










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.7 Pretoria jul. 2011
ORIGINAL ARTICLES
HIV/AIDS influences blood and blood product use at Groote Schuur Hospital, Cape Town
Ntobeko B A Ntusi; Mark W Sonderup
FCP (SA). Division of General Medicine, Department of Medicine, Groote Schuur Hospital and University of Cape Town
ABSTRACT
BACKGROUND: Use of blood and blood products in the medical wards at Groote Schuur Hospital, Cape Town, has increased substantially and significantly increased expenditure. It was suspected that the increased burden of HIV/AIDS could be a contributing factor.
METHODS: Doctors voluntarily completed a structured questionnaire when blood or blood products were utilised over a 3-month period in 2009. Statistical analysis was performed using Microsoft Excel, SPSS and STATISTICA.
RESULTS: Of 67 patients analysed, 46 (68.6%) were female, mean age 36.7 (standard deviation (SD) 8.7) years; 21 (31.3%) were male, mean age 39.3 (SD 13.5) years; and 41 (61.2%) were HIV positive, of whom 17 (41.5%) were on antiretroviral therapy (ART). HIV-infected patients were on average 10 years younger than HIV-uninfected patients (p=0.012). Anaemia was the cytopenia necessitating transfusion in 68.7% of cases, but its causes differed between HIV-infected and uninfected patients. The median CD4 count was 203 cells/µl (range 24 - 540) for HIV-infected patients on ART and 74 cells/µl (range 2 - 276) for those not on ART (p=0.012). The mean numbers of packed red cell and fresh-frozen plasma units transfused in the HIV-infected not on ART, HIV-infected on ART and HIV-uninfected groups were 3.3, 2.0 and 1.5 (p=0.013) and 13.5, 2.7 and 1.0 (p<0.001), respectively. ART in HIV-positive patients markedly decreased transfusion requirements (p<0.001). There was one minor transfusion reaction.
CONCLUSION: HIV/AIDS is a significant factor contributing to the increased use of blood and blood products in the medical wards at Groote Schuur Hospital. Being on ART appeared to reduce the requirement for blood and blood products.
Human immunodeficiency virus (HIV) infection is associated with cytopenias of all major blood cell lines. Anaemia occurs in up to 70% of patients with HIV/AIDS, and thrombocytopenia, neutropenia or lymphopenia in 40 - 70%.1 The incidence and severity of cytopenias correlate directly with the degree of immunosuppression, while isolated haematological abnormalities, particularly anaemia and thrombocytopenia, may be the initial presentation of HIV infection.2 HIV infection should be considered when assessing patients presenting with any cytopenia, although the causes of haematological abnormalities in HIV infection are often multifactorial.
Blood and blood products are the mainstay of therapy for severe cytopenias and coagulopathies. Apart from the risks of transfusion reactions, transmissible infection and development of allo-antibodies, blood and blood products are expensive. In the 2000/2001 financial year, the annual cost of blood transfusions in the UK was estimated to be £898 million.3 No similar cost estimation has been done in South Africa.
We noted that expenditure on and use of blood and blood products in the medical wards at Groote Schuur Hospital, Cape Town, had increased significantly for reasons that were unclear. We hypothesised that the increased burden of HIV/AIDS was a probable contributing factor, although there are few data on the effect of HIV/ AIDS on blood product use. We therefore investigated the key drivers of increased use of blood and blood products in the Division of General Medicine at Groote Schuur Hospital.
Methods
The Division of General Medicine comprises 60 beds, with additional beds in other wards due to excessive patient load. All patients admitted into these beds during a 3-month period in 2008/2009 who received a transfusion with blood or blood products were enrolled in the study. Doctors in general medicine were invited to voluntarily participate by completing a standard structured questionnaire when patients received blood or blood products. To maximise enrollment of patients, nursing staff were also asked to notify the investigators about all patients who were transfused during this period. The study was conducted as a prospective clinical audit to better inform and guide clinical management and protocols.
Simple descriptive statistics (Microsoft Excel, SPSS and STATISTICA) were used to interpret data and draw inferences about the patients studied. Results of quantitative traits are given as means (standard deviation (SD)). Categorical traits were represented as number and percentage. Pearson's chi-square or Fisher's exact tests were used to compare the relative frequency of characteristics between individuals. All p-values were two-sided, and p-values above 0.05 were considered not to indicate statistical significance.
Results
Sixty-seven patients with a mean age of 37.5 (SD10.4) years were evaluated over a 3-month period; 46 (68.6%), were female (mean age 36.7 (SD 8.7) years) and 21 (31.4%) were male (mean age 39.3 (SD 13.5) years) (Table I); and 41 (61.2%) were HIV-positive with 17 (41.5%) on antiretroviral therapy (ART). The mean age of the HIV-negative patients was 42.6 (SD 18.6) years. The mean age of the HIV-positive patients was significantly lower, 34.8 (SD 14.3) years for those on ART and 33.2 (11.9) years for those not on ART (p=0.012). The median CD4 count for HIV-positive patients on ART was 203 cells/µl (range 24 -540) and the CD4 count for those not on ART 74 cells/µl (range 2 276) (p=0.013). In keeping with the recommended first-line regimen for ART in the South African national HIV/AIDS management guidelines at the time, the combination of lamivudine and stavudine plus nevirapine or efavirenz was the most commonly prescribed ART regimen, used in 12 (70.6%) of the 17 patients on ART.
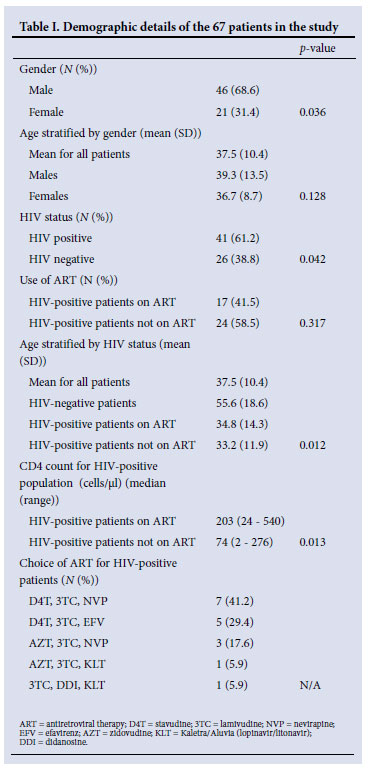
Common co-morbidities at admission in the HIV-infected group included sepsis, pulmonary and extrapulmonary tuberculosis, HIVrelated malignancy and haematological abnormalities. Malignancy and chronic systemic diseases, including cardiovascular, renal, liver, gastro-intestinal and connective tissue disorders, were more common co-morbidities in the HIV-negative patients. Infective causes and haematological abnormalities predominated as reasons for admission in the HIV-infected group, while renal (acute and chronic), liver, respiratory and cardiac disease were the major reasons for admission in the HIV-negative patients.
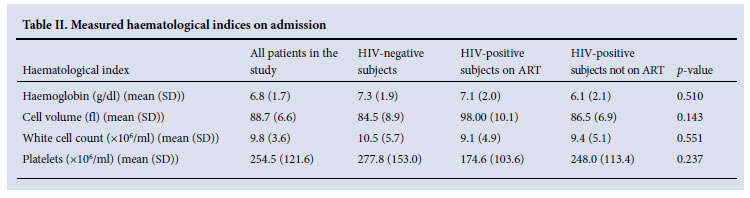
Baseline haematological parameters are listed in Table II. There were no significant differences in haematological indices, including haemoglobin concentration, white cell count, mean cell volume and platelet count, between HIV-negative patients, HIV-positive patients on ART and HIV-positive patients not on ART. The mean haemoglobin concentration was 6.8 (SD 1.7) g/dl for all patients and 7.3 (SD 1.9), 7.1 (SD 2.0) and 6.1 (SD 2.1) g/dl for the HIVnegative, HIV-positive on ART and HIV-positive patients not on ART (p=0.510) groups, respectively. The trend was similar for white cell and platelet counts in the three groups.
The indications for transfusion included anaemia (68.7%), coagulopathy (13.4%), haemorrhage (9.0%) and thrombotic thrombocytopenic purpura (TTP) (9.0%). There was no difference in the frequency of anaemia as an indication for transfusion between HIV-negative and HIV-positive patients (65.4% v. 70.7%, p=0.549). Similarly, there was no difference in the frequency of haemorrhage necessitating transfusion between HIV-positive and HIV-negative patients (9.8% v. 7.7%, p=0.421). However, coagulopathy requiring blood products was more common in HIV-negative than HIVpositive patients (26.9% v. 4.9%, p=0.028).
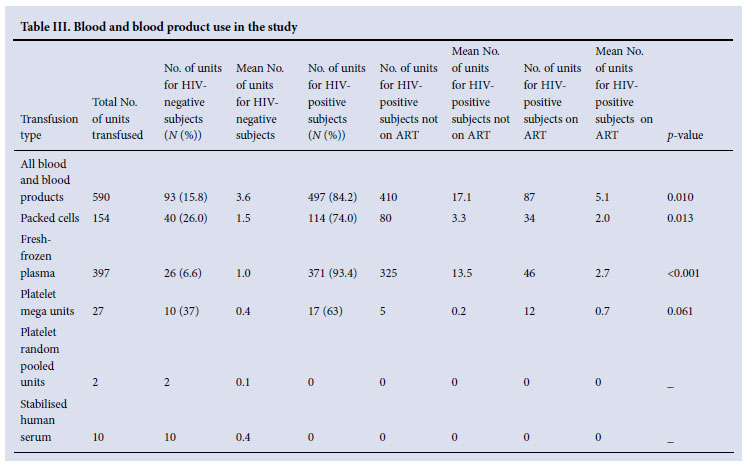
HIV positivity, particularly in patients not on ART, predicted for significantly more units of packed red cells transfused. The mean numbers of units transfused in HIV-infected patients not on ART, HIV-infected patients on ART and HIV uninfected patients were 3.3, 2.0 and 1.5, respectively (p=0.013). Similarly, the mean numbers of units of fresh-frozen plasma (FFP) transfused in the three groups were 13.5, 2.7 and 1.0, respectively (p<0.001) (Table III). Of the 590 units of blood and blood products transfused, 497 (84.2%) were used in HIV-positive patients and 93 (15.8) in HIV-negative patients (p=0.010). Most of the 497 units transfused in HIV-infected patients were used in those not on ART. A marked reduction in transfusion requirements for patients using ART was demonstrated. Of the 154 units of packed red cells used, HIV-negative patients, HIV-positive patients not on ART and HIV-positive patients on ART received 40, 80 and 34 units, respectively (p=0.013). Of the 397 units of FFP used, HIV-negative patients, HIV-positive patients not on HAART, and HIV-positive patients on HAART received 26, 325 and 46 units (p<0.001), respectively.
Only one minor adverse reaction (urticarial rash) occurred in an HIV-infected patient not on ART with a CD4 count of 36 cells/µl, who received FFP for HIV-related TTP. This resolved promptly with discontinuation of the transfusion and antihistamine therapy.
Discussion
This study provides insight into factors influencing the use of blood and blood products in patients with multi-system disease admitted to the Division of General Medicine at Groote Schuur Hospital. We demonstrated that the use of blood and blood products is significantly increased in HIV-infected patients. However, an encouraging observation is that patients on ART required significantly less blood and blood products compared with HIV-positive patients not on ART, further supporting the cost-effectiveness of ART in the management of HIV/AIDS. In keeping with the burden and demographics of HIV in South Africa, women predominated in our HIV-positive population and HIV-infected patients were on average 10 years younger than HIV-uninfected patients.
Anaemia was the commonest cytopenia necessitating transfusion (69% of patients); however, its causes differed between the HIVinfected and HIV-uninfected patients. HIV-negative patients had anaemia mainly attributable to malignancy or chronic systemic disease such as chronic kidney, liver, gastro-intestinal and/or connective tissue disorders. In contrast, HIV-infected patients had anaemia related to sepsis, haematological disorders or tuberculosis and other chronic infections. These different causes probably account for the finding that despite similar baseline haemoglobin values between the groups, HIV-positive patients received more transfusions of packed red cells than HIV-negative patients. Anaemia is the commonest haematological complication in HIV, affecting up to 80% of individuals with advancing immunosuppression.1-5 The aetiopathogenesis of HIV-related anaemia is complex and multifactorial, including HIV itself, co-morbid opportunistic infections, AIDS-associated malignancies, drugs, haemolysis, malnutrition, malabsorption or myelodysplasia.4 Anaemia in HIV is associated with an increased risk of death when patients are stratified by CD4 cell counts.6 Regular use of blood or blood products in HIV is also associated with enhancement of HIV expression and transfusion-related immunosuppression, with HIV viral loads rising after blood transfusion.7
We demonstrated that ART use is associated with a significantly reduced need for blood and blood products. HIV-induced abnormalities in myelopoiesis are also associated with recovery following ART, shown by normalisation of colony-forming units of the erythrocyte, granulocyte and monocyte cell lines after using ART for 6 months in HIV-infected patients.8 These studies suggest that in untreated HIV-infected individuals, chronic inflammation and immune dysregulation are associated with defective erythropoiesis and myelopoiesis. These are reversible following ART-induced suppression of HIV-1, thereby providing insights into mechanisms of HIV-induced bone marrow failure and pathophysiological actions of ART. The cost-effectiveness of ART has been demonstrated.9,10 This study demonstrated that ART reduces the need for and the cost of blood and blood product transfusions in HIV infection.
Although AZT is associated with myelotoxicity and is an important cause of anaemia in HIV/AIDS,11 in this study only 4 patients were on an AZT-based ART regimen. Several other commonly used drugs can also aggravate cytopenias in HIV/AIDS, e.g. co-trimoxazole.
Given the scale of the South African pandemic, the use of blood and blood products in the context of HIV/AIDS has huge economic implications. Increasing access to ART and elevating the access point to a CD4 count of 350 cells/µl will probably lessen future requirements for blood and blood product use, which will be costbeneficial in the long term.
Our study has limitations. Firstly, our sample size was limited and the findings must be validated in a larger study. Secondly, voluntary participation by doctors may mean that not all the patients receiving blood products were accounted for.
Conclusion
HIV/AIDS has emerged as a significant factor accounting for the increased use of blood and blood products in the medical wards at Groote Schuur Hospital. Patients on ART demonstrated lower blood product use indicating the cost benefit of ART. HIV negativity and the use, of ART were also associated with a decreased prevalence of cytopenias and were important factors that reduced use of packed red cells and FFP, respectively.
We declare that there are no conflicts of interest. There are no disclaimers. NN receives funding from the South African Medical Research Council, the Discovery Academic Fellowship and the Oxford Nuffield Fellowship.
References
1. Zon LI, Arkin C, Groopman JE. Haematologic manifestations of the human immunodeficiency virus (HIV). Br J Haematol 1987;66:251-256.
2. Moore RD. Anemia and human immunodeficiency virus disease in the era of highly active antiretroviral therapy. Semin Hematol 2000;7:18-23. [ Links ]
3. Varney SJ, Guest JF. The annual cost of blood transfusions in the UK. Transfusion Med 2003;13:205-218. [ Links ]
4. Moyle G. Anaemia in persons with HIV: prognostic marker and contributor to morbidity. AIDS Rev 2002;14:13-20. [ Links ]
5. O'Brien ME, Kupka R, Msamanga GI, et al. Anemia is an independent predictor of mortality and immunologic progression of disease among women with HIV in Tanzania. J Acquir Immune Defic Syndr 2005;40:219-225. [ Links ]
6. Sullivan PS, Hanson DL, Chu SY, et al. Epidemiology of anemia in human immunodeficiency virus (HIV)-infected persons: Results from the multistate adult and adolescent spectrum of HIV disease surveillance project. Blood 1998;91:301-308. [ Links ]
7. Groopman J. Impact of transfusion on viral load in human immunodeficiency virus infection. Semin Hematol 1997;34(suppl 2):27-33. [ Links ]
8. Costantini A, Giuliodoro S, Butini L, et al. HIV-induced abnormalities in myelopoiesis and their recovery following antiretroviral therapy. Current HIV Res 2010;8:336-339. [ Links ]
9. Badri M, Maartens G, Mandalia S, et al. Cost-effectiveness of highly active antiretroviral therapy in South Africa. PLoS Med 2006;3:e4. [ Links ]
10. Wood E, Braitstein P, Montaner J, et al. Extent to which low-level use of antiretroviral treatment could curb the AIDS epidemic in sub-Saharan Africa. Lancet 2000;355:2095-2100. [ Links ]
11. Richman DD, Fischl MA, Grieco MH, et al. The toxicity of azidothymidine (AZT) in the treatment of patients with AIDS and AIDS-related complex. A double-blind, placebo-controlled trial. N Engl J Med 1987;317:192-197. [ Links ]
Corresponding author: N B A Ntusi (Ntobeko.Ntusi@uct.ac.za)


{kind=link}
{kind=link}