not exceed the recommended upper limits of daily intake. Three of the runners were Comrades Marathon novices.
CONCLUSIONS: There is a continuing need to clarify the specific cluster variants that cause ARF in Comrades Marathon runners, as the risk factors appear to have evolved since the first case was described over 40 years ago.
The 89 km Comrades Marathon historically reports the highest incidence of acute renal failure (ARF) cases in any sporting event in the world (estimated at 2/10 000 runners).1 The first 2 cases reported from the event (in 1967 and 1968) occurred in races with only ~600 runners.2 An incidence as high as 10/10 000 runners was reported in the 1986 Comrades Marathon.1 The spectrum of reported cases from this ultramarathon has ranged from unrecognised ARF that persisted for 10 days post-race3 to significant renal damage requiring extended hospitalisation and peritoneal dialysis.4 Aetiology factors proposed include dehydration secondary to inadequate fluid intake and/or diarrhoea or vomiting,1,2,4,5 rhabdomyolysis2,6 and analgesic use including paracetomol4 and non-steroidal anti-inflammatory drugs (NSAIDs).5
Forty years after the first description of ARF in Comrades Marathon runners,2 we report a cluster of 4 cases that occurred in the 2010 Comrades Marathon, and analyse possible causative factors.
Methods
Four runners identified with ARF following their participation in the 2010 Comrades Marathon were brought to the attention of the event's Chief Medical Officer (JB) by the head trauma unit physician at St Augustine's Hospital, Durban - the referral hospital for the event in 2010. Verbal and written consent for the release of all hospital medical records was obtained from the runners by the first author in his capacity as Chief Medical Officer. He interviewed each runner within 2 weeks of hospital release about their medical history, running history, prior injuries, supplement and medication intake (before, during and after the run), and symptoms encountered during and after the race.
Results
Of 16 500 participants, 14 343 completed the 89.3 km 2010 Comrades Marathon under the 12 hour cut-off (80% male; 26% novices). The average temperature in Durban was 19ºC (min 14ºC; max 24ºC) with 63% humidity and 3 km/h wind speed.
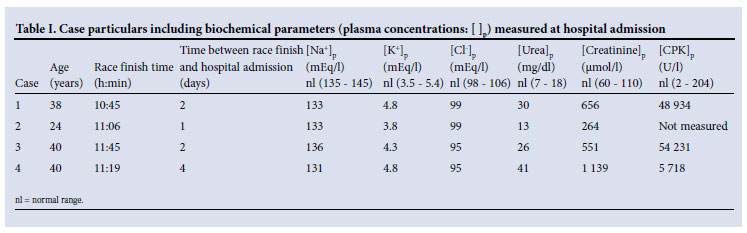
The average age of the 4 runners who developed ARF was 35±6 years (mean ± SD) and their average finish time was 673±25 minutes. All 4 runners were male. They did not present to the medical tent at the race finish but became symptomatic 1 - 4 days post-race when hospitalised for management of ARF in the same local hospital. The exact incidence of ARF in finishers and non-finishers is unknown owing to the difficulty of tracking hospitalisations once runners leave the local area (Durban through Pietermaritzburg). Initial blood samples taken on hospital admission (Table I) showed that 3 of the runners were hyponatraemic (blood sodium concentrations <135 mEq/l), and 2 were hypochloraemic (blood chloride concentrations <98 mEq/l). Blood urea, creatinine and creatine phosphokinase (CPK) concentrations were elevated. Blood calcium concentrations were not measured.
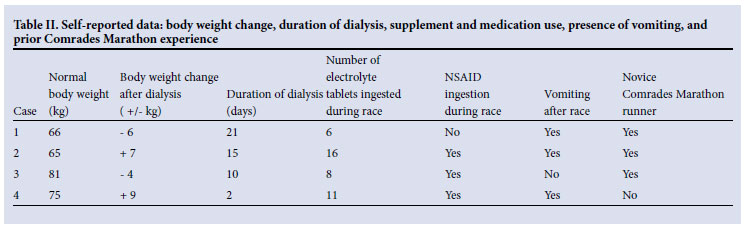
All 4 athletes reported that they ingested the same readily available anti-cramp electrolyte supplement during the race; the estimated range of tablets ingested on race day varied from 6 to 16 tablets, with an average intake of 11 tablets (1 per hour) (Table II). Three runners ingested NSAIDs during the race, while patient 1 ingested an analgesic/muscle relaxant (Besemax; 450 mg paracetamol and 35 mg orphenadrine citrate) during and Voltaren (NSAID) prior to the race for a knee injury. Three of the 4 runners reported vomiting in the period between race finish and hospital admission, while patient 3 reported developing nausea. Three of the runners were Comrades Marathon novices. Patient 4 was running his 7th Comrades Marathon, but his training had been curtailed in the 2 months before the race, owing to a significant running injury (shin splints) and surgery for haemorrhoids.
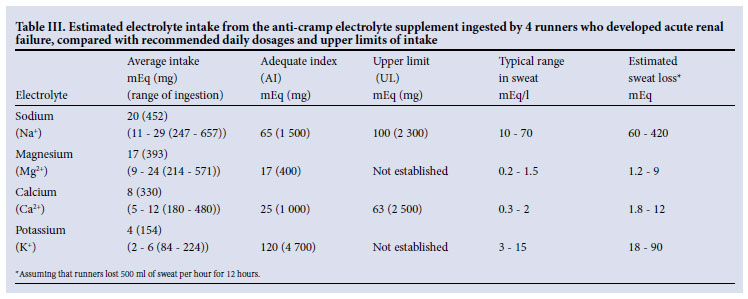
The estimated average and range of sodium, magnesium, calcium and potassium intake obtained via ingestion of the electrolyte supplement common to the runners is compared with adequate daily intake (AI), upper limit of intake (UL) and estimated electrolyte sweat loss in Table III.
Discussion
This case series details the development of ARF in 4 male runners following completion of the 2010 Comrades Marathon, requiring hospitalisation and acute renal dialysis. More of the 16 500 race participants might have developed ARF; cases might have been undetected if the affected runners did not live in the catchment area surveyed by the Chief Medical Officer. The minimum prevalence of ARF in the 2010 Comrades Marathon was therefore 1/4 125 runners; this is an unusually high incidence compared with previous marathon years ('typical' incidence was 1/10 000 runners).1
Factors known to be associated with ARF include rhabdomyolysis with elevated serum CPK usually in excess of 20 000 IU, although no clearly defined CPK 'threshold' exists where the risk of ARF is markedly increased.7 We previously described mean CPK values of between 637 and 1 878 IU in asymptomatic Comrades Marathon runners;8,9 the high values between 5 718 and 54 231 IU measured in the present cluster of runners with ARF appeared to be far above the normal range of healthy runners, indicative of marked rhabdomyolysis (Table I).
Exercise-induced rhabdomyolysis - with mean CPK values exceeding 40 000 IU in: (i) 35 patients admitted to hospital with a primary or secondary diagnosis of rhabdomyolysis;10 and (ii) 39 runners finishing a 246 km race11 - has not been shown to be diagnostic of impending renal failure. No cases of ARF were documented in either of the aforementioned studies despite the high CPK levels mimicking that of 2 of the 4 Comrades runners with ARF in the present study. On the other hand, because CPK levels were not measured pre-race, we cannot rule out the presence (or absence) of undiagnosed subclinical metabolic myopathies in this cluster. McArdle's syndrome, carnitine palmitoyltransferase deficiency, Becker's syndrome, and disorders of caveolin-3 may be 'silent myopathies' that only present with symptoms and elevated CPK levels following exercise.12
A second factor associated with ARF in endurance athletes is NSAID use, which was previously found in 79 - 80% of ARF cases in endurance athletes.4,13 Three of the 4 runners in the present study ingested NSAIDs during the 2010 Comrades Marathon: patients 2 and 4 ingested 2 and 7 Cataflam tablets respectively; and patient 3 ingested 3 Myprodol tablets. Patient 1 ingested 2 Besemax tablets during the race, as well as Voltaren for 1 week before the race to treat a knee injury. It is unclear what percentage of the 14 343 race finishers ingested NSAIDs during the race. An electronic survey of 2010 Comrades Marathon participants showed that only ~6% of 3 367 respondents indicated NSAID use either before or during the race (S. Rorke, personal communication). The much higher incidence of NSAID use in the runners who developed ARF compared with that of a 'control' group in the same race supports the role of NSAIDs as a clear ARF risk factor - even at mild non-prescription dosages. Investigations have confirmed significant changes in renal dynamics following ibuprofen ingestion.14
A third factor associated with the development of ARF is exerciseassociated hyponatraemia (EAH), as recently shown in clusters of runners following 153 km and 161 km footraces.13,15 It has been postulated that cell swelling associated with EAH destabilises muscle cell membranes, making them less resistant to (traumatic) rupture. The proposed fragility of 'swollen' muscle cells then facilitates muscle breakdown, rhabdomyolysis and myoglobin release, leading to the development of ARF.13,15
All 4 of the described runners were hyponatraemic on presentation to hospital 1 - 4 days after the race finish. This is probably the result of ARF, which can produce a dilutional hyponatraemia secondary to protracted anuria/oliguria.16 Serum sodium concentrations were not measured at the race finish; therefore it is unclear whether the documented hyponatraemia was either a cause or an effect of the exercise-associated ARF.
Curiously, all 4 runners ingested the same commercially available electrolyte supplement marketed to prevent muscle cramps during exercise. None of them had previously taken this supplement. One serving size (2 tablets) (Table III) provides 300 mg of sodium bicarbonate, 250 mg of magnesium carbonate, 150 mg of calcium carbonate, 50 mg of potassium phosphate plus trace amounts of taurine (100 mg) and vitamin B6 (5 mg). The recommended product dosage was ingestion of 2 tablets 30 minutes before the start of the event, followed by 1 tablet each hour of exercise. Of the 4 electrolytes present in the supplement, sodium, potassium and calcium are the most likely to contribute to renal dysfunction.
Sodium depletion, rather than supplementation, contributes to renal compromise via subsequent development of hyponatraemia, with or without volume depletion.17 It is unlikely that the supplemental sodium associated with ingestion of the described supplement contributed to the development of ARF or prevented the development of hyponatraemia in the 4 ARF patients. Furthermore, the absence of hyperkalaemia does not support excessive potassium ingestion as a contributing factor towards their development of ARF.
In contrast, the ingestion of large amounts of calcium plus absorbable alkali ('milk-alkali syndrome') (MAS) is a well-known cause of renal failure.18 MAS is characterised by hypercalcaemia and results from sustained intake of excessive amounts of calcium carbonate (~4 - 5 g per day).18 It appears unlikely that the amount of calcium carbonate ingested via the described electrolyte supplement - even in the highest self-reported dosage - could have contributed significantly to the development of ARF (Table III). Unfortunately, blood calcium concentrations were not measured in any of the affected runners.
Conclusions
It appears that NSAID ingestion during the Comrades Marathon in runners with an (as yet) unidentified susceptibility produced rhabdomyolysis and ARF. Unexpectedly, all 4 runners ingested a specific anti-cramp electrolyte-containing supplement. The number of runners in the race who ingested this or similar supplements is unknown; however, this finding suggests that caution should be advised regarding liberal use of the product during prolonged exercise, despite ingested doses not reaching 'toxic' dosages, based on current AI or UL recommendations.19 There is a continuing need to determine the combination of factors which caused ARF to develop uniquely in only 4/16 500 runners. Accordingly, a better tracking system for reporting future adverse events should be implemented.
References
1. Irving RA, Noakes TD, Raine RI, van Zyl SR. Transient oliguria with renal tubular dysfunction after a 90 km running race. Med Sci Sports Exerc 1990;22:756-761. [ Links ]
2. Dancaster CP, Duckworth WC, Roper CJ. Nephropathy in marathon runners. S Afr Med J 1969;43(24): 758-760. [ Links ]
3. Zyl-Smit R, Mills P, Vogelpoel L. Unrecognized acute renal failure following the comrades marathon. S Afr Med J 2000;90:39-40. [ Links ]
4. MacSearraigh ET, Kallmeyer JC, Schiff HB. Acute renal failure in marathon runners. Nephron 1979;24:236-240. [ Links ]
5. Seedat YK, Aboo N, Naicker S, Parsoo I. Acute renal failure in the "Comrades Marathon" runners. Ren Fail 1990;11:209-212. [ Links ]
6. Schiff HB, MacSearraigh ET, Kallmeyer JC. Myoglobinuria, rhabdomyolysis and marathon running. QJM 1978;47:463-472. [ Links ]
7. Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med 2009;361:62-72. [ Links ]
8. Strachan AF, Noakes TD, Kotzenberg G, Nel AE, de Beer FC. C reactive protein concentrations during long distance running. BMJ (Clin Res Ed) 1984;289:1249-1251. [ Links ]
9. Noakes TD, Kotzenberg G, McArthur PS, Dykman J. Elevated serum creatine kinase MB and creatine kinase BB-isoenzyme fractions after ultra-marathon running. Eur J Appl Physiol 1983;52:75-79. [ Links ]
10. Sinert R, Kohl L, Rainone T, Scalea T. Exercise-induced rhabdomyolysis. Ann Emerg Med 1994;23:1301-1306. [ Links ]
11. Skenderi KP, Kavouras SA, Anastasiou CA, Yiannakouris N, Matalas AL. Exertional rhabdomyolysis during a 246-km continuous running race. Med Sci Sports Exerc 2006;38:1054-1057. [ Links ]
12. Bracaccio P, Maffuli N, Limongelli FM. Creatine kinase monitoring in sport medicine. Br Med Bull 2007;81/82:209-230. [ Links ]
13. Bruso JR, Hoffman MD, Rogers IR, Lee L, Towle G, Hew-Butler T. Rhabdomyolysis and hyponatremia: a cluster of five cases at the 161-km 2009 Western States Endurance Run. Wilderness Environ Med 2010;21:303-308. [ Links ]
14. Walker RJ, Fawcett JP, Flannery EM, Gerrard DF. Indomethacin potentiates exercise-induced reduction in renal hemodynamics in athletes. Med Sci Sports Exerc 1994;26:1302-1306. [ Links ]
15. Ellis C, Cuthill J, Hew-Butler T, George SM, Rosner MH. Exercise-associated hyponatremia with rhabdomyolysis during endurance exercise. Phys Sportsmed 2009;37:126-132. [ Links ]
16. Verbalis JG, Goldsmith SR, Greenberg A, Schrier RW, Sterns RH. Hyponatremia treatment guidelines 2007: expert panel recommendations. Am J Med 2007;120:S1-S21. [ Links ]
17. Knapp MS. Saline depletion, pre-renal failure and acute renal failure. Clinics in Endocrinology and Metabolism 1984;13:311-332. [ Links ]
18. Medarov BI. Milk-alkali syndrome. Mayo Clin Proc 2009;84:261-267. [ Links ]
19. Hew-Butler T. Electrolytes. In: Mooren FC, Skinner JS, eds. Encyclopedia of Exercise Medicine in Health and Disease. DOI 10.1007/978-3-540-29807-6 ed. Berlin: Springer-Verlag, 2011. [ Links ]
Accepted 17 October 2011.
Corresponding author: T Hew-Butler (hew@oakland.edu)


{kind=link}
{kind=link}
{kind=link}