










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.7 Pretoria jul. 2011
ORIGINAL ARTICLES
Pathogenic lower genital tract organisms in HIV-infected and uninfected women, and their association with postpartum infectious morbidity
H M SebitloaneI; J MoodleyII; T M EsterhuizenIII
IMB ChB, FCOG, MMed. Department of Obstetrics and Gynaecology, University of KwaZulu-Natal, Durban
IIMB ChB, FCOG (SA), FRCOG (UK), MD. Women's Health and HIV Research Group, University of KwaZulu-Natal
IIIMSc. School of Public Health, University of KwaZulu-Natal
ABSTRACT
OBJECTIVES: To determine the prevalence of vaginal pathogens during pregnancy and their impact on postpartum infectious morbidity among antiretroviral-naïve HIV-infected, and HIVuninfected, women.
METHODS: Vaginal swabs were obtained during early labour by speculum examination prior to digital vaginal examination, and sent for microscopy and culture. Women were assessed for infectious complications within 24 - 72 hours of delivery, and up to 2 weeks postpartum.
RESULTS: Laboratory results were available for 801 women who delivered vaginally (418 HIV infected and 383 uninfected). The baseline characteristics of the two groups were comparable, and the median CD4 count for HIV-infected women (N=391) was 416/µl. Fifty-five per cent (54.8%) of women had positive cultures (439/801), more among those who were HIV infected than uninfected (60% v. 49.1%, p=0.002). Women with positive cultures had slightly higher rates of infectious morbidity than those without (20.5% v. 15.2%, p=0.052). Trichomonas vaginalis and group B streptococci were significantly associated with sepsis (p=0.023 and <0.001, respectively), whereas the presence of Candida species seemed to be protective (relative risk 0.69, p=0.014).
CONCLUSION: The study shows that a high proportion of pregnant women have pathogenic organisms in the lower genital tract that are associated with development of postpartum infectious morbidity.
A balanced colonisation by endogenous vaginal microflora of the lower female genital tract consists of predominantly Lactobacillus species,1 co-existing with vaginal anaerobes and aerobes such as Streptococcus agalactiae (e.g. group B streptococci)2 and the Bacteroides family.3 Disturbing this microbial milieu results in overgrowth of bacterial vaginosis-related organisms which are associated with a 3 - 6 times greater risk of postpartum endometritis.4,5 However, the role of endogenous lower genital tract pathogens, especially bacterial vaginosis organisms, and their impact on postpartum infectious morbidity, is controversial.6,7 Other vaginal organisms associated with postpartum infectious morbidity include Ureaplasma urealyticum, group B streptococcus (GBS) and other sexually transmitted infections (STIs) such as Trichomonas vaginalis, Neisseria gonorrhoeae and Chlamydia trachomatis. Case detection and treatment of the latter STIs is often technically difficult and expensive. Furthermore, the prevalence of genital tract infections is probably higher among HIV-positive women because of their associated immunosuppression. Studies have shown perturbations in the vaginal flora of HIV-infected women, with approximately 20% of HIV-infected women having Lactobacillus-dominant vaginal flora.8,9 Cu-Uvin et al. found no difference in the prevalence rates of lower genital tract infections among HIV-infected women compared with HIV-uninfected women.10 These conflicting findings led us to determine the prevalence of lower genital tract infections during pregnancy and their impact on postpartum infectious morbidity among HIV-infected and uninfected women.
Methods
Study population
Our study was nested within a prospective trial of 1 404 women (716 HIV positive compared with 688 HIV negative) over a 2-year period.11,12 Women of 18 years and older, and who were at 36 weeks' gestation and greater, in whom vaginal delivery was anticipated, were enrolled after obtaining consent. In addition to standard antenatal tests, pre- and post-test HIV counselling and HIV rapid testing were offered to all the women. CD4 lymphocyte counts were performed in the HIV-infected women. Vaginal swab specimens were obtained during early labour by speculum examination prior to digital vaginal examination. Since the parent study involved randomising HIVinfected women to receive either a stat dose of cefoxitin or placebo, the specimens were taken before the administration of the study drug. The vaginal swab specimens were rolled onto a glass slide for the determination of a bacterial vaginosis (BV) score using Nugent's criteria,13 and then transported in Ames medium (for detection of Gram-negative and positive organisms) and Diamond's medium (for detection of trichomoniasis). In the laboratory, the swabs were also inoculated on cefoxitin CLED plates, bacitracin choc plate and laked blood cefoxitin, for the detection of any significant isolates, and an AMS plate was inoculated to detect the presence of any antimicrobial substances. Significant isolates were identified, and susceptibilities were determined. Screening tests for syphilis (rapid plasma reagin) were also performed, and presence or absence of vulvo-vaginal warts was noted during speculum examination. Swab specimens for N. gonorrhoeae and Chlamydia species were not taken.
Demographic details and obstetric information were obtained, including: the number of vaginal examinations before and after the rupture of membranes, duration of ruptured membranes, and mode of delivery. All deliveries were conducted by professional midwives or doctors. Women were assessed for infectious complications within 24 -72 hours of delivery, at 1 week (range 6 -10 days), 2 weeks (range 11 - 17 days) and 6 weeks (40 - 49 days) postpartum. Infection occurring at any time point up to 2 weeks was recorded as a positive result. Only participants who had all microbiological laboratory results available were analysed.
Statistical analysis
Data were captured on Epi-Info 6 and imported for analyses into SPSS version 15.0 (SPSS Inc., Chicago, Ill.). A p-value <0.05 was considered statistically significant. Pearson's chi-square analysis was used to compare categorical variables between groups. Quantitative variables were compared between treatment groups using independent t-tests or non-parametric Mann-Whitney tests as appropriate. Generalised linear models estimated crude and adjusted relative risks. The dependent variable was modelled as binary with a log link to estimate relative risks. For multivariable analysis, the independent variables were chosen as those which were statistically significant at the 90% level of confidence on crude analysis. They were entered as main effects. Relative risks (RR) and 95% confidence intervals (CI) were reported. Since HIV status and mode of delivery were possible confounders, these were entered into the model, and adjusted relative risks were calculated.
Results
Laboratory results were available for 801 (418 HIV infected and 383 uninfected) of the 885 who had vaginal deliveries (including episiotomy and assisted deliveries). Baseline characteristics of the two groups were comparable, with no statistical differences in mean age, parity and body weight. The median CD4 count for HIV-infected women (N=391) was 416/µl (range 24 - 1 393), with 49/391 (12.5%) having CD counts <200/µl.
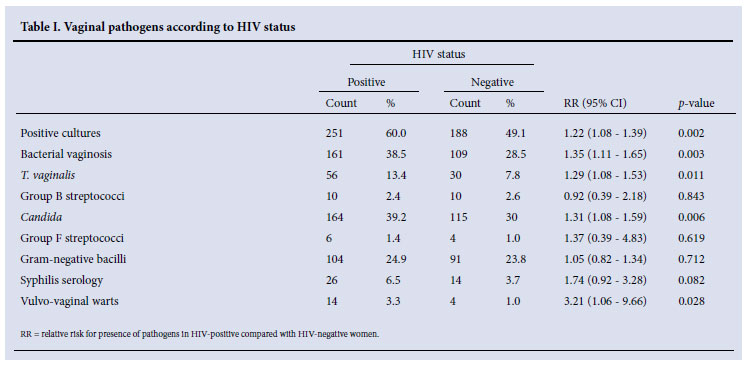
Overall, 439/801 (54.8%) had positive cultures, which was significantly more among HIV-infected women (251/418 (60%)) than HIV uninfected (188/383 (49.1%), p=0.002). T. vaginalis, BV and Candida species were significantly more prevalent among HIVinfected than uninfected women, as was vulvo-vaginal warts (Table I). Of these organisms, only T. vaginalis was significantly associated with presence of vaginal discharge on enquiry (p<0.001) (the p-value was 0.391 for BV and 0.080 for Candida species). Other organisms that were cultured included streptococci (groups B and F), as well as Gram-negative bacilli, none of which was significantly different among the HIV-infected and uninfected groups. Syphilis serology reactivity was also slightly more among HIV-infected women than among those who were uninfected (p=0.082).
Association between vaginal organisms and development of postpartum infectious complications
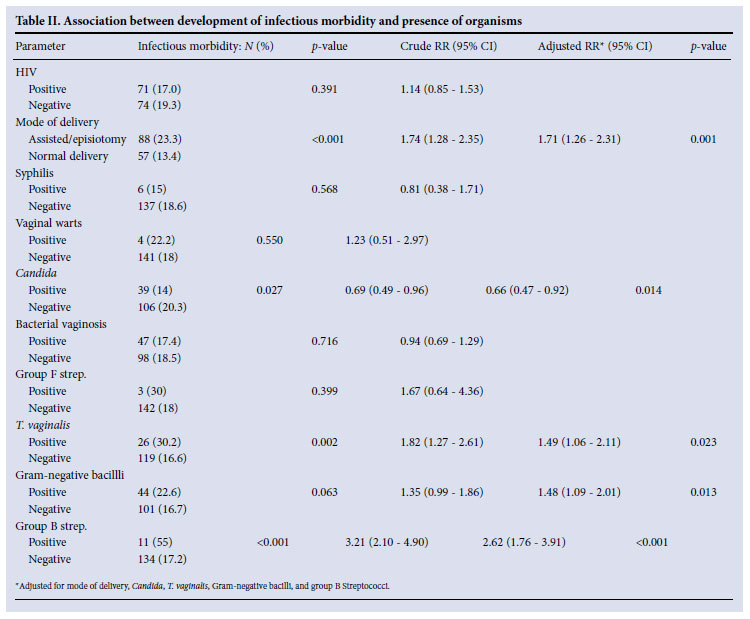
The overall puerperal sepsis rate in this cohort was 18.1% (145/801) over the 2 weeks of follow-up. Women with positive cultures had higher rates of infectious morbidity than those without (90/439 (20.5%) v. 55/362 (15.2%), p=0.052).
HIV status was not associated with development of sepsis (p=0.391) in crude or multivariable analysis and was therefore omitted from the multivariable model. Mode of delivery, Candida, T. vaginalis, Gram-negative bacilli and group B streptococci were added to the multivariable model as independent variables. After adjustment for confounding effects, assisted vaginal delivery or episiotomy posed a significantly higher risk for sepsis than non-assisted normal vaginal delivery (NVD) (p=0.001). The presence of Candida species seemed to be protective (RR 0.66, 95% CI 0.47 - 0.92) (Table II), while T. vaginalis, Gram-negative bacilli and group B streptococci were all significant risk factors for sepsis.
Discussion
In this cohort, more than 50% of women had culture-positive pathogenic organisms detected during early labour, which represents a very high rate of microbial pathogens in the lower genital tract of pregnant women who were asymptomatic, with the exception of a possible vaginal discharge. However, similar rates have been reported.14,15 In a similar population, one or more STIs was found to be present in 16.5% of asymptomatic antenatal patients.15 Though not statistically significant, postpartum infectious morbidity was higher in women with positive cultures (p=0.052). Furthermore, in our study, positive cultures were significantly higher among HIV-infected (60%) than HIV-uninfected women (49.1%, p=0.002). The difference according to HIV status was expected and is in keeping with other reports of increased rates of lower genital tract pathogens among HIV-infected women.16
A higher incidence of infectious morbidity among HIV-infected women was expected in view of their higher rate of positive cultures. The lack of influence of HIV status on the development of postpartum infectious morbidity in our study has also been noted in other reports;11,12 this is probably because most HIV-infected women in our study were immunocompetent, with mean CD4 counts >350.
The most common organisms detected in our study were associated with BV, with rates in keeping with other sub-Saharan Africa rates of up to 50%.8,17,18 Although organisms associated with BV were the most prevalent, there was surprisingly no association between presence of BV and postpartum infectious morbidity. The vast literature showing an association of BV with pregnancy complications has mainly focused on preterm labour and delivery, and subsequently postpartum endometritis.19 We postulate that the postpartum endometritis in those studies is a continuation of the preceding inflammatory process that led to miscarriage or preterm labour, and asymptomatic women who proceed to term are less likely to experience BV-associated complications in the postpartum period. This observation could explain the lack of association between the presence of BV and postpartum infectious morbidity in our cohort of otherwise asymptomatic women, recruited at > 36 weeks' gestation.
We showed a significant association of postpartum infectious morbidity and presence of T. vaginalis. This organism colonises the lower genital tract, and is therefore not expected to be associated with upper genital disease (above the level of the internal cervical os). T. vaginalis has been documented in the upper genitalia and is associated with pelvic inflammatory disease in those who are HIV infected,20 but not among those without HIV infection. Although small numbers were T. vaginalis positive, our study also found a significant association between T. vaginalis and postpartum infections in the whole cohort (p=0.010), and particularly among HIV-infected women (relative risk (RR) 3.36, p=0.009) rather than HIV-uninfected women (RR 1.29, p=0.599). This association between HIV and T. vaginalis-associated morbidity may suggest an altered host-microbe relationship, resulting in an apparent increased risk of upper genital tract infection.20 Since the parent study involved randomising HIVinfected women to a single dose of 2 grams of cefoxitin and placebo, cefoxitin administration was found to significantly reduce the development of infectious morbidity in women who had T. vaginalis (RR 0.18, 95% confidence interval 0.03 - 1.22, p=0.024). Cefoxitin has little effect on anaerobes such as T. vaginalis, and it therefore raises the possibility that its effect is more on the 'secondary invaders' that cause infection in mucosa that is already compromised by the presence of T. vaginalis. This relationship is well known in the development of pelvic inflammatory disease in non-pregnant women.21
As expected, the presence of GBS was strongly associated with development of postpartum infections. However, the prevalence rate of GBS in our study was much lower than the 15% prevalence rate reported previously from the same institution.22 This may be due to swabs only being taken from the cervico-vaginal area in this study, whereas Naidoo et al. noted that a combination of vaginal and introital swabs increased the yield for GBS by 25%.22
Candida species were present in at least 30% of our cohort; however, most women were asymptomatic. A surprising finding in our study was that the presence of Candida organisms protected against the development of postpartum infectious morbidity, which persisted even after controlling for other variables. Further studies are needed to confirm this.
In conclusion, HIV-positive women did not have an increased risk of postpartum infectious morbidity despite higher rates of pathogens in the lower genital tract, a finding which may be due to the reasonably intact immune system of the study cohort. However, the presence of T. vaginalis, Gram-negative bacilli and group B streptococci was associated with a significantly increased risk of postpartum morbidity, irrespective of HIV status.
References
1. Witkin SS, Linhares IM, Giraldo P. Bacterial flora of the female genital tract: function and immune regulation. Best Pract Res Clin Obstet Gynaecol 2007;21(3):347-354. [ Links ]
2. Thadepalli H, Chan WH, Maidman JE, Davidson EC Jr. Microflora of the cervix during normal labor and the puerperium. J Infect Dis 1978;137(5):568-572. [ Links ]
3. Goplerud CP, Ohm MJ, Galask RP. Aerobic and anaerobic flora of the cervix during pregnancy and the puerperium. Am J Obstet Gynecol 1976;26(7);858-868. [ Links ]
4. Jacobsson B, Pernevi P, Chidekel L, Platz-Christensen JJ. Bacterial vaginosis in early pregnancy may predispose for preterm birth and postpartum endometritis. Acta Obstet Gynecol Scand 2002;81:1006-1010. [ Links ]
5. Watts DH, Krohn MA, Hillier SL, Eschenbach DA. Bacterial vaginosis as a risk factor for post-cesarean endometritis. Obstet Gynecol 1990;75:52-58. [ Links ]
6. Piper JM, Newton ER, Peairs WA. Is bacterial vaginosis associated with postpartum infectious morbidity? Abstract 156, 15th Annual Meeting of the Society of Perinatal Obstetricians. Am J Obstet Gynecol 1995;172(1):304. [ Links ]
7. Faro S. Postpartum endometritis. Clin Perinatol 2005;32:803-814. [ Links ]
8. Gray RH, Waiver MJ, Sewankomb N, Serwadda D. HIV-1 infection associated with abnormal vaginal flora morphology and bacterial vaginosis. Lancet 1997;350:1780. [ Links ]
9. Martin HL, Richardson BA, Nyange PM, et al. Vaginal lactobacilli, microbial flora, and risk of human immunodeficiency virus type 1 and sexually transmitted disease acquisition. J Infect Dis 1999;180(6):1863-1868. [ Links ]
10. Cu-Uvin S, Hogan JW, Warren D, et al. Prevalence of lower genital tract infections among human immunodeficiency virus (HIV)-seropositive and high risk HIV-seronegative women. HIV Epidemiology Research Study Group. Clin Infect Dis 1999;29(5):1145-1150. [ Links ]
11. Sebitloane HM, Moodley J, Esterhuizen TM. Prophylactic antibiotics for the prevention of postpartum infectious morbidity in women infected with human immunodeficiency virus: A randomized controlled trial. Am J Obstet Gynecol 2008;198:189e1-189e6. [ Links ]
12. Sebitloane HM, Moodley J, Esterhuizen TM. Determinants of postpartum infectious complications among HIV uninfected and antiretroviral-naïve HIV infected women following vaginal delivery: a prospective cohort study. Eur J Obstet Gynecol Reprod Biol 2009;145(2):158-162. [ Links ]
13. Nugent RP, Krohn MA, Hillier SL. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of Gram's stain interpretation. J Clin Microbiol 1991;29(2):297-301. [ Links ]
14. Akerele J, Abhulimen P, Okonofua F. Prevalence of asymptomatic genital infection among pregnant women in Benin City, Nigeria. Afr J Reprod Health 2002;6(3):93-97. [ Links ]
15. Dietrich M, Hoosen AA, Moodley J, Moodley S. Urogenital tract infections at King Edward V111 Hospital, Durban, South Africa. Genitourin Med 1992;68:39-41. [ Links ]
16. Mbizvo EM, Msuya SE, Stray-Pedersen B, Sundby J, Chirenje ZM, Hussain A. Determinants of reproductive tract infections among asymptomatic women in Harare, Zimbabwe.Cent Afr J Med 2001;47(3):57-64. [ Links ]
17. Mayaud P, Uledi E, Cornelissen J, et al. Risk scores to detect cervical infections in urban antenatal clinic attenders in Mwanza, Tanzania.Sex Transm Infect 1998;74(Suppl 1):S139-146. [ Links ]
18. Hillier SL, Krohn MA, Rabe LK, Klebanoff SJ, Eschenbach DA. The normal vaginal flora, H2O2-producing lactobacilli, and bacterial vaginosis in pregnant women. Clin Infect Dis 1993;16(Suppl 4):S273-281. [ Links ]
19. Hillier SL, Nugent RP, Eschenbach DA, et al., for the Vaginal Infections and Prematurity Study Group. Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. N Engl J Med 1995;333:1737-1742. [ Links ]
20. Moodley P, Wilkinson D, Connolly C, Moodley J, Sturm AW.Trichomonas vaginalis is associated with pelvic inflammatory disease in women infected with human immunodeficiency virus. Clin Infect Dis 2002;34(4):519-522. [ Links ]
21. Chow AW, Malkasian KL, Marshall JR, Guze LB. The bacteriology of acute pelvic inflammatory disease. Am J Obstet Gynecol 1975;122(7):876-879. [ Links ]
22. Naidoo TD, Hoosen AA, Peer AK, Moodley J. Late antenatal screening for group B Sterptococcal colonization using vaginal introital/rectal swabbing: implications for maternity services in South Africa. S Afr J Epidemiol Infect 2003;18(3):48-51. [ Links ]
Accepted 22 October 2010.
Corresponding author: J Moodley (tombe@ukzn.ac.za)


{kind=link}
{kind=link}