










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.8 Pretoria ago. 2011
ORIGINAL ARTICLES
Reference intervals for serum total cholesterol, HDL cholesterol and non-HDL cholesterol in Batswana adults
Seako M MaphephuI; Ishmael KasvosveII
IBSc. Department of Medical Laboratory Sciences, Faculty of Medicine and Health Sciences, University of Botswana, Gaborone, Botswana
IIBSc, MSc, PhD. Department of Medical Laboratory Sciences, Faculty of Medicine and Health Sciences, University of Botswana, Gaborone, Botswana. International Training and Education Center for Health (I-TECH) Botswana, Gaborone
ABSTRACT
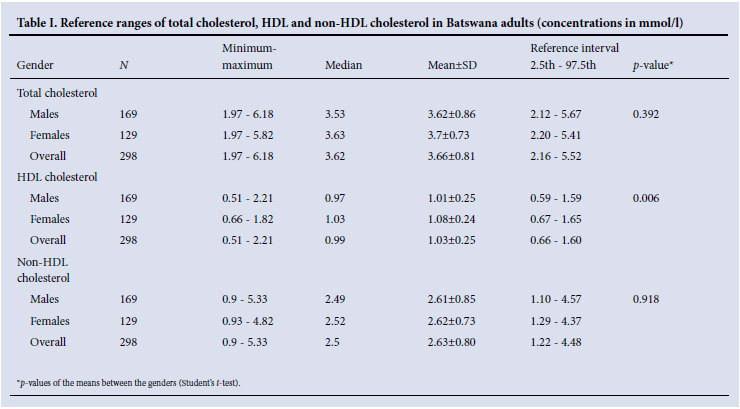
Reference intervals of total cholesterol, HDL cholesterol and non- HDL cholesterol concentrations were determined on 309 blood donors from an urban and peri-urban population of Botswana. Using non-parametric methods to establish 2.5th and 97.5th percentiles of the distribution, the intervals were: total cholesterol 2.16 - 5.52 mmol/l; non-HDL cholesterol 1.22 - 4.48 mmol/l; and HDL cholesterol 0.67 - 1.65 mmol/l and 0.59 - 1.59 mmol/l for females and males, respectively.
Population-specific reference intervals when combined with other clinical data are important for clinical decision-making in the management of patients considered to be at risk for atherosclerotic cardiovascular disease (CVD). Reference intervals vary according to gender, age, ethnicity and diet, among other factors; it is therefore recommended that population-specific reference intervals be established. The ISO 15189:2003 standard recommends that biological reference intervals appropriate for the reference population and patient population be used when reporting laboratory results.1 Southern Africa has little study of populations that are undergoing significant change in lifestyle and risk of CVD. To our knowledge, there are no published reference ranges for clinical chemistry parameters for the Batswana adult population, and the common practice is to adopt reference intervals from other populations. We aimed to establish reference intervals for serum total cholesterol, HDL cholesterol and non-HDL cholesterol concentrations in Batswana adults.
Materials and methods
The National Blood Transfusion Services (NBTS) centre in Gaborone is the main blood bank laboratory in Botswana, collecting about 23 000 blood units annually. A professional health counsellor carries out a pre-donation confidential assessment to determine eligibility to donate blood and prior history of diseases, medications, sexual behaviour, cigarette smoking, alcohol consumption and illicit drugs. We analysed 309 anonymised residual blood samples (129 females) from qualifying donors who were from Gaborone and surrounding areas, representing the urban and peri-urban indigenous populations of Botswana. All the blood collected was tested for presence of HIV and hepatitis A, B and C viruses, and screened for sexually transmitted infections. Ethical approval for the study was obtained from the institutional review boards of the University of Botswana, NBTS and Ministry of Health. Anonymised residual samples were used, and therefore no consent was obtained from donors, consistent with ISO:15189 recommendations that state that the use of samples for purposes other than requested without prior consent should only occur if the residual samples are rendered anonymous.2
Blood collected in plain tubes was transported chilled in a cooler box from NBTS to a central testing laboratory where it was centrifuged using a Haereus Instruments Biofuge primo centrifuge at 3 000 rpm for 5 minutes. Serum was separated and stored at -20ºC until analysis. The samples were tested using Roche reagent kits for total cholesterol and HDL cholesterol on a COBAS Integra 400 plus auto-analyser using enzymatic methods according to standard operating procedures. The analyser was calibrated using Roche calibrators, and quality control sera from the manufacturer were tested alongside the serum samples. Non-HDL cholesterol was obtained by subtracting HDL cholesterol from total cholesterol.3 The reference interval was calculated as the range between the 2.5th and 97.5th percentile values of the population using Stata/SE version 8.2 statistical software (StataCorp, Texas). Comparison between females and males was done using Student's t-test.
Results
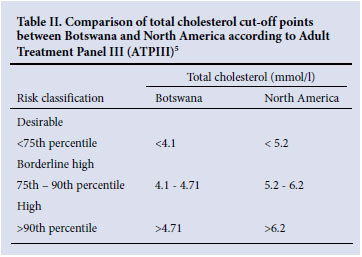
Reference intervals for total cholesterol, HDL cholesterol and non-HDL cholesterol were constructed on 129 females and 169 males aged 16 - 60 years; 11 had incomplete demographic data and were excluded. The Clinical Laboratory Standards Institute recommends that a minimum of 120 acceptable observations from healthy individuals be used to calculate reference intervals using non-parametric methods.4 Overall, the reference intervals for total cholesterol were 2.16 -5.52 mmol/l and for non-HDL cholesterol 1.22 - 4.48 mmol/l (see Table I). Reference intervals for HDL cholesterol concentration were 0.67 - 1.65 mmol/l and 0.59 - 1.59 mmol/l for females and males, respectively. Table II compares the cut-off values of total cholesterol concentration between Batswana and North American populations according to recommendations of the Laboratory Standardization Panel of the National Cholesterol Education Program.5
Discussion
To our knowledge, this is the first study to document reference intervals for the black population of Botswana, a middle-income country. The 2.5th and 97.5th percentiles were used as limits for the reference intervals. In keeping with other studies, HDL cholesterol concentrations were higher in females than males (p=0.006). The reference interval for total cholesterol derived in this study was lower than those from other African populations and industrialised countries.6
In combination with other predisposing factors, HDL cholesterol concentration is useful in assessing the risk of developing coronary heart disease (CHD). Low levels of HDL cholesterol are associated with increased risk of developing CHD whereas a high concentration is protective against CHD. Non-HDL cholesterol correlates with mortality owing to CHD.7 To screen subjects at risk of developing CHD by using lipid concentrations, population-specific reference values should be applied. Table II shows that the total cholesterol concentration thresholds for CHD risk stratification are lower in the studied population, compared with North America.
The samples in this study were from non-fasting donors. Previous studies recommend that lipid concentration estimations should be done on fasting specimens. However, recent literature suggests that fasting is not necessary for lipid concentration estimation and does not influence the results.4 In this study, we recognise that health status of the population was not determined by a physician; however, blood donors are considered a good source of reference individuals. Our findings, based on a limited sample size, suggest that reference intervals of lipids are lower in Batswana than other populations. As developing countries are expected to have CVD as the leading cause of death by 2020, a larger study in Botswana and possibly other regions of Africa to correlate vascular disease with the concentrations of the conventional lipid profile should be carried out.
We thank the management and staff of the National Blood Transfusion Services Botswana for screening of blood donors and collection of blood samples, and the Department of Chemical Pathology, Princess Marina Hospital, Gaborone, for use of the chemistry auto-analyser and other equipment.
References
1. International Organization for Standardisation. Medical laboratories - particular requirements for quality and competency. ISO 15189. Geneva: ISO, 2003. [ Links ]
2. International Organization for Standardisation. Annexure C: Ethics in laboratory medicine. ISO 15189: 2007:C9. Geneva: ISO, 2007. [ Links ]
3. Emerging Risk Factors Collaboration, Di Angelantonio E, Sarwar N, et al. Major lipids, apolipoproteins and risk factors of vascular disease. JAMA 2009;302:1993-2000. [ Links ]
4. National Committee for Clinical Laboratory Standards. How to define and determine reference intervals in the clinical laboratory; approved guideline. NCCLS document C28-A and C28-A2. Wayne, PA: NCCLS, 1995,2001. [ Links ]
5. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497. [ Links ]
6. Roberts WL, McMillin GA, Burtis CA. Reference Information for Clinical Laboratory. In: Burtis CA, Ashwood ER, Bruns DE, eds. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics. St Louis: Elsevier Saunders, 2006:2251-2318. [ Links ]
7. Cui Y, Blumenthal RS, Flaws JA, et al. Non-high density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Arch Intern Med 2001;161:1413-1419. [ Links ]
Accepted 8 March 2011.
Corresponding author: I Kasvosve (ishmael.kasvosve@mopipi.ub.bw)


{kind=link}