










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 n.9 Pretoria Sep. 2011
FORUM
HISTORY OF MEDICINE
Akhenaten, a unique pharaoh
François Pieter Retief; Louise Cilliers
Akhenaten was a unique pharaoh in more ways than one. He initiated a major socio-religious revolution that had vast consequences for his country, and possessed a strikingly abnormal physiognomy that was of note in his time and has interested historians up to the present era. In this study, we attempt to identify the developmental disorder responsible for his eunuchoid appearance.
Akhenaten, the Pharaoh (Dynasty 18,1350 - 1334 BC, New Kingdom)1,2
Amenotep IV (Akhenaten) succeeded his father, Amenotep III, after a particularly prosperous and peaceful reign of nearly 40 years. He was hidden from public scrutiny for a good part of his father's reign, perhaps because of his curious appearance. It is possible that he was co-regent with his father for a few years. Amenotep III had begun to find the polytheistic priesthood of Amun restrictive on his reign and initiated early measures to curb them. His son was to extend this considerably. He began his movement towards the institution of a monotheistic religion centred on Aten, the sungod, by building him a temple outside the Amun temple complex at Karnak (Thebes). The sungod already formed an important component of the Amun godhead complex as Amen-Re or Re-Hanakhte. It was soon clear that the two cults could not survive together. Proving himself more of a philosopher and thinker than his forebears, Amenotep IV changed his name to Akhenaten (Servant of Aten) in his 5th or 6th regnal year, and started closing the temples of Amun and prosecuting its priesthood. At the same time, he proceeded to move his capital from Thebes to halfway down the Nile at Memphis, which he called Akhetaten (Horizon of Aten) - today called el-Amarna.
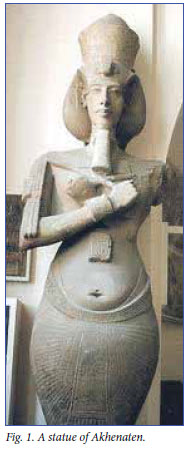
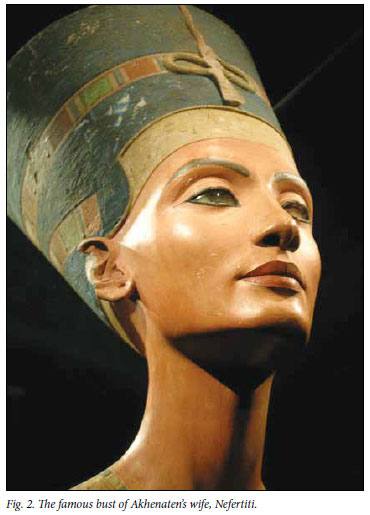
Akhetaten, constructed on a stretch of virgin soil, and about 6 km x 4 km in size, was predominantly on the eastern Nile bank and gave the impression of a garden city with extensive palaces, temples for Aten, living quarters for the aristocracy, and ceremonial graves excavated into the cliffs to the east. Modern archaeology reveals evidence of hasty but shoddy workmanship. Artists were encouraged to emulate what they saw, rather than reproducing human stereotypes typical of the past. The pharaoh's curious physique was represented in various statues and reliefs (Fig. 1); it even became fashionable to emulate the pharaoh's elongated limbs in statues of other members of the royal family. The most famous sculpture of his queen, Nefertiti, shows her with an elongated neck (Fig. 2). The realistic art of the era became known as 'Amarna art' (after the city). Akhenaten also encouraged literature, and it is thought that he was the author of the extraordinary Hymn to the Aten - in which some authorities see a resemblance to Psalm 104 from the Bible. The 'Amarna letter' shows evidence of extensive correspondence with foreign kings in the Middle East. State administration and foreign affairs were largely left to viziers such as Ay and Horemheb, while the king tended to the expansion of his religion and social systems. Evidence is that the new Aten religion was accepted by the aristocracy of the time, but that it was probably not widely practised by the common people.
Besides his chief wife, Nefertiti (the daughter of his vizier, Ay), Akhenaten had 4 other wives (2 were daughters of Nefertiti), at least 6 daughters and probably 1 son, Tuthankamen. Nefertiti died (or was disposed of) in his 12th regnal year, when he married her daughter, Merytaten. On his death (of unknown cause) in his 16th regnal year, he was probably buried in his prepared tomb at Akhetaten, but his mummy was subsequently removed and possibly re-interred in the Valley of the Kings in Thebes. The mysterious tomb 55 is often quoted as a possible final resting place, but his mummy has never been found. Subsequent pharaohs promptly restored the religion of Amun, and moved the capital back to Thebes.
Akhenaten's curious physiognomy
Judging from his statues and reliefs, Akhenaten had a eunuchoid body structure: narrow chest with gynaecomastia, wide hips with prominent fatty deposits, elongated spindly limbs and elongated neck and skull (Fig. 1).1,2 The physiognomy is typical of eunuchs castrated early in life, and is caused by a deficiency of androsterone (testosterone), normally produced predominantly in the testes. The small amount of testosterone produced in the adrenal glands is not sufficient to prevent the feminine growth pattern in adolescence. Normally, two gonadotrophic hormones (GTH) produced by the hypothalamus and anterior pituitary gland (luteinising hormone (LH) and follicle stimulating hormone (FSH)) stimulate the testes to produce testosterone and spermatozoa (sperm cells) respectively. For sperm cell production, an amount of testosterone is also essential, but androgen of adrenal origin will suffice for this.3,4
Differential diagnoses
A variety of diagnoses have been suggested to explain Akhenaten's physiognomy:
• There is no evidence that Akhenaten was a true eunuch as a result of early castration or destructive testicular disease in infancy. As a eunuch, he would have been infertile.
• Fröhlich's syndrome was one of the earliest suggestions.1,5 This is caused by a tumour or cyst of the hypothalamic-pituitary axis with hypogonadism owing to deficient production of GTH to stimulate the testes. Hypothalamic dysfunction also results in disordered hunger metabolism and resultant obesity. The feminine figure would fit Akhenaten's physical peculiarities although he was not fat. However, patients with Fröhlich's syndrome are infertile (Akhenaten had at least 6 children) and mental retardation is the rule.6 The pharaoh was not retarded.1 There is growing doubt whether this syndrome warrants an independent identity.
• Marfan's syndrome was suggested by Burridge7 as a possible diagnosis. Underlying this inherited disease is a disorder of the fibrillin gene which results in defective fibrin and collagen production. The patients characteristically have long, thin extremities, arachnoidactyli, dolicocephaly, with a narrow face and pectus excavatum (pigeon chest). Joints are remarkably lax ('double jointed'), and associated abnormalities such as subluxation of the ocular lens with retinal detachment, femoral hernias and cystic lung disease are common. They are also prone to dilatation of the proximal aorta with aortic regurgitation, dissecting aortic aneurysms, mitral incompetence and early heart failure. Although the elongated face and extremities would fit Akhenaten's physiognomy, Marfan's syndrome is not associated with the pharaoh's eunuchoid features.8
• Klinefelter's syndrome is mentioned by various authors.9 In this chromosomal abnormality (most typically with an XXY, 47 chromosome), whose incidence is approximately 1 in 500 newborns, the basic defect is hyalinisation of the testicular seminal tubules and defective Leydig cells, resulting in total azoospermia, testosterone deficiency and consequent eunuchoid features: tall, wide hips, female escutchion, gynaecomastia, and small testes.10 Mental retardation is common. Although Akhenaten's build would accordingly resemble Klinefelter's syndrome, the latter patients are infertile by definition, unlike the pharaoh.
• Kallmann's syndrome is a disorder inherited by autosomal recessive X-linked propagation, characterised by deficient synthesis of both hypothalamic-pituitary gonadotrophic hormones (FSH and LH) and is associated with anosmia/hyposmia owing to aphasia of the olfactory bulb. The incidence is approximately 1 in 50 000 births. The condition therefore presents with lifelong hypogonadism in the male and female. The male shows a pronounced feminine build and total infertility - the first characteristic fitting in with the 'Akhenaten syndrome', but not the infertility. Kallmann's syndrome may also include colour blindness and eventual optic atrophy, nerve deafness, cleft palate, renal abnormalities, crypto-orchidism and neurological abnormalities with mirror movement.11
• Fertile eunuch syndrome is characterised by selective deficiency of LH synthesis in the hypothalamic-pituitary axis, while FSH is normally produced. The result is effective sperm production (assisted by adrenal testosterone), but lack of testicular testosterone necessary to avoid feminine characteristics developing during adolescence. The patient therefore appears eunochoid but is indeed fertile - adrenal testosterone also facilitating sexual activity. This condition may occur in association with Kallmann's syndrome, or be caused by supracellar or intracellar tumours.12 Akhenaten showed no other evidence of a lifelong intracerebral tumour.
Discussion
We suggest that Akhenaten's curious body build - typical of eunuchoidism but associated with fertility - was due to the rare condition of 'fertile eunuch syndrome' - which might in future even be called Akhenaten syndrome. There can be little doubt that the pharaoh led an active sex life with at least 5 wives and, although some of his many children might perhaps have had extra-connubial parentage, it is most unlikely that all of them did. If Akhenaten's disorder was indeed partly Kallmann's syndrome (as we suggest), he almost certainly also lacked a sense of smell and, as he aged, possibly developed loss of hearing, blindness and odd neurological defects. He probably did not have a cleft palate.
Finding Akhenaten's mummy would be the 'cherry on top' in finally identifying the heretic pharaoh's metabolic defect, but it has so far eluded discovery.
1. Clayton PA. Chronicles of the Pharaohs. London: Thames & Hudson, 1994:120-128. [ Links ]
2. Gardner A. The Egyptians. London: Folio Society, 2000:81, 207-236. [ Links ]
3. Ganong WF. Review of Medical Physiology. Los Altos: Lange Med Publ, 1985:357-360. [ Links ]
4. Griffin JA, Wilson JD. Hermaphroditism. In: Walsh PC, Retik AB, Stamey TA, Vaughan ED, eds. Campbell's Urology. Philadelphia: W B Saunders, 1982:1516-1531. [ Links ]
5. Aldred C. Akhenaten, King of Egypt. London: Thames & Hudson, 1988. [ Links ]
6. Nelson DH, Thron GW. Fröhlich's Syndrome. In: Harrison TR, Adams RD, Bennett SL, eds. Harrison's Principles of Internal Medicine. New York: McGraw Hill, 1966:411. [ Links ]
7. Burridge A. Did Akhenaten suffer from Marfan's Syndrome? Temple Project Newsletter, Akhenaten no. 3, 1995. [ Links ]
8. Bearn AE. Marfan's Syndrome. In: Beeson PB, McDermott W, eds. Textbook of Medicine. Philadelphia: WB Saunders, 1975:1869-1870. [ Links ]
9. Nunn JF. Ancient Egyptian Medicine. Norman: University of Oklahoma Press, 1996:84. [ Links ]
10. Strachan MMJ, Walker BR. Endocrine Disease. In: Colledge NR, Walker BR, Ralston SH, eds. Davidson's Principles and Practice of Medicine. Edinburgh: Churchill Livingstone, 2010:763. [ Links ]
11. London DR. Kallmann's Syndrome. In: Weatherall DJ, Ledingham JGG, Warrell DA, eds. Oxford Textbook of Medicine. Oxford: Oxford Med Publ, 1987:10.87-88. [ Links ]
12. London DR. The fertile eunuch syndrome. In: Weatherall DJ, Ledingham JGG, Warrell DA, eds. Oxford Textbook of Medicine. Oxford: Oxford Medical Publications, 1987:10.101. [ Links ]
François Retief was Founding Dean of the Medical Faculty of the University of the Free State; Rector of Medunsa; Director-General of National Health Services; and Rector of the University of the Free State. He is now an Honorary Research Fellow, researching diseases of antiquity.
Louise Cilliers has taught at UNISA, the University of Natal and Rand Afrikaans University, and was Professor and Head of the Department of Classical Languages at the University of the Free State. She is also an Honorary Research Fellow at UOFS.
Corresponding author: L Cilliers (cilliers@ufs.ac.za)

