










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.8 Pretoria ago. 2011
ORIGINAL ARTICLES
Part IV. Human infections and antibiotic resistance
P Crowther-Gibson; N Govender; D A Lewis; C Bamford; A Brink; A von Gottberg; K Klugman; M du Plessis; A Fali; B Harris; K H Keddy; M Botha
Keywords: antibiotics; antibiotic (antimicrobial) resistance; pneumonia; acute respiratory infection; enteric infections; sexually transmitted infections; hospital-acquired infections
South Africa has a high burden of infectious diseases, including a large portion that are of bacterial origin. This section reviews the national burden of disease and levels of antibiotic resistance in common bacterial infections in the human population. The consequences of resistance on clinical outcomes, through either treatment failures or the development of more virulent infections, are largely unknown. The full impact of antibiotic resistance on health in South Africa therefore remains to be assessed.
National burden of disease
South Africa faces a quadruple burden of disease, as a result of the HIV/AIDS epidemic, other infectious diseases, injuries, and non-communicable diseases. Tables I and II show the top five causes of death for all ages and for children under the age of 5 (information from the Revised Burden of Disease Estimates for South Africa 20001 and the 2010 South African Health Review2).
The largest single cause of death for all ages is HIV/AIDS, accounting for 26% of deaths.1 This is 5 times greater than the next largest single cause of death, ischaemic heart disease and stroke (7% each) followed by tuberculosis (TB) and interpersonal violence, each accounting for about 6%. While males have higher proportions of deaths owing to homicide/violence and TB than females, females have higher proportions of deaths due to HIV/AIDS, heart disease and stroke.
There is considerable uncertainty around estimates of child mortality in South Africa because of incomplete vital registration.2 Existing numbers suggest that HIV/AIDS is the leading cause of death (46%), followed by neonatal causes dominated by preterm complications, asphyxia, and infection. Diarrhoea, pneumonia and injuries together account for 17% of mortality.
HIV/AIDS and TB
The most pressing health concern in South Africa is the HIV/AIDS epidemic, with around 29% of the population infected with the virus (2009). In addition to a high incidence of chronic illness and violencerelated deaths, South Africa has the largest number of people living with HIV/AIDS in the world (over 5.5 million), and 1 000 people are estimated to die as a result of AIDS daily.3 The Health Economics and HIV/AIDS Research Division predicts that HIV patients will soon account for around 60 - 70% of all hospital expenditures. HIV-related illnesses currently account for 50% of hospital admissions.
In absolute terms, South Africa has the fourth-largest TB population in the world (behind India, China and Indonesia) and bears 28% of the global burden of TB related to HIV. In 2007 data from the Global TB database, almost 1 000 per 100 000 of the population are infected with the disease annually. The emergence in South Africa of extremely drug-resistant tuberculosis (XDR-TB) that is considered virtually untreatable is of particular concern in a country with a high prevalence of HIV and a poor record of TB treatment.
Bacterial disease and antibiotic resistance
Our data are summarised from national surveillance efforts and site-specific case studies. The picture is incomplete because causes of illnesses and deaths are not well counted in South Africa, as is often the case in low-resource countries. Furthermore, separating bacterial from viral diseases requires a level of detail that, in most cases, does not exist. Nonetheless, the available information provides a basic idea of the current situation.
We present information on the burden of disease, current treatment options and antibiotic resistance for acute respiratory infections, diarrhoeal infections, sexually transmitted infections and nosocomial infections.
Acute respiratory and meningeal infections
As causes of severe respiratory tract, systemic and meningeal infections such as pneumonia, bacteraemia, and meningitis, the bacterial pathogens Streptococcus pneumoniae, Neisseria meningitidis and Haemophilus influenzae are major contributors to morbidity and mortality worldwide.
Antimicrobial chemotherapy has substantially decreased morbidity and mortality from these infectious diseases. However, their control is threatened by the global increase in antimicrobial resistance (AMR), including multidrug resistance. Resistant infections may adversely affect mortality, treatment costs, disease spread and duration of illness, increasing pressure on the choice of appropriate antibiotics. In developing countries such as South Africa and sub-Saharan Africa, where respiratory and meningeal diseases are more frequent because of the high burden of HIV infections, limited access to health care, costly antibiotics and low vaccination coverage, lack of access to antimicrobials and resistance to those available may increase the morbidity and mortality of vaccine-preventable diseases.
Streptococcus pneumoniae
S. pneumoniae is a leading cause of bacterial infection worldwide.4 The World Health Organization (WHO) estimates that 1.6 million people, including up to 1 million children aged <5 years, die annually of pneumococcal infection, with most deaths in developing countries.5
Treatment
Successful management of pneumococcal disease involves use of early antimicrobial therapy.6 During the 1940s, clinical pneumococcal isolates exhibited complete susceptibility to antibiotics such as penicillin, the antibiotic of choice for the treatment of pneumococcal infections.7 However, in Australia, intermediate penicillin resistance was observed for the first time in 1967.8 In South Africa, fully penicillin-resistant S. pneumoniae strains were detected in 1977,9 and in 1978 the occurrence of multidrug-resistant and highly resistant strains was reported.10,11 Since then, the prevalence of S. pneumoniae antibiotic resistance has increased around the world, not only to penicillin but also to non-β-lactam drugs, such as the macrolides, tetracycline, chloramphenicol, the fluoroquinolones and co-trimoxazole. Resistance to non-β-lactam drugs is often associated with decreased susceptibility to penicillin, so the prevalence of multidrug-resistant strains is also increasing.12
Antibiotic resistance
The increasing prevalence of pneumococcal resistance to single and multiple antimicrobials in South Africa demonstrates the need for new strategies to combat the problem, especially in terms of preventing increased mortality and treatment failures in penicillin-resistant pneumococcal meningitis.13,14 The clinical impact of antibiotic resistance has been reported as treatment failures for acute otitis media,15 and for pneumococcal meningitis.13,16 However, using the revised penicillin susceptibility breakpoints of 4 µg/ml for intermediate and >8 µg/ml for resistant strains, there is no evidence for a relationship between penicillin resistance and pneumococcal pneumonia treatment failures.17,18
Surveillance data reveal that rates of resistance to penicillin and other antibiotics among S. pneumoniae vary by geographical location. Penicillin-resistant pneumococci have been reported with particularly high frequencies in South Africa since the mid-1970s19 and in other African countries since the 1980s.
A 1997 African multicountry study revealed that penicillin resistance levels among all isolates of S. pneumoniae ranged from 9% to 61%, and that an increase in resistance has been observed in four countries across Africa.20 Resistance levels in North Africa are generally high, as reported by Algeria (35% of all isolates),21 Egypt (49% of invasive isolates),22 and Tunisia (41% of all isolates),20 although in Morocco levels are much lower (9% of all isolates).20 Penicillin resistance in West Africa varies from 62% in Senegal,20 31% in Ghana23 and 22% in Ivory Coast20 down to 7% of invasive isolates in The Gambia.24 In East Africa, the prevalence in Ethiopia and Kenya has increased over the years to 29% of clinically significant isolates, and 48% of paediatric invasive isolates, respectively.25-27 In Malawi, a 1997 study of paediatric nasopharyngeal isolates revealed penicillin resistance of 21%.28 In Zambia, 14% of paediatric non-invasive isolates were penicillin-resistant in 199429 and in Mozambique, a prevalence of 14% of paediatric invasive isolates was reported.30 No systemic studies have defined the reasons for the diversity in resistance rates reported.
South Africa has been the primary site of pneumococcal penicillin resistance surveillance and research in Africa, and has had one of the highest reported rates in the world.31 Since the first reports of resistance in the 1970s, the prevalence of resistance in S. pneumoniae in South Africa has increased. Between 1979 and 1986, the prevalence of resistance to one or more antibiotics in pneumococcal cerebrospinal fluid and blood isolates increased from 4% to 14%.32,33 A continuation of the same survey, between 1991 and 1998, reported that antibiotic resistance increased from 19% to 25% among all age groups, and in children from 32% to 38%.34 Among all age groups during this period, penicillin resistance increased from 10% to 18%.34 In 1992, 40% of isolates causing community-acquired meningitis or bacteraemia in children were penicillin-resistant.31 A 1999 Alexander Project study of pneumococcal isolates from the private sector in Johannesburg revealed that 79% were penicillin-resistant.31 Also in 1999, a study of nasopharyngeal isolates from private paediatric practices in Johannesburg found that antibiotic resistance was 69%, with 37% being multiply resistant.35 In 2003, a report on isolates from private clinical laboratories in South Africa showed that the rate of penicillin resistance among all age groups was 76%.36 Other studies in that year on invasive pneumococcal isolates from adults outside the private sector who were likely to have been exposed to less antibiotic prescribing revealed penicillin resistance levels of 13%,37 and a study on non-invasive isolates from HIV-infected adults reported penicillin resistance at 15%.38 A study conducted in Gauteng in 2006 on adults with bacteraemic pneumonia showed that 33% of isolates were penicillin-resistant, when using the historical meningitis susceptibility breakpoints.39 Penicillin resistance in South Africa remains mainly intermediate in level, with a low prevalence of fully resistant isolates. Although, annually, resistance levels have increased overall, these are dependent on the site of specimen collection, age of the patients, and their location in the country.
Macrolide resistance. The increasing incidence of penicillin-resistant S. pneumoniae has been paralleled by an increase in resistance to other classes of antimicrobials, suggesting that penicillin resistance serves as a marker of resistance to other drugs.40-43 Almost 25% of S. pneumoniae isolates from South Africa show full erythromycin resistance, with over 90% of these also resistant to clindamycin.31 Additionally, 40 - 50% of penicillin-resistant isolates show cross-resistance to macrolides.31 In 2001, a national multicentre study of private clinical laboratories in South Africa revealed that a high prevalence (61%) of non-invasive isolates were macrolide (clarithromycin and azithromycin) resistant,36 whereas a national 2005 study showed that 14% of invasive pneumococcal isolates were resistant to macrolides.44
Co-trimoxazole resistance. The Alexander Project in Johannesburg in 1996 - 1997 revealed that 15 - 20% of isolates were resistant to co-trimoxazole,31 while a 2001 study showed that co-trimoxazole resistance was as high as 72%.36 Other South African studies have found that co-trimoxazole resistance is associated with multidrug resistance in pneumococcal isolates from childhood carriers in hospitals11 and healthy children in the community.45 In a 1986 study, 43% of penicillin-resistant strains among childhood carriers in South Africa were also resistant to co-trimoxazole.46
Fluoroquinolone resistance. A Canadian study showed that 1% of pneumococci have reduced susceptibility to fluoroquinolones.47 An increase in the frequency and degree of resistance to fluoroquinolones among pneumococci occurred particularly in penicillin-resistant S. pneumoniae, and in adults over 65 years.47 In South Africa, 2008 study data suggest that the use of fluoroquinolones to treat multidrug-resistant TB in children has led to the emergence of invasive pneumococcal disease (IPD) caused by levofloxacin-non-susceptible S. pneumoniae,48 although these strains remain rare outside those institutions.
Multidrug resistance. S. pneumoniae resistance to three or more different classes of antibiotics, defined as multidrug resistance, is a problem of increasing concern worldwide.49 The emergence of multidrug resistance was first reported in Soweto, South Africa, in 1977.11 Subsequently, multidrug resistance emerged globally.20,41,50,51 In South Africa in 2004, a third of pneumococcal isolates studied displayed multidrug resistance.49 Successful multidrug-resistant clones that are disseminated worldwide belong to only 10% of the 93 pneumococcal serotypes, including serotypes 3, 6A, 6B, 9N, 9V, 14, 19A, 19F and 23F.52
Neisseria meningitidis
N. meningitidis causing meningitis and other meningococcal diseases, such as meningococcaemia, is a major cause of morbidity and mortality in children worldwide, and of epidemics in Africa and Asia.
Antibiotic resistance
In Africa, limited data are available regarding antimicrobial non-susceptibility of N. meningitidis. Few studies have documented the existence of penicillin and other antimicrobial non-susceptibility in Africa other than South Africa. A study in Morocco reported an average rate of 4% for penicillin intermediately resistant invasive meningococcal isolates collected from 1992 to 2000.53 All isolates tested were susceptible to cefotaxime, chloramphenicol and rifampicin. Laboratory-based surveillance in Egypt from 1998 to 2004 reported high rates (86%) of resistance to co-trimoxazole but low rates of resistance to penicillin (1%) and ampicillin (5%); 40% of isolates were intermediately resistant to either ampicillin (minimum inhibitory concentration (MIC) 0.25 - 1 µg/ml) or penicillin (MIC 0.12 - 0.25 µg/ml) and 34% were intermediately resistant to both penicillin and co-trimoxazole.54 One isolate, with intermediate resistance to penicillin, tested positive for β-lactamase production.
A serogroup A meningitis outbreak in northern Ghana in 1998 showed no evidence of resistance to any of the drugs tested, with the exception of sulphadiazine.55 No resistance to β-lactam agents or chloramphenicol was reported during surveillance of meningococcal meningitis in Cameroon during the 2007 and 2008 meningitis seasons. In Ethiopia, epidemic meningococcal isolates collected during 2002 -2003 were compared with those from the 1988 -1999 epidemic.56 All 40 isolates were fully susceptible to the antibiotics tested, except for sulfamethoxazole (MIC >256 µg/ml). A study of the aetiology of bacterial meningitis in Nigeria was conducted between 1987 and 1992, and N. meningitidis was the most common pathogen isolated.57 Antimicrobial susceptibility testing by disc diffusion of 118 meningococci demonstrated 39% and 67% non-susceptibility to penicillin and co-trimoxazole, respectively; 5 were resistant to both penicillin and chloramphenicol but were susceptible to ciprofloxacin. Non-susceptibility to penicillin increased progressively over the period analysed, seemingly caused by the abuse of penicillin, which is readily purchased over the counter.
In South Africa, β-lactamase-producing penicillin-resistant (MIC >256 µg/ml) meningococcal isolates from two patients were reported in 1987, but the mechanism of resistance was not confirmed genotypically and the strains were lost.58 National laboratory-based surveillance for invasive meningococcal disease in South Africa was initiated during 1999. A study that genotypically characterised invasive meningococci collected from 2001 to 2005 reported a relatively low prevalence of penicillin non-susceptibility.59 During this period 6% of isolates were intermediately resistant to penicillin, with MICs ranging from 0.094 µg/ml to 0.25 µg/ml. No isolates tested were fully resistant or tested positive for β-lactamase production and all were susceptible to other drugs tested, with the exception of rifampin (0.3%). In 2009, South Africa reported its first case of fluoroquinolone-resistant N. meningitidis.60 MICs for ciprofloxacin and levofloxacin were 0.125 µg/ml, and 0.25 µg/ml for ofloxacin. Resistance appeared to be mediated by a single amino acid substitution in the DNA gyrase enzyme. The isolate was susceptible to other drugs tested but was resistant to nalidixic acid (12 µg/ml). No subsequent cases of fluoroquinolone-resistant meningococci have been reported.
Haemophilus influenzae
H. influenzae is an important cause of acute otitis media, sinusitis, chronic bronchitis, community-acquired pneumonia and meningitis.61 Before the introduction of H. influenzae type b (Hib) conjugate vaccines, globally Hib was estimated to be responsible for approximately 3 million serious illnesses and 386 000 deaths annually;62 95% of these cases and 98% of all deaths occurred in patients from developing countries, mainly in children <5 years.63 In sub-Saharan African children, Hib is responsible for 20% of all radiologically confirmed pneumonia cases and 40% of all meningitis cases.64,65
Treatment
Antimicrobial treatment is pivotal in the management of H. influenzae disease. Until the early 1970s, when H. influenzae resistance to ampicillin was first reported,66 ampicillin was the cornerstone of therapy.67,68 In sub-Saharan Africa, chloramphenicol and penicillin are the first-line antibiotics to treat meningitis and severe pneumonia, while mild pneumonia is treated with co-trimoxazole, ampicillin or amoxicillin.69,70 In South Africa, β-lactams such as penicillin, ampicillin or amoxicillin are still recommended as empirical first-line therapy for the treatment of respiratory tract infections in patients <65 years old and without co-morbid illness.71,72 Alternative agents recommended for treating patients >65 years old, or who have co-morbid illness, include amoxycillin-clavulanate or selected oral cephalosporins (cefuroxime axetil or cefpodoxime).71,72
Antibiotic resistance
The increasing prevalence of resistance among H. influenzae isolates to commonly used antibiotics is of concern. Resistance to penicillin is high, with prevalence rates of >45% reported in some settings.69,70,73,74 Resistance to ampicillin and other β-lactams is almost exclusively due to β-lactamase production. Isolates expressing this mechanism remain susceptible to β-lactamase-inhibitor combinations such as amoxicillin-clavulanic acid. A second non-β-lactamase-mediated resistance mechanism is conferred by mutations in the ftsI gene, encoding the transpeptidase region of penicillin-binding protein 3 (PBP3), which results in decreased affinities of the PBP3 for β-lactams.75 Such strains are termed β-lactamase-negative ampicillin-resistant (BLNAR). Worldwide, BLNAR strains continue to be isolated at very low frequencies.75-78 However, their prevalence has recently increased in countries such as Japan,79,80 Spain76,79 and Korea.81
In Africa, data for H. influenzae AMR, especially regarding trends, are sparse.69,70,82,83 Increasing rates of chloramphenicol and co-trimoxazole resistance have been reported in Africa.70,82,84 In Cameroon, chloramphenicol resistance levels of up to 84% have been reported,84 while high prevalence of co-trimoxazole resistance have been reported in Mozambique (46%)82 and Kenya (66%).70
Beta-lactamase production is by far the most common mechanism of ampicillin resistance in South African isolates of H. influenzae.75 From 2003 to 2008, 2 177 cases of invasive H. influenzae were reported to the national laboratory-based surveillance system, of which 54% had viable isolates available for antimicrobial susceptibility testing. Of the viable isolates, 2% and 15% were found to be intermediately resistant and resistant to ampicillin, respectively. Of the 190 ampicillin non-susceptible isolates, 99% were β-lactamase producing and 1% were phenotypically β-lactamase-negative ampicillin resistant (BLNAR) and were characterised as low-level BLNAR (MIC 2 µg/ml). In addition, a β-lactamase-positive amoxicillin-clavulanate-resistant (BLPACR) strain was identified (MIC 8 µg/ml).
In the only previous report of South African BLNAR strains (ampicillin MIC 2 µg/ml),85 a BLNAR prevalence of 6% among isolates collected from various sources, including respiratory secretions and blood, was reported during a SENTRY worldwide surveillance programme in the Asia-Pacific region.
Diarrhoeal infections
Non-typhoidal Salmonella
Salmonellosis due to non-typhoidal Salmonella enterica spp. accounts for a large burden of disease worldwide. Illness is usually self-limiting and antimicrobial therapy is not required, but in cases of invasive disease antimicrobial therapy is important for a successful clinical outcome. Over the period 2003 - 2010, the Enteric Diseases Research Unit (EDRU) at the National Institute for Communicable Diseases (NICD) has documented 16 435 records of laboratory-confirmed cases of non-typhoidal Salmonella enterica isolates from human and non-human sources for South Africa. Isolates received from non-human sources (N=224) include samples of water, food and animal specimens processed at the EDRU for study purposes, or as a service by special request and not as part of their routine surveillance activities. These isolates were therefore not screened for antimicrobial susceptibility. Of the 16 211 human isolates, 13 702 were viable and were screened using antimicrobial agents.
Treatment
The treatment of choice for such infections are third-generation cephalosporins and fluoroquinolones, as resistance to ampicillin, chloramphenicol and co-trimoxazole has been present worldwide for many years.86 Failure to respond to treatment with the fluoroquinolones, as isolates have displayed decreased susceptibility to ciprofloxacin, has recently been reported. AMR to nalidixic acid has been used as a proxy to identify isolates that may not respond to treatment with ciprofloxacin.
Antibiotic resistance
Resistance to quinolones usually occurs as a result of alterations in the target enzymes (DNA gyrase and topoisomerase IV) and as a result of changes in drug entry and drug efflux.87 Resistance to quinolones can also be mediated by plasmids that carry genes coding for Qnr proteins, which protect the quinolone targets from inhibition. Plasmid-mediated quinolone resistance among South African strains of non-typhoidal Salmonella has been previously reported, as well as the detection of mutations in the DNA gyrase enzyme of clinical non-typhoidal Salmonella.88
In the period 2003 - 2010 there has been a decrease in the proportion of non-typhoidal Salmonella isolates showing resistance to ampicillin from 64% to 16%, chloramphenicol from 47% to 14%, ceftriaxone from 40% to 10%, and nalidixic acid from 38% in 2003 to 10% in 2010. Although the overall proportion of non-typhoidal Salmonella isolates showing resistance to nalidixic acid has decreased over time, when comparing non-typhoidal Salmonella isolates causing invasive disease with non-typhoidal Salmonella isolates causing non-invasive disease, isolates causing invasive disease account for the greater proportion of isolates showing resistance to nalidixic acid. There has been no increase in the proportion of non-typhoidal Salmonella isolates exhibiting resistance to ciprofloxacin. In 2004, the greatest proportion of non-typhoidal Salmonella isolates, just less than 2% (26/1 597), showed resistance to ciprofloxacin. Overall, just less than 1% of all non-typhoidal Salmonella isolates exhibited resistance to ciprofloxacin from 2003 to 2010. Over this same period the proportion of non-typhoidal Salmonella isolates exhibiting resistance to sulfamethoxazole has fluctuated from 40% of isolates in 2003, to a high of 78% of isolates for 2004 and 2005, to 48% of isolates in 2010, but overall there has been a general decrease in resistance to sulfamethoxazole since the highs of 2004/2005.
Extended-spectrum β-lactamase (ESBL)-producing non-typhoidal Salmonella isolates have been identified by the EDRU since 2003. In 2003, 28% (452/1 597) of all non-typhoidal Salmonella isolates were found to be ESBL producing. The proportion of all non-typhoidal Salmonella isolates found to be ESBL producing has decreased to 8% in 2010. ESBL production in non-typhoidal Salmonella in South Africa is usually associated with nosocomial isolates of non-typhoidal Salmonella.89,90 Govinden et al.91 have suggested that among a selection of clinically isolated strains of non-typhoidal Salmonella there is co-expression of quinolone and ESBL.
Salmonella enterica serotype Typhi
S. Typhi bacterium causes typhoid fever and is transmitted via food or water contaminated with human faeces. It is of clinical importance, as humans are the only recognised reservoir of S. Typhi. Typhoid fever is a major contributor of illness and death in humans, particularly in developing countries. In 2000 it was estimated that typhoid fever caused approximately 22 million illnesses and 220 000 deaths globally.92
Treatment
Antibiotics are vital in the management of typhoid fever. Various fluoroquinolones such as ciprofloxacin have become the treatment of choice for infection with S. Typhi.93 However, as with the non-typhoidal Salmonella, increased resistance to the quinolone nalidixic acid and reduced susceptibility to the fluoroquinolone ciprofloxacin have been reported.86
Antibiotic resistance
South Africa, with an estimated typhoid fever burden of disease of 100/100 000 of the population, has not been spared nalidixic-acid-resistant S. Typhi.92 Smith et al.87 reported on 27 nalidixic-acid-resistant isolates collected between 2003 and 2007 that exhibited mutations in both gyrase and topisomerase genes and an active efflux of antibiotic as mechanisms of quinolone resistance. Keddy et al.94 subsequently reported on the first locally isolated strain of fluoroquinolone-resistant S. Typhi. The associated mechanism of resistance was the presence of a single amino-acid mutation in the gyrase A gene along with a QnrS protein and active efflux of antibiotic. They concluded that the strain was possibly imported through contact with a traveller from the Asian sub-continent.94
In the period 2003 - 2010, the EDRU received 706 viable S. Typhi isolates that have been screened using antimicrobial agents. Of these 706 viable S. Typhi isolates 595 caused invasive disease. The proportion of S. Typhi isolates resistant to the older antibiotic ampicillin has fluctuated over this period from 10% in 2003 to a high of 40% in 2006, and 10% at the end of 2010. The proportion of S. Typhi isolates resistant to sulfamethoxazole remained consistently around 30%. In terms of chloramphenicol, the proportion of S. Typhi isolates identified by the EDRU as resistant has more than doubled from 5% in 2003 to 13% in 2010. The proportion of S. Typhi isolates causing invasive disease resistant to chloramphenicol for the year 2010 was 15%. In 2009, 20% (N=60) of all S. Typhi were resistant to the quinolone nalidixic acid. This proportion of quinolone-resistant S. Typhi isolates has been the highest identified through laboratory surveillance by the EDRU since 2003. In 2003, the proportion of quinolone-resistant S. Typhi was 10%, which decreased to 5% in 2006 and increased to 15% at the end of 2010. Over this same 8-year period, the proportion of ciprofloxacin-resistant S. Typhi was zero, except in 2009 when that proportion rose to 2% with the isolation of the fluoroquinolone-resistant S. Typhi mentioned earlier. Although there have been reports of ESBL-producing S. Typhi, none has been isolated in South Africa to date.95
Shigella
Shigellosis is caused by the enteric bacteria Shigella species. The disease is a worldwide problem, particularly in areas with poor access to clean water and sanitation, causing an estimated 600 000 deaths annually. As a result Shigella is a pathogen associated with water or food contamination as it can easily be spread by the faecal-oral route. The only reservoirs of significance, except for primate colonies, are humans. Shigella dysenteriae type 1 is probably the most important Shigella variant because it is epidemic-prone and the production of Shiga toxin by this variant of Shigella results in severe illness.96 S. sonnei has been associated with food- and water-borne outbreaks.
Treatment
Shigella isolates that are multidrug-resistant to ampicillin, trimethoprim, sulfamethoxazole and tetracycline have become prevalent. As a result, reliance on antibiotic treatment has shifted toward fluoroquinolones such as ciprofloxacin as first-line treatment. Although optimal treatment is to replace fluid and electrolytes, the use of antibiotics to shorten the duration and severity of disease and to decrease the period of pathogen excretion is important.97
Antibiotic resistance
From 2003 to 2010, the EDRU received 9 538 viable Shigella isolates. Of the 9 538 Shigella isolates only 337 caused invasive disease. Antimicrobial screening shows that the proportion of Shigella isolates resistant to older antibiotics over the 8-year period has been consistent: 50% for ampicillin, 50% for tetracycline, 80% for sulfamethoxazole and 40% for chloramphenicol. In terms of what has now become first-line treatment, consistently from 2003 to 2010 the proportion of Shigella isolates resistant to nalidixic acid has been 1% and for both ciprofloxacin and ceftriaxone the proportion of resistant Shigella isolates has been just below 1%. The proportion of Shigella isolates exhibiting ESBL production has also consistently been less than 1%. Despite the consistent low levels of resistance to both quinolones and fluoroquinolones, there is concern that the numbers may increase over time.
Vibrio species
Vibrio spp. are commonly found in aquatic environments and infection occurs as a result of poor access to clean water and sanitation. Of more than 30 species of Vibrio, 12 have been associated with illness in humans,98 of which the most important are V. cholerae subgroups O1 and O139, the causative agent of epidemic cholera.99 Although infection occurs with non-O1 V. cholerae the clinical manifestation is milder because this subgroup of V. cholerae lacks the cholera-toxin-producing gene. Pandemics of the devastating diarrhoeal disease caused by V. cholerae have been documented since 1817.98 Most epidemics occur in developing countries where it is endemic. The debilitating disease caused by V. cholerae is the result of an enterotoxin known as choleragen. V. cholerae O1 occurs in 3 serotypes (Ogawa, Inaba and Hikojima), and is further characterised into two biotypes - El Tor and classic.98,99
Treatment
Although antimicrobials are prescribed for the management of severe cases, to shorten the duration of illness and reduce the volume of rehydration solution required, V. cholerae strains are resistant to a number of antimicrobials including tetracycline, co-trimoxazole, trimethoprim and sulfamethoxazole. Knowledge of the AMR profile of local strains is important for the management of complicated cases, but adequate and timely rehydration therapy remains the gold-standard treatment for cholera.99
Antibiotic resistance
In 2008, an outbreak of cholera started in South Africa and continued into 2009. This was linked to cholera in Zimbabwe, with patients crossing the border to seek health care in South Africa. During 2009, the EDRU processed 570 V. cholerae O1 isolates associated with the outbreak. Further laboratory characterisation showed that 98% of the isolates were serotype Ogawa and 2% were serotype Inaba; all were biotype El Tor and 99.5% of the isolates were positive for the cholera toxin. The 2008/2009 outbreak isolates showed 100% resistance to co-trimoxazole, 48% resistance to chloramphenicol, 100% resistance to nalidixic acid, 3% resistance to tetracycline and 39% resistance to erythromycin. Although there was 100% resistance to nalidixic acid, none of the isolates associated with this outbreak was resistant to ciprofloxacin.100
In a second outbreak in 2008, reported from Shebagold Mine in the Ehlanzeni district of Mpumalanga, 31 isolates were submitted for analysis to the EDRU. All were biotype El Tor and displayed resistance to ampicillin, amoxycillin-clavulanate, sulfamethoxazole, trimethoprim, chloramphenicol, nalidixic acid, kanamycin, streptomycin and tetracycline, which was initially the antimicrobial agent of choice in the treatment of cholera in Africa. Although the isolates exhibited resistance to nalidixic acid they were susceptible to ciprofloxacin and imipenem. Further resistance to third-generation cephalosporins ceftriaxone and ceftazidime was observed, indicative of ESBL activity.101
The EDRU routinely conducts antimicrobial screening on all V. cholerae O1 isolates and has data available from 2007. Since 2007, the EDRU has received 899 viable V. cholerae O1 isolates. In 2007, 13 of the 30 isolates received were resistant to sulfamethoxazole. The summary of these recent outbreaks is the most accurate description of the current situation of AMR among V. cholerae isolates in South Africa.
Diarrhoeagenic Escherichia coli
E. coli is commonly found in the normal flora of the colon and is used as an indicator of faecal contamination of water. Although a commensal organism, E. coli is an important human pathogen that has been associated with several gastro-intestinal syndromes. There are 6 major categories of diarrhoeagenic E. coli; enterotoxigenic (ETEC), entero-invasive (EIEC), enteropathogenic (EPEC), enterohaemorrhagic (EHEC), diffusely adherent (DAEC) and entero-aggregative (EAggEC). The most clinically important is EHEC. The strain E. coli O157:H7 has been associated with outbreaks and clinical presentation of haemorrhagic diarrhoea, colitis and haemolytic uraemic syndrome.102, 103 E. coli O157:H7 produces two cytotoxins, one a verotoxin and the other a toxin identical to the Shiga toxin produced by Shigella dysenteriae type 1. These Shiga-toxin-producing E. coli are referred to as STEC. STECs are not limited to the E. coli O157:H7 serotype, as any of the non-O157:H7 serotypes may present as EHEC or STEC.
Treatment
Fluid replacement is recommended as treatment for gastro-enteritis caused by E. coli O157:H7 or non-O157:H7 STEC infection, as it believed (although evidence is lacking) that antimicrobial therapy is of no benefit and may increase the risk of haemolytic uraemic syndrome.103
Antibiotic resistance
As part of the EDRU's surveillance activities, a screening multiplex polymerase chain reaction (M-PCR) analysis is conducted on all E. coli isolates submitted to the unit to categorise the isolate into one of the aforementioned diarrhoeagenic E. coli categories. This is done because antimicrobial screening is conducted only on isolates that are EHEC or STEC. Over the years 2003 - 2010, the EDRU received 3 109 viable E. coli isolates, of which 17 were found to be STEC and 21 to be EHEC by M-PCR. Antimicrobial screening of these isolates shows that consistently less than 1% of all STEC or EHEC isolates are resistant to tetracycline, ampicillin, amoxycillin-clavulanate, co-trimoxazole, trimethoprim, sulfamethoxazole and chloramphenicol. The proportion of E. coli isolates showing ESBL activity for the same period was also consistently lower than 1%.
A recent study of clinical isolates of ESBL-producing E. coli isolates screened for ESBL enzymes found that 16 of the 22 isolates were resistant to ciprofloxacin as a result of the presence of aac (6_)-Ibcr, a variant of an aminoglycoside modifying enzyme.104 Nothing from the EDRU surveillance data suggests that there may be E. coli resistant to the fluoroquinolones, as none was found to be resistant to ciprofloxacin, but these findings should be taken into consideration.
Sexually transmitted infections
Bacterial sexually transmitted infections (STIs) cause significant morbidity in South Africa and may rarely cause death, for example from ruptured ectopic pregnancy secondary to tubal damage from Neisseria gonorrhoeae and Chlamydia trachomatis or fetal death from congenital syphilis. They account for 87% of male urethritis syndrome (MUS) cases, 30% of vaginal discharge syndrome (VDS) cases and 10% of genital ulcer syndrome (GUS) cases. Importantly, both ulcerative and genital discharge syndromes are key co-factors for augmenting HIV infectiousness and susceptibility and increase transmission risk by 2 - 5 times in prospective studies.105
Patients with bacterial STIs may present with MUS, VDS, scrotal swelling syndrome (SSW, i.e. epididymo-orchitis), lower abdominal pain syndrome (LAP, i.e. pelvic inflammatory disease), GUS or buboes. As the syndromic management approach does not utilise laboratory testing, it is not possible to determine the national burden of bacterial STIs by individual STI pathogen. The bacterial burden also differs according to STI syndrome; recent aetiological surveillance data from South Africa showed that bacteria account for 87% of cases of MUS, 30% of cases of VDS and only 10% of GUS cases (Table III).
Between April 2004 and March 2005, 1 654 776 new STI episodes were treated in primary health care (PHC) clinics throughout South Africa. Incidence rates of new STI syndrome episodes, calculated per 1 000 population aged 15 - 49 years, demonstrated a national incidence rate of 63 per 1 000 population. The highest incidence rates were recorded in Limpopo (90 per 1 000), KwaZulu-Natal (87 per 1 000) and the Eastern Cape (73 per 1 000); the lowest incidence rate was recorded in the Western Cape (38 per 1 000). During the same time period, a total of 145 818 new STI syndrome episodes (46 222 in males, 99 596 in females, 8.8% of the national total) were reported among 126 656 patients in the sentinel survey, with a peak in the 20 - 24-year-old age group. In men with STIs, the most frequent syndromes were MUS and GUS, whereas for women they were VDS and LAP (Fig. 1). The relative prevalence and incidence of MUS, the most reliable indicator syndrome for 'true' STIs, seen at the sentinel sites during 2004 - 2005, is shown by province in Table IV.

Neisseria gonorrhoeae
At present in South Africa, AMR is solely an issue for N. gonorrhoeae infection. It is very important to have effective microbiological surveillance systems in place in South Africa and its neighbouring countries to facilitate early detection of such strains. There is mounting public health concern that gonorrhoea may become untreatable in years to come, which would have an extremely deleterious effect on HIV transmission in South Africa, where the prevalence of both diseases is high. Accordingly, efforts must be made locally to reduce the burden of gonorrhoea and for the international community to invest in the search for a new class of antimicrobial agents active against N. gonorrhoeae.
Treatment
In South Africa, STIs have been treated using the syndromic management approach since the late 1990s. This approach is to manage symptomatic STIs and has the advantage of providing same-day treatment according to treatment flow charts, which can easily be adhered to by nursing staff at every PHC entry point across the country. Laboratory testing of STI patients is not required for case management, although the WHO recommended that periodic aetiological and AMR surveys are carried out in all countries using the approach. Lack of clinical samples has deskilled laboratory staff in terms of ability to culture and test gonococci for antimicrobial susceptibility. The syndromic approach generally works better for male-associated compared with female-associated STI syndromes. The poor specificity of syndromes such as VDS and LAP to predict the presence of STIs leads to overdiagnosis of STIs, unnecessary stigmatisation and potential relationship difficulties. Importantly, it results in substantial overprescribing of antimicrobial agents that may influence the development of AMR among sexually transmitted and non-sexually transmitted bacteria.106 Mathematical modelling has shown that syndromic management is the cheapest programmatic approach to the management of STIs, although there remains debate as to whether it is the most cost-effective.107,108
Owing to the rapid emergence of quinolone-resistant gonococci in 2003, and their subsequent spread throughout the country, revised national guidelines were published in 2008. Gonorrhoea should now be treated with oral cefixime or intramuscular ceftriaxone. Gonococci exhibiting clinical resistance to oral cephalosporins have emerged in the Western Pacific region and have now spread to Europe. No such isolates have been found in Africa to date, but their emergence is likely in the near future. Other key changes include use of acyclovir in the GUS treatment algorithm and the replacement of erythromycin with amoxicillin for the treatment of presumptive chlamydial infection in pregnant women with VDS.
At least half of STI care episodes are estimated to be managed by the private sector, where the National Department of Health (NDoH) has less influence on prescribing practice.109 An interview-based study conducted among general practitioners (GPs) in Gauteng over a decade ago highlighted poor knowledge of STI syndromic management, and less than half of prescriptions overall were judged to be effective.110 In addition, for most STI syndromes, uninsured patients were offered significantly cheaper and less convenient antibiotic regimens. Prescribing correct drug treatment for STIs by GPs has been associated with male gender and recent graduation of the GP, as well as the patient having medical aid.111 A study of knowledge, beliefs and attitudes of GPs and public-sector nurses in Gauteng, conducted several months after the publication of the revised 2008 national STI guidelines, found that only a quarter of the GPs, as opposed to two-thirds of nurses, were aware that cefixime should now be used to treat gonorrhoea (D A Lewis, unpublished data). Within South Africa, there appears to be a lack of an effective pathway to disseminate revised NDoH guidelines to GPs, and this remains a key challenge for quality private-sector health care delivery. To make matters worse, at the time that the national STI guidelines were changed, the NDoH had to purchase cefixime directly from Merck in Germany, and it was only made available at PHCs. This led to an inequality in the health care system, where cefixime was available to patients with presumptive gonorrhoea attending public clinics whereas similar patients attending tertiary-level hospital or GP facilities could only be treated with ceftriaxone. Cefixime was finally made accessible to all practitioners for the treatment of gonorrhoea at the start of 2011.
Antibiotic resistance
The need for periodic aetiological and AMR surveillance, which is an integral part of syndromic management, has been largely ignored by most African countries. With the exception of South Africa, where good laboratory infrastructure and funding exist to support surveillance, Africa has minimal AMR data available for bacterial STI pathogens. Gonorrhoea is the only bacterial STI for which AMR surveys are currently undertaken in South Africa. Despite reports concerning AMR in chlamydial strains collected from patients failing treatment, it remains controversial whether documented stable homotypic drug resistance to antibiotics exists and AMR studies are not routinely performed for this STI pathogen anywhere in the world.112,113 Although a high prevalence of tetracycline resistance has been documented among Mycoplasma genitalium isolates, susceptibility testing for this relatively new bacterial STI pathogen is performed in few specialist laboratories worldwide.114,115 Screening for resistance in Treponema pallidum remains a challenge because of inability to culture this organism in vitro. Although resistance of T. pallidum to penicillin has not been described to date, a molecular assay for the macrolide resistance-associated A2058G mutation in 23S rRNA does exist.116 The STI Reference Centre has failed to detect this A2058G mutation in T. pallidum-positive DNA extracts from genital ulcer swabs recently collected in South Africa (D A Lewis and E E Müller, unpublished data). Chancroid is now a rare cause of GUS, and it is no longer feasible to culture isolates to determine AMR. Chancroid was the most frequent cause of GUS in the 1990s and surveys performed at that time reported that most strains were resistant to penicillin, co-trimoxazole and tetracyclines but susceptible to amoxicillin-clavulanate, macrolides, quinolones and extended-spectrum cephalosporins.117
Gonococci isolated in South Africa remained fully susceptible to ciprofloxacin, the former first-line therapy used to treat gonorrhoea, until 2003 when researchers from the University of KwaZulu-Natal reported the abrupt emergence of quinolone-resistant N. gonorrhoeae (QRNG) among MUS patients attending an STI clinic in Durban.118 Subsequently, the NDoH requested that the STI Reference Centre co-ordinate a gonococcal resistance survey in several South African cities, which included Cape Town, Durban, Johannesburg, Pietermaritzburg, Pretoria and Mthatha. The data revealed varying prevalence of QRNG, from 0% in Pretoria to 24% in Durban, although all isolates tested appeared susceptible to cephalosporins.119 Despite the widespread problem with QRNG, revised national guidelines were not published until 2008, at which point ciprofloxacin was replaced by either cefixime or ceftriaxone as first-line therapy for presumptive gonococcal infection.120 During this 4-year period, further rises in QRNG prevalence was reported from Durban (24% in 2004; 42% in 2005), Pretoria (0% in 2004, 7% in 2005), Cape Town (7% in 2004; 27% in 2007) and Johannesburg (11% in 2004; 32% in 2007).118,121,122 The STI Reference Centre has conducted additional surveys in Kimberley (2006), Bloemfontein (2008), East London (2010), Rustenburg (2011) and Polokwane (2011), and observed a QRNG prevalence of 53%, 16%, 41%, 15% and 40% respectively (D A Lewis, unpublished data).
There is substantial public health concern about the global spread of gonococci with decreased susceptibility to oral cephalosporins which have resulted in gonorrhoea treatment failures in several countries, including Japan, China, Australia, Norway and the UK.123-126 Japan, China and Australia therefore now use intramuscular ceftriaxone to treat gonorrhoea.127 To date there has been no confirmed case of clinical failure with oral cephalosporins in Africa, but such strains will undoubtedly emerge over time, either through importation or de novo. All gonococci tested in South African surveys carried out by the STI Reference Centre (STIRC) over the past 5 years have remained fully susceptible to both cefixime and ceftriaxone (D A Lewis, unpublished data).
In terms of other antimicrobials, studies from Gauteng have confirmed that tetracyclines and penicillin should not be used to treat gonorrhoea in South Africa because of a high prevalence of plasmid-mediated tetracycline resistance (36 - 74%) and a lower, but still unacceptably high, prevalence of penicillinase-producing gonococci (16 - 26%).121,128 Gonococci isolated in Johannesburg in 2008 demonstrate no resistance as yet to azithromycin, spectinomycin and gentamicin (D A Lewis, unpublished data).
Where bacterial STI pathogens are resistant to treatment, patients may be at increased risk of pathogen-associated complications, such as epididymo-orchitis or pelvic inflammatory disease in the case of antimicrobial-resistant N. gonorrhoeae. From the public health viewpoint, such patients also remain infectious to others for longer and this may increase transmission of the pathogen within the community. STIs are also important co-factors in HIV transmission, and HIV viral loads are increased in cervicovaginal, seminal and ulcer-derived secretions in the presence of other STIs. In the case of gonorrhoea, for example, studies from Malawi demonstrated that urethritis can elevate the seminal HIV viral load approximately 8 times and, even with effective anti-gonococcal treatment, it may take over 3 weeks for the seminal viral loads to decline to levels seen in HIV-infected dermatology patients (controls).129 The risk of HIV transmission may be much greater in HIV-infected individuals with antimicrobial-resistant gonorrhoea, particularly in a country like South Africa where there are an estimated 5.3 million HIV-infected individuals aged 15 years and older.130 Relevant to this argument, the STI Reference Centre demonstrated that the detection of QRNG in men with MUS in Cape Town and Johannesburg was significantly associated with co-infection with HIV.122
Finally, treating patients with resistant STIs will require use of more expensive antimicrobial agents and also, when gonococcal resistance to oral cephalosporins emerges in South Africa, increased use of injectable antimicrobials such as ceftriaxone, spectinomycin or gentamicin. The widespread use of intramuscular antimicrobial agents to treat index STI patients and their partner(s) may have a deleterious public health effect by reducing patient and sexual partner access because of fears concerning injections. Widespread use of intramuscularly administered antimicrobials also heightens the risk of needle-stick injuries for staff working with STI patients, who are at high risk of being HIV infected.
Hospital-acquired infections
Public sector
According to the 2009 National Health Laboratory Service (NHLS) public sector susceptibility data (Table V), K. pneumoniae remains a highly resistant nosocomial pathogen, with more than 50% of all strains producing ESBLs. These isolates were frequently multiresistant, with only 32 - 63% susceptible to gentamicin and 54 - 80% susceptible to ciprofloxacin.
E. coli strains exhibited less resistance than K. pneumoniae, with 76 - 91% susceptible to gentamicin, 78 - 92% susceptible to ciprofloxacin and only 6 - 16% producing ESBLs. The very high rate of ESBL production (48%) at Chris Hani Baragwanath Hospital (CHBH) remains unexplained.
Patterns of resistance among P. aeruginosa isolates vary between laboratories. Ceftazidime remains the most active agent.
Carbapenem resistance among Acinetobacter spp. is common in the 5 hospitals with major intensive care units, with only 20 - 40% of isolates being susceptible to carbapenems.
Approximately 60% of S. aureus isolates from blood are sensitive to cloxacillin.
Private sector
For several reasons, including selective pressure from overuse of antibiotics and failure of hospital infection control practices, the incidence of colonisation and infection, particularly with resistant Gram-negative bacteria, in South African private institutions appears to be increasing. In addition, the worldwide emergence and spread of carbapenem-resistant K. pneumoniae and E. coli and reports of hospital outbreaks owing to such strains is cause for local concern.131,132 Increased use of carbapenems in the private sector in South Africa is driven by an increase in cephalosporin and fluoroquinolone resistance among ESBL-producing Enterobacteriaceae.133 Although extensive published data regarding antibiotic susceptibility of community-acquired respiratory tract pathogens especially S. pneumoniae are available, including those of invasive isolates, few data have been published for Gram-negative pathogens such as A. baumannii or P. aeruginosa or for Gram-positive pathogens, particularly S. aureus.
The SENTRY international antimicrobial surveillance programme documented the prevalence of ESBL production in Enterobacter cloacae among hospitalised patients in several Johannesburg private hospitals as 20% (N=11/54) and that of oxacillin resistance in blood-culture isolates of nosocomially acquired S. aureus to be 40%.134,135 A 2006 survey of bacteraemic pathogens isolated from patients in private hospitals in 5 major South African cities conducted by the former National Antibiotic Surveillance Forum (NASF), found that nationwide prevalence of ampicillin resistance in blood culture isolates of E. coli (N=471) was 84%, and 20% were resistant to fluoroquinolones (Table VI).136 Cephalosporin resistance among isolates of K. pneumoniae (N=636) was high; 52% were resistant to cefuroxime. The most active agents in Enterobacter spp. (N=242) were imipenem/meropenem, ertapenem, ciprofloxacin and levofloxacin, with 100%, 94%, 88% and 87% susceptibility, respectively. Carbapenem resistance in invasive isolates of P. aeruginosa (N=382) varied between 45% and 42% for imipenem and meropenem and in A. baumannii (N=190) between 33% and 32%, respectively. The overall incidence of methicillin resistance among S. aureus isolates was 36% (N=629). The prevalence of ESBL production among allsource isolates of K. pneumoniae (N=7 514), Enterobacter spp. (N= 4 031) and E.coli (N=28 412) was 26%, 12% and 5%, respectively.
References
1. Norman R, Bradshaw D, Schneider M, Pieterse D, Groenewald P. Revised Burden of Disease Estimates for the Comparative Risk Factor Assessment, South Africa 2000. Methodological Note. Cape Town: South African Medical Research Council, Unit BoDR, 2006:22. [ Links ]
2. Day C, Gray A. Chapter 21: Health and Related Indicators, p 283. In: Fonn A, Padarath A, eds. South African Health Review. Durban: Health Systems Trust, 2010. [ Links ]
3. BMI. South Africa Pharmaceuticals and Healthcare Report. London: 2010. [ Links ]
4. Musher DM. Infections caused by Streptococcus pneumoniae: clinical spectrum, pathogenesis, immunity, and treatment. Clin Infect Dis 1992;14(4):801-807. [ Links ]
5. World Health Organization. Pneumococcal conjugate vaccine for childhood immunization: WHO position paper. Wkly Epidemiol Rec 2007 Mar 23;82(12):93-104. [ Links ]
6. World Health Organization. Management of the young child with an acute respiratory infection. Program for control of acute respiratory infections. Geneva: WHO, 1990. [ Links ]
7. Du Plessis M, Smith AM, Klugman KP. Rapid detection of penicillin-resistant Streptococcus pneumoniae in cerebrospinal fluid by a seminested-PCR strategy. J Clin Microbiol 1998;36(2):453-457. [ Links ]
8. Hansman D, Bullen M. A resistant pneumococcus. Lancet 1967;2:264-265. [ Links ]
9. Appelbaum PC, Bhamjee A, Scragg JN, Hallett AF, Bowen AJ, Cooper RC. Streptococcus pneumoniae resistant to penicillin and chloramphenicol. Lancet 1977;2:995-997. [ Links ]
10. Jacobs MR, Koornhof HJ. Multiple-antibiotic resistance - now the pneumococcus. J Antimicrob Chemother 1978;4(6):481-483. [ Links ]
11. Jacobs MR, Koornhof HJ, Robins-Browne RM, et al. Emergence of multiply resistant pneumococci. N Engl J Med 1978;299(14):735-740. [ Links ]
12. Allen KD. Penicillin-resistant pneumococci. J Hosp Infect 1991;17(1):3-13. [ Links ]
13. Friedland IR, Klugman KP. Failure of chloramphenicol therapy in penicillin-resistant pneumococcal meningitis. Lancet 1992;339:405-408. [ Links ]
14. Klugman KP, Walsh AL, Phiri A, Molyneux EM. Mortality in penicillin-resistant pneumococcal meningitis. Pediatr Infect Dis J 2008;27(7):671-672. [ Links ]
15. Dagan R, Leibovitz E, Leiberman A, Yagupsky P. Clinical significance of antibiotic resistance in acute otitis media and implication of antibiotic treatment on carriage and spread of resistant organisms. Pediatr Infect Dis J 2000;19(5Suppl):S57-65. [ Links ]
16. Catalan MJ, Fernandez JM, Vazquez A, Varela de Seijas E, Suarez A, Bernaldo de Quiros JC. Failure of cefotaxime in the treatment of meningitis due to relatively resistant Streptococcus pneumoniae. Clin Infect Dis 1994;18(5):766-769. [ Links ]
17. Klugman KP. Bacteriological evidence of antibiotic failure in pneumococcal lower respiratory tract infections. Eur Respir J Suppl 2002;36:3s-8s. [ Links ]
18. Weinstein MP, Klugman KP, Jones RN. Rationale for revised penicillin susceptibility breakpoints versus Streptococcus pneumoniae: coping with antimicrobial susceptibility in an era of resistance. Clin Infect Dis 2009;48(11):1596-1600. [ Links ]
19. McGee L, McDougal L, Zhou J, et al. Nomenclature of major antimicrobial-resistant clones of Streptococcus pneumoniae defined by the pneumococcal molecular epidemiology network. J Clin Microbiol 2001;39(7):2565-2571. [ Links ]
20. Benbachir M, Benredjeb S, Boye CS, et al. Two-year surveillance of antibiotic resistance in Streptococcus pneumoniae in four African cities. Antimicrob Agents Chemother 2001;45(2):627-629. [ Links ]
21. Ramdani-Bouguessa N, Rahal K. Serotype distribution and antimicrobial resistance of Streptococcus pneumoniae isolated in Algiers, Algeria. Antimicrob Agents Chemother 2003;47(2):824-826. [ Links ]
22. Wasfy MO, Pimentel G, Abdel-Maksoud M, et al. Antimicrobial susceptibility and serotype distribution of Streptococcus pneumoniae causing meningitis in Egypt, 1998-2003. J Antimicrob Chemother 2005;55(6):958-964. [ Links ]
23. Ohene A. Bacterial pathogens and their antimicrobial susceptibility in Kumasi, Ghana. East Afr Med J 1997;74(7):450-455. [ Links ]
24. Adegbola RA, Hill PC, Secka O, et al. Serotype and antimicrobial susceptibility patterns of isolates of Streptococcus pneumoniae causing invasive disease in The Gambia 1996-2003. Trop Med Int Health 2006;11(7):1128-1135. [ Links ]
25. Erqou S, Kebede Y, Mulu A. Increased resistance of Streptococcus pneumoniae isolates to antimicrobial drugs, at a referral hospital in north-west Ethiopia. Trop Doct 2008;38(2):110-112. [ Links ]
26. Felmingham D, Gruneberg RN. The Alexander Project 1996-1997: latest susceptibility data from this international study of bacterial pathogens from community-acquired lower respiratory tract infections. J Antimicrob Chemother 2000;45(2):191-203. [ Links ]
27. Muhe L, Klugman KP. Pneumococcal and Haemophilus influenzae meningitis in a children's hospital in Ethiopia: serotypes and susceptibility patterns. Trop Med Int Health 1999;4(6):421-427. [ Links ]
28. Feikin DR, Davis M, Nwanyanwu OC, et al. Antibiotic resistance and serotype distribution of Streptococcus pneumoniae colonizing rural Malawian children. Pediatr Infect Dis J 2003;22(6):564-567. [ Links ]
29. Woolfson A, Huebner R, Wasas A, Chola S, Godfrey-Faussett P, Klugman K. Nasopharyngeal carriage of community-acquired, antibiotic-resistant Streptococcus pneumoniae in a Zambian paediatric population. Bull World Health Organ 1997;75(5):453-462. [ Links ]
30. Valles X, Flannery B, Roca A, et al. Serotype distribution and antibiotic susceptibility of invasive and nasopharyngeal isolates of Streptococcus pneumoniae among children in rural Mozambique. Trop Med Int Health 2006;11(3):358-366. [ Links ]
31. Felmingham D, Feldman C, Hryniewicz W, et al. Surveillance of resistance in bacteria causing community-acquired respiratory tract infections. Clin Microbiol Infect 2002;8 Suppl 2:12-42. [ Links ]
32. Klugman KP, Koornhof HJ. Drug resistance patterns and serogroups or serotypes of pneumococcal isolates from cerebrospinal fluid or blood, 1979-1986. J Infect Dis 1988;158(5):956-964. [ Links ]
33. Koornhof HJ, Wasas A, Klugman K. Antimicrobial resistance in Streptococcus pneumoniae: a South African perspective. Clin Infect Dis 1992;15(1):84-94. [ Links ]
34. Huebner RE, Wasas AD, Klugman KP. Trends in antimicrobial resistance and serotype distribution of blood and cerebrospinal fluid isolates of Streptococcus pneumoniae in South Africa, 1991-1998. Int J Infect Dis 2000;4(4):214-218. [ Links ]
35. Huebner RE, Wasas AD, Klugman KP. Prevalence of nasopharyngeal antibiotic-resistant pneumococcal carriage in children attending private paediatric practices in Johannesburg. S Afr Med J 2000;90(11):1116-1121. [ Links ]
36. Liebowitz LD, Slabbert M, Huisamen A. National surveillance programme on susceptibility patterns of respiratory pathogens in South Africa: moxifloxacin compared with eight other antimicrobial agents. J Clin Pathol 2003;56(5):344-347. [ Links ]
37. Buie KA, Klugman KP, von Gottberg A, et al. Gender as a risk factor for both antibiotic resistance and infection with pediatric serogroups/serotypes, in HIV-infected and -uninfected adults with pneumococcal bacteremia. J Infect Dis 2004;189(11):1996-2000. [ Links ]
38. Pemba L, Charalambous S, von Gottberg A, et al. Impact of cotrimoxazole on non-susceptibility to antibiotics in Streptococcus pneumoniae carriage isolates among HIV-infected mineworkers in South Africa. J Infect 2008;56(3):171-178. [ Links ]
39. Feldman C, Brink AJ, von Gottberg A, et al. Antimicrobial susceptibility of pneumococcal isolates causing bacteraemic pneumococcal pneumonia: analysis using current breakpoints and fluoroquinolone pharmacodynamics. Int J Antimicrob Agents 2010;36(1):95-97. [ Links ]
40. Campbell GD, Jr., Silberman R. Drug-resistant Streptococcus pneumoniae. Clin Infect Dis 1998;26(5):1188-1195. [ Links ]
41. Doern GV, Brueggemann AB, Huynh H, Wingert E. Antimicrobial resistance with Streptococcus pneumoniae in the United States, 1997-98. Emerg Infect Dis 1999;5(6):757-765. [ Links ]
42. Fenoll A, Gimenez MJ, Robledo O, et al. Influence of penicillin/amoxicillin non-susceptibility on the activity of third-generation cephalosporins against Streptococcus pneumoniae. Eur J Clin Microbiol Infect Dis 2008;27(1):75-80. [ Links ]
43. Whitney CG, Farley MM, Hadler J, et al. Increasing prevalence of multidrug-resistant Streptococcus pneumoniae in the United States. N Engl J Med 2000;343(26):1917-1924. [ Links ]
44. Wolter N, von Gottberg A, du Plessis M, de Gouveia L, Klugman KP. Molecular basis and clonal nature of increasing pneumococcal macrolide resistance in South Africa, 2000-2005. Int J Antimicrob Agents 2008;32(1):62-67. [ Links ]
45. Klugman KP, Koornhof HJ, Kuhnle V. Clinical and nasopharyngeal isolates of unusual multiply resistant pneumococci. Am J Dis Child 1986;140(11):1186-1190. [ Links ]
46. Klugman KP, Koornhof HJ, Wasas A, Storey K, Gilbertson I. Carriage of penicillin resistant pneumococci. Arch Dis Child 1986;61(4):377-381. [ Links ]
47. Chen DK, McGeer A, de Azavedo JC, Low DE. Decreased susceptibility of Streptococcus pneumoniae to fluoroquinolones in Canada. Canadian Bacterial Surveillance Network. N Engl J Med 1999;341(4):233-239. [ Links ]
48. Von Gottberg A, Klugman KP, Cohen C, et al. Emergence of levofloxacin-non-susceptible Streptococcus pneumoniae and treatment for multidrug-resistant tuberculosis in children in South Africa: a cohort observational surveillance study. Lancet 2008;371(9618):1108-1113. [ Links ]
49. Felmingham D. Comparative antimicrobial susceptibility of respiratory tract pathogens. Chemotherapy 2004;50 Suppl 1:3-10. [ Links ]
50. Siira L, Rantala M, Jalava J, et al. Temporal trends of antimicrobial resistance and clonality of invasive Streptococcus pneumoniae isolates in Finland, 2002 to 2006. Antimicrob Agents Chemother 2009;53(5):2066-2073. [ Links ]
51. Syrogiannopoulos GA, Grivea IN, Davies TA, Katopodis GD, Appelbaum PC, Beratis NG. Antimicrobial use and colonization with erythromycin-resistant Streptococcus pneumoniae in Greece during the first 2 years of life. Clin Infect Dis 2000;31(4):887-893. [ Links ]
52. Okeke IN, Laxminarayan R, Bhutta ZA, et al. Antimicrobial resistance in developing countries. Part I: recent trends and current status. Lancet Infect Dis 2005;5(8):481-493. [ Links ]
53. Zerouali K, Elmdaghri N, Boudouma M, Benbachir M. Serogroups, serotypes, serosubtypes and antimicrobial susceptibility of Neisseria meningitidis isolates in Casablanca, Morocco. Eur J Clin Microbiol Infect Dis 2002;21(6):483-485. [ Links ]
54. Afifi S, Wasfy MO, Azab MA, et al. Laboratory-based surveillance of patients with bacterial meningitis in Egypt (1998-2004). Eur J Clin Microbiol Infect Dis 2007;26(5):331-340. [ Links ]
55. Gagneux S, Hodgson A, Ehrhard I, et al. Microheterogeneity of serogroup A (subgroup III) Neisseria meningitidis during an outbreak in northern Ghana. Trop Med Int Health 2000 Apr;5(4):280-287. [ Links ]
56. Norheim G, Rosenqvist E, Aseffa A, et al. Characterization of Neisseria meningitidis isolates from recent outbreaks in Ethiopia and comparison with those recovered during the epidemic of 1988 to 1989. J Clin Microbiol 2006;44(3):861-871. [ Links ]
57. Emele FE. Etiologic spectrum and pattern of antimicrobial drug susceptibility in bacterial meningitis in Sokoto, Nigeria. Acta Paediatr 2000;89(8):942-946. [ Links ]
58. Botha P. Penicillin-resistant Neisseria meningitidis in southern Africa. Lancet 1988;1:54. [ Links ]
59. Du Plessis M, von Gottberg A, Cohen C, de Gouveia L, Klugman KP. Neisseria meningitidis intermediately resistant to penicillin and causing invasive disease in South Africa in 2001 to 2005. J Clin Microbiol 2008;46(10):3208-3214. [ Links ]
60. Du Plessis M, de Gouveia L, Skosana H, et al. Invasive Neisseria meningitidis with decreased susceptibility to fluoroquinolones in South Africa, 2009. J Antimicrob Chemother 2010;65(10):22582260. [ Links ]
61. Cardines R, Giufre M, Mastrantonio P, Ciofi degli Atti ML, Cerquetti M. Nontypeable Haemophilus influenzae meningitis in children: phenotypic and genotypic characterization of isolates. Pediatr Infect Dis J 2007;26(7):577-582. [ Links ]
62. World Health Organization. Haemophilus influenzae Type B (HiB): WHO Fact Sheet. Geneva: World Health Organization, 2005. [ Links ]
63. Peltola H. Worldwide Haemophilus influenzae type b disease at the beginning of the 21st century: global analysis of the disease burden 25 years after the use of the polysaccharide vaccine and a decade after the advent of conjugates. Clin Microbiol Rev 2000;13(2):302-317. [ Links ]
64. Mulholland K, Hilton S, Adegbola R, et al. Randomised trial of Haemophilus influenzae type-b tetanus protein conjugate vaccine [corrected] for prevention of pneumonia and meningitis in Gambian infants. Lancet 1997;349:1191-1197. [ Links ]
65. Mwangi I, Berkley J, Lowe B, Peshu N, Marsh K, Newton CR. Acute bacterial meningitis in children admitted to a rural Kenyan hospital: increasing antibiotic resistance and outcome. Pediatr Infect Dis J 2002;21(11):1042-1048. [ Links ]
66. Tomeh MO, Starr SE, McGowan JE, Jr., Terry PM, Nahmias AJ. Ampicillin-resistant Haemophilus influenzae type B infection. JAMA 1974;229(3):295-297. [ Links ]
67. Cerquetti M, Cardines R, Giufre M, Mastrantonio P. Antimicrobial susceptibility of Haemophilus influenzae strains isolated from invasive disease in Italy. J Antimicrob Chemother 2004;54(6):11391143. [ Links ]
68. Tamargo I, Fuentes K, Llop A, Oteo J, Campos J. High levels of multiple antibiotic resistance among 938 Haemophilus influenzae type b meningitis isolates from Cuba (1990-2002). J Antimicrob Chemother 2003;52(4):695-698. [ Links ]
69. Roca A, Quinto L, Abacassamo F, et al. Invasive Haemophilus influenzae disease in children less than 5 years of age in Manhica, a rural area of southern Mozambique. Trop Med Int Health 2008;13(6):818-826. [ Links ]
70. Scott JA, Mwarumba S, Ngetsa C, et al. Progressive increase in antimicrobial resistance among invasive isolates of Haemophilus influenzae obtained from children admitted to a hospital in Kilifi, Kenya, from 1994 to 2002. Antimicrob Agents Chemother 2005;49(7):3021-3024. [ Links ]
71. Brink AJ, Cotton MF, Feldman C, et al. Guideline for the management of upper respiratory tract infections. S Afr Med J 2004;94(6 Pt 2):475-483. [ Links ]
72. Feldman C, Brink AJ, Richards GA, Maartens G, Bateman ED. Working Group of the South African Thoracic Society. Management of community-acquired pneumonia in adults. S Afr Med J 2007;97(12):1296-1304 [ Links ]
73. Daza P, Banda R, Misoya K, et al. The impact of routine infant immunization with Haemophilus influenzae type b conjugate vaccine in Malawi, a country with high human immunodeficiency virus prevalence. Vaccine 2006;24(37-39):6232-6239. [ Links ]
74. Ndiaye G, Edwige H, Guèye FB, Boye CSB. Trend in antibiotic resistance of Streptococcus pneumoniae and Haemophilus influenzae strains isolated from community acquired respiratory tract infections in Dakar, Senegal between 2005 and 2008. Microbiology Insights 2010;3:45-52. [ Links ]
75. Fali A, du Plessis M, Wolter N, Klugman KP, von Gottberg A. Single report of beta-lactam resistance in an invasive Haemophilus influenzae isolate from South Africa mediated by mutations in penicillinbinding protein 3, 2003-2008. Int J Antimicrob Agents 2010;36(5):480-482. [ Links ]
76. Garcia-Cobos S, Campos J, Lazaro E, et al. Ampicillin-resistant non-beta-lactamase-producing Haemophilus influenzae in Spain: recent emergence of clonal isolates with increased resistance to cefotaxime and cefixime. Antimicrob Agents Chemother 2007;51(7):2564-25673. [ Links ]
77. Matic V, Bozdogan B, Jacobs MR, Ubukata K, Appelbaum PC. Contribution of beta-lactamase and PBP amino acid substitutions to amoxicillin/clavulanate resistance in beta-lactamase-positive, amoxicillin/ clavulanate-resistant Haemophilus influenzae. J Antimicrob Chemother 2003;52(6):1018-1021. [ Links ]
78. Osaki Y, Sanbongi Y, Ishikawa M, et al. Genetic approach to study the relationship between penicillinbinding protein 3 mutations and Haemophilus influenzae beta-lactam resistance by using site-directed mutagenesis and gene recombinants. Antimicrob Agents Chemother 2005;49(7):2834-2839. [ Links ]
79. Jansen WT, Verel A, Beitsma M, Verhoef J, Milatovic D. Longitudinal European surveillance study of antibiotic resistance of Haemophilus influenzae. J Antimicrob Chemother 2006;58(4):873-877. [ Links ]
80. Kaczmarek FS, Gootz TD, Dib-Hajj F, Shang W, Hallowell S, Cronan M. Genetic and molecular characterization of beta-lactamase-negative ampicillin-resistant Haemophilus influenzae with unusually high resistance to ampicillin. Antimicrob Agents Chemother 2004;48(5):1630-1639. [ Links ]
81. Kim IS, Ki CS, Kim S, et al. Diversity of ampicillin resistance genes and antimicrobial susceptibility patterns in Haemophilus influenzae strains isolated in Korea. Antimicrob Agents Chemother 2007;51(2):453-460. [ Links ]
82. Mandomando I, Sigauque B, Morais L, et al. Antimicrobial drug resistance trends of bacteremia isolates in a rural hospital in southern Mozambique. Am J Trop Med Hyg 2010;83(1):152-157. [ Links ]
83. Molyneux E, Walsh A, Phiri A, Molyneux M. Acute bacterial meningitis in children admitted to the Queen Elizabeth Central Hospital, Blantyre, Malawi in 1996-97. Trop Med Int Health 1998;3(8):610-618. [ Links ]
84. Ndip RN, Ntiege EA, Ndip LM, Nkwelang G, Akoachere JF, Akenji TN. Antimicrobial resistance of bacterial agents of the upper respiratory tract of school children in Buea, Cameroon. J Health Popul Nutr 2008;26(4):397-404. [ Links ]
85. Turnidge J, Bell J. Emerging beta-lactamase-negative ampicillin resistant Haemophilus influenzae in Japan and South Africa (Abstract). Chicago: 43rd Interscience Conference on Antimicrobial Agents and Chemotherapy, 14-17 September 2003:C2-1268. [ Links ]
86. Parry CM, Threlfall EJ. Antimicrobial resistance in typhoidal and nontyphoidal salmonellae. Curr Opin Infect Dis [Review] 2008;21(5):531-538. [ Links ]
87. Smith AM, Govender N, Keddy KH. Quinolone-resistant Salmonella typhi in South Africa, 2003-2007. Epidemiol Infect 2010;138(1):86-90. [ Links ]
88. Govender N, Smith AM, Karstaedt AS, Keddy KH. Plasmid-mediated quinolone resistance in Salmonella from South Africa. J Med Microbiol 2009;58(Pt10):1393-1394. [ Links ]
89. Kruger T, Szabo D, Keddy KH, et al. Infections with nontyphoidal Salmonella species producing TEM-63 or a novel TEM enzyme, TEM-131, in South Africa. Antimicrob Agents Chemother 2004;48(11):4263-4270. [ Links ]
90. Govinden U, Mocktar C, Moodley P, Sturm AW, Essack SY. CTX-M-37 in Salmonella enterica serotype Isangi from Durban, South Africa. Int J Antimicrob Agents 2006;28(4):288-291. [ Links ]
91. Govinden U, Mocktar C, Moodley P, Sturm A, Essack S. Detection of mutations in the gyrA of clinical Salmonella spp. African Journal of Biotechnology 2009;8(16):3911-3914. [ Links ]
92. Crump JA, Luby SP, Mintz ED. The global burden of typhoid fever. Bull World Health Organ 2004;82(5):346-353. [ Links ]
93. Aarestrup FM, Wiuff C, Molbak K, Threlfall EJ. Is it time to change fluoroquinolone breakpoints for Salmonella spp.? Antimicrob Agents Chemother 2003;47(2):827-829. [ Links ]
94. Keddy KH, Smith AM, Sooka A, Ismail H, Oliver S. Fluoroquinolone-resistant typhoid, South Africa. Emerg Infect Dis 2010;16(5):879-880. [ Links ]
95. Pfeifer Y, Matten J, Rabsch W. Salmonella enterica serovar Typhi with CTX-M beta-lactamase, Germany. Emerg Infect Dis 2009;15(9):1533-1535. [ Links ]
96. Mahon C, Lehman D, Manuselis G. Enterobacteriaceae, Shigella. Diagnostic Microbiology, 3rd ed. St. Louis: Saunders Elsevier; 2007:521-523. [ Links ]
97. Smith AM, Keddy KH, Sooka A, Ismail H, Dejong GM. Analysis of a temporal cluster of Shigella boydii isolates in Mpumalanga, South Africa, November to December 2007. J Infect Dev Ctries 2009;3(1):65-70. [ Links ]
98. Mahon C, Lehman D, Manuselis G. Vibrio, Aeromonas and Campylobacter species. In: Diagnostic Microbiology. 3rd ed. St Louis: Saunders Elseiver; 2007:521-523. [ Links ]
99. Heymann D. Vibrio cholerae serogroups 01 and 0139. In: Control of Communicable Diseases Manual. 19th ed. Washington, DC: American Public Health Association, 2008:120-128. [ Links ]
100. Keddy K. Cholera outbreak in South Africa: extended laboratory characterisation of isolates. In: National Health Laboratory Service - Annual report 2009/2010. Sandringham, GA: National Health Laboratory Service, 2010:112. [ Links ]
101. Keddy K. Molecular characterisation of multidrug resistant cholera outbreak isolates. In: National Health Laboratory Service - Annual report 2009/2010. Sandringham, GA: National Health Laboratory Service, 2010:112. [ Links ]
102. Mahon C, Lehman D, Manuselis G. Enterobacteriaceae, Escherichia coli. Diagnostic Microbiology. 3rd ed. St. Louis: Saunders Elseiver, 2007:505-512. [ Links ]
103. Heymann D. Diarrhea, acute - diarrhea caused by Escherichia coli. In: Control of Communicable Diseases Manual. 19th ed. Washington, DC: American Public Health Association, 2008:181-195. [ Links ]
104. Peirano G, van Greune CH, Pitout JD. Characteristics of infections caused by extended-spectrum beta-lactamase-producing Escherichia coli from community hospitals in South Africa. Diagn Microbiol Infect Dis 2011;69(4):449-453. [ Links ]
105. Fleming DT, Wasserheit JN. From epidemiological synergy to public health policy and practice: the contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Transm Infect 1999;75(1):3-17. [ Links ]
106. Telzak EE, Spitalny KC, Faur YC, et al. Risk factors for infection with plasmid-mediated high-level tetracycline resistant Neisseria gonorrhoeae. Sex Transm Dis 1989;16(3):132-136. [ Links ]
107. Pettifor A, Walsh J, Wilkins V, Raghunathan P. How effective is syndromic management of STDs? A review of current studies. Sex Transm Dis 2000;27(7):371-385. [ Links ]
108. Sahin-Hodoglugil NN, Woods R, Pettifor A, Walsh J. A comparison of cost-effectiveness of three protocols for diagnosis and treatment of gonococcal and chlamydial infections in women in Africa. Sex Transm Dis 2003;30(5):455-469. [ Links ]
109. Schneider H, Blaauw D, Dartnall E, Coetzee DJ, Ballard RC. STD care in the South African private health sector. S Afr Med J 2001;91(2):151-156. [ Links ]
110. Chabikuli N, Schneider H, Blaauw D, Zwi AB, Brugha R. Quality and equity of private sector care for sexually transmitted diseases in South Africa. Health Policy Plan 2002;17 Suppl:40-46. [ Links ]
111. Schneider H, Chabikuli N, Blaauw D, Funani I, Brugha R. Sexually transmitted infections - factors associated with quality of care among private general practitioners. S Afr Med J 2005;95(10):782-785. [ Links ]
112. Suchland RJ, Sandoz KM, Jeffrey BM, Stamm WE, Rockey DD. Horizontal transfer of tetracycline resistance among Chlamydia spp. in vitro. Antimicrob Agents Chemother 2009;53(11):4604-4611. [ Links ]
113. Somani J, Bhullar VB, Workowski KA, Farshy CE, Black CM. Multiple drug-resistant Chlamydia trachomatis associated with clinical treatment failure. J Infect Dis 2000;181(4):1421-1427. [ Links ]
114. Bjornelius E, Anagrius C, Bojs G, et al. Antibiotic treatment of symptomatic Mycoplasma genitalium infection in Scandinavia: a controlled clinical trial. Sex Transm Infect 2008;84(1):72-76. [ Links ]
115. Hamasuna R, Osada Y, Jensen JS. Antibiotic susceptibility testing of Mycoplasma genitalium by TaqMan 5' nuclease real-time PCR. Antimicrob Agents Chemother 2005;49(12):4993-4998. [ Links ]
116. Lukehart SA, Godornes C, Molini BJ, et al. Macrolide resistance in Treponema pallidum in the United States and Ireland. N Engl J Med 2004;351(2):154-158. [ Links ]
117. Dangor Y, Miller SD, Exposto Fda L, Koornhof HJ. Antimicrobial susceptibilities of southern African isolates of Haemophilus ducreyi. Antimicrob Agents Chemother 1988;32(9):1458-1460. [ Links ]
118. Moodley P, Sturm AW. Ciprofloxacin-resistant gonorrhoea in South Africa. Lancet 2005;366(9492):1159. [ Links ]
119. Lewis D. Antibiotic resistant gonococci - past, present and future. S Afr Med J 2007;97:1146-1150. [ Links ]
120. National Department of Health. First Line Comprehensive Management and Control of Sexually Transmitted Infections (STIs): Protocol for the Management of a Person with a Sexually Transmitted Infection according to the Essential Drugs List. Pretoria: National Department of Health, 2008. [ Links ]
121. De Jongh M, Dangor Y, Adam A, Hoosen AA. Gonococcal resistance: evolving from penicillin, tetracycline to the quinolones in South Africa - implications for treatment guidelines. Int J STD AIDS 2007;18(10):697-699. [ Links ]
122. Lewis DA, Scott L, Slabbert M, et al. Escalation in the relative prevalence of ciprofloxacin-resistant gonorrhoea among men with urethral discharge in two South African cities: association with HIV seropositivity. Sex Transm Infect 2008;84(5):352-355. [ Links ]
123. Deguchi T, Yasuda M, Yokoi S, et al. Treatment of uncomplicated gonococcal urethritis by doubledosing of 200 mg cefixime at a 6-h interval. J Infect Chemother 2003;9(1):35-39. [ Links ]
124. Lewis DA. The gonococcus fights back: is this time a knock out? Sex Transm Infect 2010;86(6):415- 421. [ Links ]
125. Unemo M, Golparian D, Syversen G, Vestrheim DF, Moi H. Two cases of verified clinical failures using internationally recommended first-line cefixime for gonorrhoea treatment, Norway, 2010. Euro Surveill 2010;15(47):pii=19721. [ Links ]
126. Ison CA, Hussey J, Sankar KN, Evans J, Alexander S. Gonorrhoea treatment failures to cefixime and azithromycin in England, 2010. Euro Surveill 2011;16(14):pii=19833. [ Links ]
127. Tapsall JW. Implications of current recommendations for third-generation cephalosporin use in the WHO Western Pacific Region following the emergence of multiresistant gonococci. Sex Transm Infect 2009;85(4):256-258. [ Links ]
128. Fayemiwo S, Müller E, Gumede L, Lewis D. Plasmid-mediated penicillin and tetracycline resistance among Neisseria gonorrhoeae isolates in South Africa: Prevalence, detection and typing using a novel molecular assay. Sex Transm Dis 2011;38:329-333. [ Links ]
129. Cohen MS, Hoffman IF, Royce RA, et al. Reduction of concentration of HIV-1 in semen after treatment of urethritis: implications for prevention of sexual transmission of HIV-1. AIDSCAP Malawi Research Group. Lancet 1997;349(9069):1868-1873. [ Links ]
130. UNAIDS. Global Report: UNAIDS Report on the Global AIDS Epidemic 2010. Geneva: UNAIDS, 2010:1-100. http://www.unaids.org/globalreport/documents/20101123_GlobalReport_full_en.pdf (accessed 22 June 2011). [ Links ]
131. Kumarasamy KK, Toleman MA, Walsh TR, et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study. Lancet Infect Dis 2010;10(9):597-602. [ Links ]
132. Nordmann P, Cuzon G, Naas T. The real threat of Klebsiella pneumoniae carbapenemase-producing bacteria. Lancet Infect Dis 2009;9(4):228-236. [ Links ]
133. Elliott E, Brink AJ, van Greune J, et al. In vivo development of ertapenem resistance in a patient with pneumonia caused by Klebsiella pneumoniae with an extended-spectrum beta-lactamase. Clin Infect Dis 2006;42(11):e95-98. [ Links ]
134. Bell JM, Turnidge JD, Jones RN. Prevalence of extended-spectrum beta-lactamase-producing Enterobacter cloacae in the Asia-Pacific region: results from the SENTRY Antimicrobial Surveillance Program, 1998 to 2001. Antimicrob Agents Chemother 2003;47(12):3989-3993. [ Links ]
135. Bell JM, Turnidge JD. High prevalence of oxacillin-resistant Staphylococcus aureus isolates from hospitalized patients in Asia-Pacific and South Africa: results from SENTRY antimicrobial surveillance program, 1998-1999. Antimicrob Agents Chemother 2002;46(3):879-881. [ Links ]
136. Brink AJ, Moolman J, Cruz da Silva M, and the National Antibiotic Surveillance Forum. Antimicrobial susceptibility profile of selected bacteraemic pathogens from private institutions in South Africa. S Afr Med J 2007;97:630-636. [ Links ]


{kind=link}
{kind=link}
{kind=link}
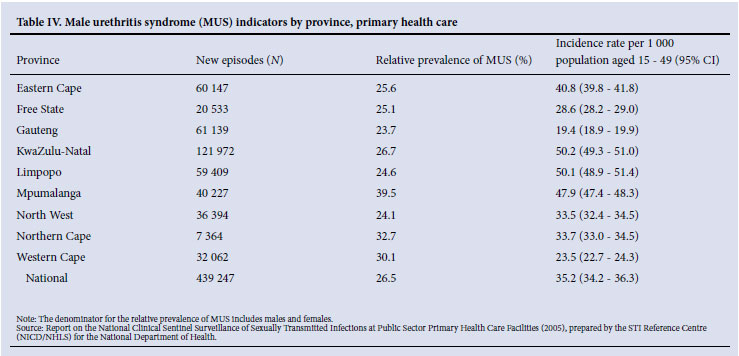{kind=link}
{kind=link}
{kind=link}