










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.7 Pretoria jul. 2011
ORIGINAL ARTICLES
The prevalence of hepatitis B infection in a rural South African HIV clinic
Tom H BoylesI; Karen CohenII
IBM BCh, MRCP (UK), DTM&H (UK), MD (UK). Madwaleni Hospital, Eastern Cape, and Division of Infectious Diseases and HIV Medicine, Department of Medicine, University of Cape Town
IIMB ChB, FCFP (SA), MSc (Epid), Dip HIV Man (SA), Dip Obst (SA). Division of Clinical Pharmacology, Department of Medicine, University of Cape Town
ABSTRACT
The prevalence of hepatitis B virus (HBV) infection in 1 765 HIVpositive patients in rural Eastern Cape was 7.1%. This is lower than the previously reported rural prevalence and is similar to urban prevalence. Male sex and baseline alanine aminotransferase (ALT) were significant predictors of HBV status. Most HBV-positive patients had normal baseline ALT, making ALT an insensitive screening test for HBV status.
Since both HIV and HBV are endemic in sub-Saharan Africa and share routes of transmission, co-infection is common.1 As life expectancy with HIV has improved owing to widespread use of antiretroviral treatment (ART), the proportion of morbidity and mortality caused by non-AIDS-defining illnesses such as HBV is likely to increase.
Estimates of the prevalence of HBV infection among adults with HIV in South Africa have been around 5% in urban cohorts2,3 and 20% in a cohort of goldminers from rural areas.1 It has therefore been suggested that co-infection rates are higher in rural than in urban areas in South Africa.4 We present prevalence data from a cohort of HIV-infected adults in rural Eastern Cape.
Methods
Madwaleni HIV Wellness and ART Programme is a public sector service in a deeply rural area of the Eastern Cape. ART delivery began in June 2005 and, by October 2009, about 4 000 adult patients had registered on the programme. About 2 000 patients had initiated ART; the remainder were not yet eligible for ART. Patient demographic and clinical data, including laboratory investigations, were prospectively entered into a database.
We sought to identify HBV co-infected patients so that we could motivate for them to receive tenofovir. All patients either established on ART or undergoing CD4 monitoring while not yet eligible for ART required 6-monthly routine blood tests. Over a 10-month period, testing for hepatitis B surface antigen (HBVsAg) was added as an additional test on all routine blood tests. Samples were processed within 48 hours by AxSYM HBsAg (V2) (Abbott Laboratories, Abbott Park, Illinois, USA).
Demographic details, HBVsAg results, ALT and CD4 count at the time of registration on the programme were extracted from the database. Statistical analysis was performed using STATA version 10 (Stata Corp. College Station, TX). CD4 count and age were summarised using median and interquartile range as they were nonnormally distributed. ALT was categorised as either above or below the upper limit of the normal range at the programme laboratory (40 IU/l). A multivariate logistic regression model was constructed, using a stepwise forward fitting approach, adding first variables that appeared to be most strongly associated with HBVsAg status on univariate analysis. Age was included in the model based on an a priori decision.
Ethical approval was obtained from the University of Cape Town's Faculty of Health Sciences Research Ethics Committee.
Results
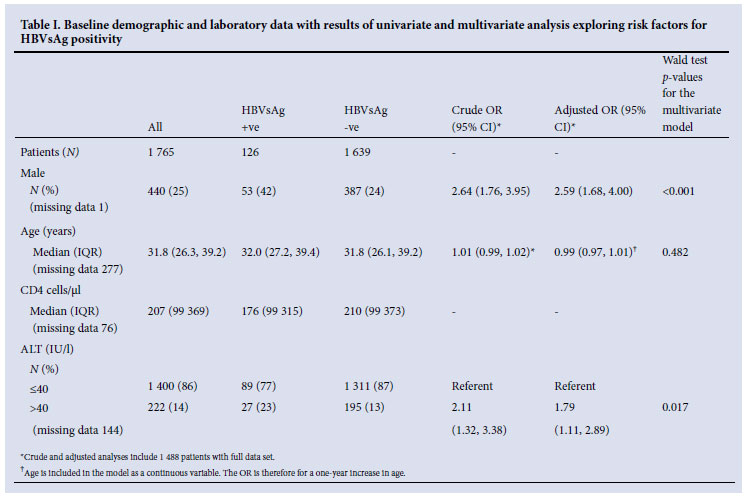
Between December 2008 and October 2009, 1 765 adult patients were tested for HBVsAg, of whom126 were positive, giving an overall prevalence of 7.1%. The prevalence was 5.5% in females and 12.1% in males (chi-squared p<0.001). One thousand, one hundred and sixtynine (66%) had already commenced ART, and HBVsAg prevalence was similar in those on and off ART (6.6% v. 8.2%, chi-squared p=0.207). Patient HBVsAg status, demographic and laboratory variables and results of analysis are summarised in Table I.
On univariate analysis, ALT at baseline was associated with HBVsAg positivity (odds ratio (OR) 2.11, 95% confidence interval (CI) 1.32 - 3.38). After adjustment, the association remained but was weaker (OR 1.79, 95% CI 1.11 - 2.89, p=0.017), possibly because sex and ALT were strongly associated, with 21% of men and 11% of women having ALT>40 IU/l (chi-squared p<0.001). At baseline, 89/116 (77%) of HBVsAg-positive patients had normal ALT.
After adjustment for age and baseline ALT, male sex remained strongly associated with HBVsAg positivity (OR 2.59, CI 1.68 - 4.00, p<0.001). Age was not associated with HBVsAg positivity.
Discussion
In this Eastern Cape cohort, the prevalence of HBV-HIV co-infection was 7.1%. This figure is lower than the 20% prevalence previously estimated in rural South Africa,1 but is similar to the estimated prevalence in urban cohorts.2,3 Male sex and abnormal baseline ALT were independent predictors of HBVsAg positivity in our cohort.
Previous estimates of rural co-infection rates may not be applicable to the rural population of South Africa as a whole. A study of goldminers in South Africa found a prevalence of 20%, but participants were drawn from a number of African countries, and 94% were male.1
Male sex is a risk factor for HBV positivity in HIV-negative South Africans5 and is thought to be the result of either the observed prolonged replicative phase of the virus in boys or differences in the sexual behaviours of men and women.5,6 Our data are the first to suggest that male sex is also a risk factor for HBV positivity in HIVpositive South Africans; further study is warranted to determine if the reasons for this correlation are similar to those in the HIV-negative population.
Studies have found ALT to be an unreliable marker of HBV status in HIV-positive adults, possibly because of the high prevalence of other factors that affect ALT, including opportunistic infections and drugs.1,3 We found an association between baseline ALT and HBV status in multivariate analysis. However, 77% of HBV-positive patients had a normal baseline ALT, so it is not a sensitive marker for HBVsAg positivity. Studies have shown that abnormal baseline ALT predicts high HBV viral load and risk of toxicity on ART.1 Baseline ALT may therefore be more useful as an addition to HBV testing than as a predictor of HBV status.
A limitation of this study is that HBVsAg was the only available measure of chronic HBV infection. A previous study has shown that detectable HBV viral load with negative HBVsAg (known as occult HBV infection) may account for two-thirds of all HBV infections, although the clinical implications of this are not well known.7 Patients were selected for the study by attending for routine blood tests, which might have biased the sample towards patients established on ART. However, the prevalence of HBV was similar among those on and off ART, suggesting that no important bias was introduced. Lamivudine is known to increase the rate of HBVsAg loss. Therefore, some patients on lamivudine might have cleared HBVsAg before testing.
We explored the association between ALT measured on entry into the treatment programme and a positive test for HBVsAg, as many patients had commenced an ART regimen containing lamivudine at the time of HBV testing. The maximum time from baseline measurement to HBV testing was 4 years. An important assumption is therefore that few HBV transmissions occurred in that time; this is reasonable, given the relatively short time period and that many HBV transmissions in South Africa are thought to occur in childhood.6
References
1. Hoffmann CJ, Charalambous S, Martin DJ, et al. Hepatitis B virus infection and response to antiretroviral therapy (ART) in a South African ART program. Clin Infect Dis 2008; 47(11):1479-1485. [ Links ]
2. Lodenyo H, Schoub B, Ally R, Kairu S, Segal I. Hepatitis B and C virus infections and liver function in AIDS patients at Chris Hani Baragwanath Hospital, Johannesburg. East Afr Med J 2000;77(1):13-15. [ Links ]
3. Firnhaber C, Reyneke A, Schulze D, et al. The prevalence of hepatitis B co-infection in a South African urban government HIV clinic. S Afr Med J 2008;98(7):541-544. [ Links ]
4. Di Bisceglie AM, Maskew M, Schulze D, Reyneke A, McNamara L, Firnhaber C. HIV-HBV coinfection among South African patients receiving antiretroviral therapy. Antivir Ther 2010;15(3 Pt B):499-503. [ Links ]
5. Abdool Karim SS, Thejpal R, Coovadia HM. Household clustering and intra-household transmission patterns of hepatitis B virus infection in South Africa. Int J Epidemiol 1991;20(2):495-503. [ Links ]
6. Kramvis A, Kew MC. Epidemiology of hepatitis B virus in Africa, its genotypes and clinical associations of genotypes. Hepatol Res 2007;37(s1):S9-S19. [ Links ]
7. Firnhaber C, Viana R, Reyneke A, et al. Occult hepatitis B virus infection in patients with isolated core antibody and HIV co-infection in an urban clinic in Johannesburg, South Africa. Int J Infect Dis 2009;13(4):488-492. [ Links ]
Accepted 14 February 2011.
Corresponding author: T Boyles (tomboyles@yahoo.com)


{kind=link}