










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.8 Pretoria Ago. 2011
ORIGINAL ARTICLES
Part III. Antibiotic supply chain and management in human health
S Y Essack; N Schellack; T Pople; L van der Merwe; F Suleman; J C Meyer; A G S Gous; D Benjamin
Keywords: drug supply chain; drug procurement; antibiotics; Essential Drugs List; Standard Treatment Guidelines; pharmaceutical industry; antibiotic prescribing; antibiotic pricing
This section examines the regulatory environment and supply chain for antibiotics for both the public and private sectors, followed by a review of what is known about patterns of antibiotic consumption in South Africa. It provides information pertaining to national policy documents and their relationship with drug supply and distribution, the position of antibiotics in therapeutic guidelines and dispensing regulations, and the current status of pharmaceutical management.
Policy framework for antibiotic management
The South African drug regulatory system is conceptualised in the National Drug Policy (NDP), published in 1996. The National Department of Health (NDoH) aimed to address previous structured inequalities and inaccessibility to medicines with the implementation of the NDP, hoping to ensure '... adequate and reliable supply of safe, cost-effective drugs of acceptable quality to all citizens of South Africa and the rational use of drugs by prescribers, dispensers and consumers'.1 The NDP outlines specific health, economic and national development objectives, including the availability and accessibility of essential medicines, the safety and quality of medicines, good dispensing and prescribing practices, and individual responsibility for health and informed decision-making. Other policies have also expressed economic goals such as promoting cost-effective use of medicines and establishing advisory groups for pharmaco-economics.
The Medicines and Related Substances Control Act 101 of 1965 (as amended) makes provision for the registration and control of medicines, as well as the licensing of professionals to dispense and manufacture them.2 Those permitted to prescribe and dispense medicines are registered by their Professional Councils as enacted by the Pharmacy Act 53 of 1974, the Health Professions Act 56 of 1974, the Veterinary and Para-Veterinary Professions Act 19 of 1982, the Allied Health Professions Act 63 of 1982 and the Nursing Act 33 of 2005.
Quality control and efficacy of medicines Regulatory authorities
The NDP aim of ensuring 'that drugs reaching patients are safe, effective and meet the approved standards' relates to the core pharmaceutical aspects of medicine quality, safety and efficacy and falls under the mandate of the Medicines Control Council (MCC). The MCC is responsible for the registration and re-licensing (retention) of medicines, dossier-based medicine evaluations and laboratory-based testing of all medicines used in South Africa in compliance with criteria for medicine evaluation and good manufacturing practice (GMP). The MCC subscribes to the World Health Organization (WHO)'s Certification Scheme for the Quality of Pharmaceuticals Moving in International Commerce, the Guidelines for Donated Drugs, the Model List of Items to be Included in a Clinical Trial Protocol and the Ethical Criteria for Medicinal Drug Promotion. When necessary, the MCC may implement need-based prioritisation of medicine registration and expedite the registration of essential medicines. The MCC serves as an inspectorate of guideline compliance in government depots, hospital stores and private pharmacies and among dispensing health workers on a provincial level, while retaining the specialised functions of inspecting manufacturing facilities and wholesale premises at a national level.1
Quality assurance requirements
Pharmaceutical and analytical quality assurance requirements of the MCC encompass pharmaceutical and biological availability, details on the active pharmaceutical ingredient, formulation, specifications and control procedures for pharmaceutical ingredients, containers and packaging materials, manufacturing procedures, stability data of the finished pharmaceutical product, pharmaceutical development, and the expertise and premises used for the manufacture of a biological medicine.3 The stability testing and required information endorsed by the MCC is based on the tripartite guideline developed by the Quality Expert working group of the International Conference on Harmonization and is aligned with the Food and Drug Administration and the European Medicines Agency.4 The MCC also stipulates the conditions under which in vivo (clinical trial) and in vitro bio-availability information is acceptable, in addition to stipulating criteria for the design and conduct of studies for orally administered pharmaceutical products, and bio-equivalence requirements.5
Until an independent quality control laboratory is established, universities conduct quality control testing under contract with the MCC. The NDoH has in the past outsourced, on tender, the quality assurance role of the MCC and two institutions were awarded tenders. The Centre for Quality Assurance of Medicines (CENQAM), located on the Potchefstroom campus of North West University, was contracted to perform post-marketing quality control surveillance on pharmaceuticals, while the National Control Laboratory (NCL) at the University of the Free State undertook quality control testing for the batch release of biological medicines and vaccines.6 The last CENQAM contract ended in 1999, and the MCC has since made use of CENQAM services on an ad hoc basis, submitting only samples suspected of being sub-standard for testing.
Counterfeits
Counterfeiting of pharmaceuticals in South Africa is highly problematic, with an estimated one in five medicines sold believed to be counterfeit.7 The majority of counterfeit medicines are imported from India and Pakistan and reach pharmacies through illegal means. The NDoH has a small team investigating the issue, but there had only been one successful prosecution as at 2010.
Pharmacovigilance
In 1992, the National Adverse Drug Event Monitoring Centre created at the University of Cape Town in 1987 became the first National Pharmacovigilance Centre in Africa to become a full member of the WHO International Drug Monitoring Programme.8 In 1998, guidelines for the reporting of adverse drug reactions (ADRs) were developed for the pharmaceutical industry and have served as a reference for all persons conducting clinical trials and applicants who have statutory obligations to report safety information to the MCC. In addition, a pharmacovigilance committee was formed and continues to serve the MCC to date. The ADR system also includes the Adverse Event Following Immunization system, formalised by the Expanded Programme on Immunization (EPI) in 1997, for reporting of vaccine reactions and related safety concerns.9
Programmatic pharmacovigilance and awareness of pharmacovigilance in South Africa was boosted when the Operational Plan for Comprehensive HIV/AIDS Care was launched by Parliament in 2003 with the responsibility of implementation delegated to the MCC. The pharmacovigilance programme has experienced a high staff turnover and systems problems, and, although the MCC secretariat is responsible for ensuring the proper functioning of the key units, there is no formal relationship between the MCC and the University of Limpopo/Medunsa unit, or any system of peer review of the unit.10 As a result, many provinces have developed their own pharmacovigilance programmes and non-governmental organisations such as the President's Emergency Plan for AIDS Relief, Management Sciences for Health and Wits Health Consortium have also developed pharmacovigilance programmes that do not feed into the national system (personal communication by Dr Ushma Mehta).
Essential Drugs List and Standard Treatment Guidelines
Antibiotic management encompasses restrictions on the use of antibiotics by type and application, especially those to which resistance emerges rapidly.11 Limiting the choice of antibiotics through the use of formularies may not only reduce hospital flora to a wide spectrum of antibiotics, but can save costs to the patient, the facility and the government. The development of Essential Drugs Lists (EDLs) and Standard Treatment Guidelines (STGs) forms part of this strategy in the public sector. In the private sector, formularies are developed at the discretion of the facility management and, reportedly, there is little enforcement of their use in practice.
The STGs and EDL form part of the country's 'Essential Drugs Concept', and are viewed as critical aspects of national health policy. Compiled and periodically reviewed by expert committees under the auspices of the National Essential Drugs List Committee and implemented through the South African NDoH, these documents serve to address medicine availability and accessibility problems at primary care and hospital-level health facilities. In the case of antibiotics, they also provide standards for rational prescribing. Drugs on the EDL are generic, criterion-based and stratified by primary and hospital care, and further stratified by guidelines for adult and paediatric patients. Drugs excluded from the list may be requested in exceptional circumstances for specific patients according to a standardised process. Some drugs may be included in institution-specific supplementary EDLs formulated and periodically reviewed by the institution's Pharmacy and Therapeutics Committee (PTC).1
Resistance and antibiotic selection
Two of the most important factors influencing the inclusion of an antibiotic in the EDL should be microbial aetiology of the disease and the incidence of resistance. The latter, however, has not played a role in the development of the South African STGs or EDL. When the 'expert committees' compiled the documents, they did so without the benefit of surveillance studies or even sentinel site data. Given the high burden of bacterial infections in the public health system as a result of the HIV/AIDS epidemic, researchers recommended that surveillance data be collected and utilised to inform amendments to the present STGs.11
Traditional medicine
The low costs of traditional medicines make them a popular choice for many South Africans, with the market estimated at around R3 billion (US$492 million).7 Around 350 of the country's plants are commonly used for medicinal purposes, with 20 000 tons being consumed by at least 27 million patients annually. In 2008, the government published a draft policy on African traditional medicine with the aim of institutionalising it within the health care system. The policy sought to regulate the market through registration, intellectual property provisions, research, and formalisation of the traditional healer profession. The impact of this market on antibiotic use and resistance is unknown. One remedy, the root extract umckaloabo, has been patented by the German company ISO Arzneimittel to treat pneumonia, tuberculosis and other bacterial diseases. As an antibiotic substitute, the efficacy of this medicine is worth further exploration. However, the extent to which other traditional medicines are mixed with antibiotics and to what effect have not been investigated.12
Antibiotic supply chain
Pharmaceutical industry and manufacturers
The pharmaceutical industry in South Africa is relatively well developed and mostly focused on the production of generics, including manufacturing copy medicines under licence.7 Several multinational companies have a presence through local subsidiaries and increasingly view the country as a stable base from which to penetrate sub-Saharan Africa. The public sector tendering process is highly competitive and provides huge opportunities to bid winners.
The market is currently fragmented, with no one player holding more than 15% market share. Domestic producers meet around one-third of the country's pharmaceutical demand, with the percentage higher in the generics sector. Key foreign companies are GSK, Sanofi-Aventis, BMS and Johnson & Johnson. US companies supply over one-fifth of the market, followed by German, British and Swiss firms. In June 2010, South Africa's Minister of Trade and Industry welcomed Indian pharmaceutical companies to establish manufacturing units in the country. The invitation came as part of the government's larger industrial policy framework.
Distribution
The government maintains a cost-conscious medicine procurement policy, which is biased towards local industry and generics. The process begins with the submission of orders and expected pharmaceutical needs from hospital PTCs to the NDoH, which manages a competitive tender process among suppliers. Once a tender is awarded and fulfilled, medicines are distributed through government warehouse depots housed in each province. Primary health clinics generally order from large hospitals in their areas or from the supply depots. The majority work on an EDL and have a set protocol of antibiotics they can use for treating specific conditions. Their demand is included in the quantities the government calls for in the tender. Although varied, and presumably increasing, hospital demand should form the basis of the tender amounts. A review of tenders over the past 4 years (2007 - 2011) shows little to no change in the quantity of antibiotics requested. The reason for this is unclear.
The private sector functions differently. Three large hospital networks constitute the bulk of demand, viz. Netcare, Medi-Clinic and Life Healthcare. Each network reportedly has a formulary on which they base the types of antibiotics to order. Because private hospitals are not restricted to following formularies in the manner that public hospitals are bound to the EDL, the formulary is not necessarily followed by facilities in the pattern of antibiotics stocked. Private sector facilities can purchase medicines directly from wholesalers and pharmaceutical companies, all of which must be approved by the MCC. Three distribution companies - IHD, Kinesis and PHD - distribute the majority of originator medicines on the market (IMS background paper). These distributors handle stocking on behalf of their principals and undertake delivery to wholesalers, pharmacists, dispensing doctors, private hospitals and other private outlets.
Prescribing and dispensing
The NDP aim of developing 'human resources to promote the concepts of rational drug use' is enabled by pharmaceutical support staff appointed to ensure an optimal distribution chain. Multidisciplinary hospital PTCs are recommended in the public and private sector to ensure efficient and cost-effective medicine supply and use by compilation of a hospital formulary and good supply chain management.1 By law, only licensed practitioners may prescribe and/or dispense antibiotics. A prescription or verbal instructions of an authorised prescriber known to the managing pharmacist are necessary to purchase antibiotics from a hospital or private pharmacy, and unregulated over-the-counter sales are not the major concern of national antibiotic stewardship.
Pharmacists
The government requires that pharmacies operate under a licence and the full-time management and supervision of a registered pharmacist. In addition to playing a central community education role advising patients on the correct use of medicines, pharmacists are also expected to assume a leadership role in the rational use of medicines in both the health care and community environments. In the hospital setting, the pharmacist participates in the hospital PTC that regulates antibiotic use and is expected to communicate with antibiotic stewardship committees to determine resistance patterns in the local setting. Pharmacies also house mandatory reference sources and have access to additional information from the central drug information system.1
Two sets of ethical and professional conduct codes issued by the South African Pharmacy Council serve to guide pharmacists and hold them accountable. The standards emphasise a practice philosophy, patient respect and the pharmacist's role within a multidisciplinary team, an integral part of the role served by a clinical pharmacist.12
It is important to note that pharmacists may sell a greater or lesser quantity of antibiotics than prescribed. However, the quantity dispensed cannot be over 5% more or less than that specified in the prescription. The extent to which pharmacists and patients use this allowance when dealing in antibiotics and the impact it has on appropriate dosing are unknown.2
Medical practitioners and nurses
The Health Professions Council of South Africa and the Allied Health Professions Council of South Africa register medical practitioners to prescribe, compound, dispense and possess medicines.2 Professional Council regulations make explicit mention of the conflict between being licensed to prescribe medicines and pharmacy ownership or management. Whereas other countries allow prescribers to both practise medicine and own pharmacies, South Africa prohibits it and may thus reduce associated abuses. It is not known whether the restriction has an impact on the financial incentives of prescribers or the amount and types of antibiotics they prescribe.
Upon successful completion of a suitable training programme, nurses can apply for a licence to prescribe and dispense medicines, with prescribing at primary care level being competency-based as opposed to occupation-based. In situations where medical practitioners are not available, nurses are further permitted to diagnose patients if authorised by the provincial Director-General of Hospital Services, the medical officer of such local authority or the medical practitioner in charge of such an organisation in consultation with the South African Nursing Council.13
Education and training
The NDP prioritises the education and training of medical practitioners, nurses, pharmacists, pharmacy support staff, health service managers and pharmaceutical depot managers in the context of all relevant aspects of pharmaceutical management, commonly used STGs, the EDL and rational drug use. The availability of scientifically validated drug information for health care professionals and the community through Drug Information Centres (DICs) also aids in supporting the informed use of medicines. Relevant professional councils are tasked with oversight of mandatory continuing education and training and ensure that core curricula of all educational programmes include adequate inclusion of the concepts of rational drug use, patient counselling and communication. The pharmaceutical industry is required to provide the public with 'patient information leaflets' that describe the medicines and their proper use in common language. Facilitating drug surveillance is a further function of the DIC.1
Population-level antibioticconsumption
Pharmaceutical pricing
Pharmaceutical pricing and reimbursement is a contentious issue in South Africa.7 In the past prices were virtually uncontrolled, with the government, manufacturers, wholesalers and retailers all denying responsibility for the resulting high costs to patients. Reform through the Regulation on the Pricing of Medicines and Related Substances legislation in 2002 sought to address the problem, but implementation proved difficult. Further, controversy surrounded the 'single exit price', a flat fee system for dispensers, which replaced the mark-up system. Under the law, dispensing fees for prescription drugs were set at a maximum 26% of the manufacturer's selling price. After repeated disputes, the government revealed a new pharmacy dispensing fee system in which there are a series of mark-up percentage ceilings within medicine price brackets. Under the new structure, pharmacies charge less for low-priced, high-volume medicines like antibiotics, but can increase their fees for higher-priced products. Although it is hoped that this progressive system will increase access among low-income patients, this may be at the expense of independent, small pharmacies that are unable to sustain falling profit margins.
Antibiotic spending in the public sector and the generics market
At present, government tender documents are the only source of information on antibiotic spending and demand in the public sector. However, the information has yet to be evaluated or assessed and is therefore not available for this report.
Generics
Pharmacists are required to inform patients if a generic version of a medicine is available and are bound by law to dispense the generic. Exceptions are made only if the patient expressly refuses the generic or if the prescribing doctor has forbidden the generic in a note on the script. Substitution can also be overruled if the generic costs more than the originator or if the government declared the generic non-suitable.12
Medicines remain a key contributor to rising health care costs.14 However, encouraging growth in the use of generic medicines could result in significant cost savings. Originators still account for 59% of the pharmaceutical market in terms of value sales, but generic medicines dominate the market in terms of sales volume.7 By 2014, the pharmaceutical industry predicts that the generics market will have grown by 13.3% in local currency terms. Generic efficiency, or the number of times a generic could be dispensed, also increased from 69% in 2007 to 72% in 2009.14 The reasons for this growth include but are not limited to more generic alternatives being made available on the market, and their encouraged use by medical schemes and the government.
Antibiotic spending in the private sector
Information on antibiotic consumption in the private sector comes primarily from IMS Health. Data are collected from wholesalers as well as from direct sales from manufacturers to pharmacies.
Annual medicine expenditure can be broken into two components - cost and volume. Table I shows antibiotic consumption in terms of units. Although IMS does not report in the commonly accepted unit for pharmaceutical consumption, daily defined doses, their units do help to show trends over time. In the case of South Africa, the trend is an increasing one. In particular, unit sales of broadspectrum penicillins, fluoroquinolones, carbapenems and penems, carbacephems and glycopeptides have increased annually. Use of chloramphenicols has decreased, while cephalosporins, trimethoprim combinations, aminoglycosides and monobactams have fluctuated.15
From a value perspective, the top three classes of antibiotics used in the private sector are oral broad-spectrum penicillin with 18.3% of the market, penems and carbapenems with 14% of the market, and macrolides with 11.1% of the market. While penicillins and macrolides both exhibited growth rates over 6% from 2009, use of penems and carbapenems grew by 18.6%.15 The value, growth and market share for antibiotic classes are shown in Table II.
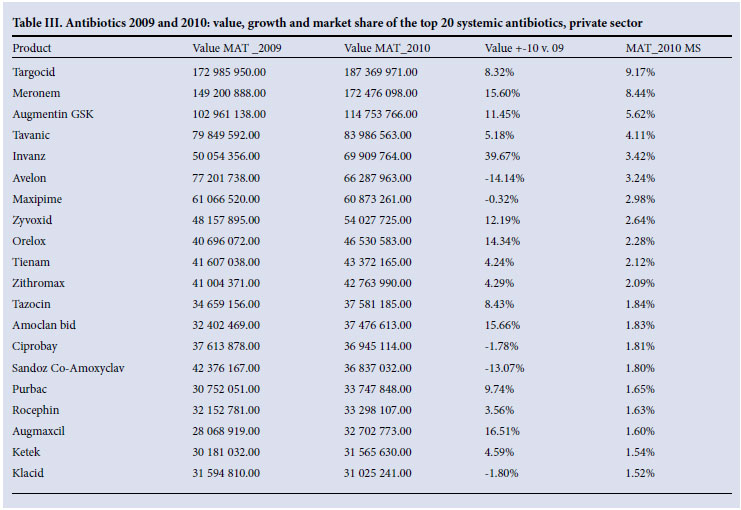
The top 20 antibiotics contribute 61% towards the total systemic antibacterial market. Targocid is ranked first with a 9.2% market share and growth rate of 8.3% from the previous year. Meropenem, ranked second, has a market share of 8.4% and growth of 15.6%, and Augmentin GSK is ranked third with 5.6% of market share and growth of 11.5%.15 The value, growth and market share of the top 20 antibiotic agents are shown in Table III.
References
1. Department of Health. National Drug Policy for South Africa. Pretoria: Government Printer, 1996. http://www.doh.gov.za/docs/policy/drugsjan1996.pdf [ Links ]
2. Department of Health. Medicine and Related Substances Control Act. Pretoria: Government Printer, 1997. http://www.doh.gov.za/docs/legislation/acts/1997/act90.pdf [ Links ]
3. Medicines Control Council. Registration of Medicines. Pharmaceutical and Analytical. http://www.mccza.com [ Links ]
4. Medicines Control Council. Registration of Medicines. Stability. http://www.mccza.com [ Links ]
5. Medicines Control Council. Registration of Medicines. Biostudies. http://www.mccza.com [ Links ]
6. Medicines Control Council. http://www.mccza.com/genericDocuments/20.10_Licences_issued_Dec10_v1.doc (accessed 15 March 2011). [ Links ]
7. South Africa Pharmaceuticals & Healthcare Report. London: Business Monitor International, 2010. [ Links ]
8. Health Professions Act 56 of 1974. http://www.hpcsa.co.za/downloads/health_act/health_act_56_1974.pdf [ Links ]
9. Allied Health Professions Act 63 of 1982. http://www.ahpcsa.co.za/pdf_files/legislation/the-act/The%20Allied%20Health%20Professions%20Act%2063%20of%201982%20_as%20amended.pdf [ Links ]
10. World Health Organization. Training Resources. http://apps.who.int/prequal/trainingresources/pq_pres/pharmacovigilance/CountryARVs/South_Africa.ppt - 273 [ Links ]
11. Essack SY. Strategies for the prevention and containment of antibiotic resistance. South African Family Practice 2006;48(1). [ Links ]
12. South African Pharmacy Council (SAPC). Good Pharmacy Practice in South Africa. 4th ed. Arcadia: South African Pharmacy Council, 2010. [ Links ]
13. Nursing Act 33 of 2005. http://www.acts.co.za/nursing_act_2005/index.htm [ Links ]
14. Bester M, Badenhorst E. Medicines Review. Mediscor PBM, 2010. [ Links ]
15. IMS Health South Africa: Total Private Market Report - MAT January 2011. [ Links ]


{kind=link}
{kind=link}
{kind=link}