










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.7 Pretoria jul. 2011
FORUM
ISSUES IN MEDICINE
Improving operating theatre efficiency in South Africa
A B van As; Z Brey; A Numanoglu
South African health and wellbeing indicators are poor for a middle-income country, and are usually attributed to inequity.1 Despite notable successes,2,3 South Africa's Gini co-efficient is one of the highest globally, compounded by weaknesses in implementation and planning, lack of creativity in designing incentive frameworks, and shortfalls in management and information systems.
The Western Cape Provincial Administration has developed the Comprehensive Service Plan (CSP), aided by the provincial Burden of Disease Project. The plan sets out how health services in the Western Cape will be provided; what health services will be provided at tertiary, regional and district level; and what is needed to provide the service. Its goal is to improve service delivery by ensuring that approximately 3.5 million uninsured patients using the services are treated at the level of care appropriate to their need, with better access to services.
The situation is complicated by the high levels of trauma and HIV in South Africa. Trauma is a leading cause of admission to all provincial hospitals and for patients to require a surgical procedure.4 Of all acute trauma, 80 - 90% present 'after hours'; and trauma patients often require emergency surgery. The trauma burden unpredictability and mismatch between supply and demand poses particular challenges for systems improvement and streamlining. Although the unpredictability is largely a product of the occurrence of accidents, managers and clinicians can identify patterns usefully. During office hours, work-related injuries are more likely to occur, while most stabbings and firearm injuries take place on weekends and pay days. Mapping of injury patterns can facilitate identifying the mismatch between supply and demand.
HIV/AIDS also affects the spectrum of diseases in hospitals, and its complications have increased their clinical loads. Although children infected or exposed to HIV/AIDS may have a higher rate of complications, surgery can be performed safely and should not be withheld.
Nationally, significant funds have been shifted to primary health care (PHC), and over 500 new primary level facilities constructed,5 but the latter do not function optimally.2 These services are largely nurse-driven but their development is often sub-optimal, with skills shortages, poor supply chains and inadequate support for nursebased services. The quality of care in many public hospitals is suboptimal, compounded by many higher-paid public sector employees using private health services and not being affected as services deteriorate.6
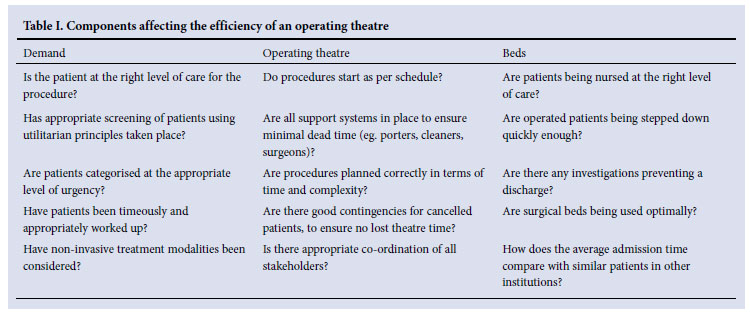
In the state health system, it is difficult to reward staff members who can improve efficiencies - they are more likely to be 'punished' for being efficient. For example, if patients are distributed across provincial services for a procedure X with an average waiting time of 3 months before the procedure can take place, an efficient facility that reduces this waiting time to 2 months will be over-burdened by patients from elsewhere, so creating a negative incentive loop. It is helpful to think of operating theatre utilisation from 3 aspects: Demand (number of patients, number of procedures); operating theatre (utilisation); and supply of beds (postoperatively). Each aspect has a set of criteria that directly affect the efficiency of any given operating theatre (Table I).
Since surgical specialists have criticised the Western Cape Department of Health because of the decline of available surgical slates, theatre efficiency is a key issue. Therefore the Department intends to develop a provincial policy to eliminate ineffective and wasteful use of the available theatre slates.
The UK's NHS has experimented with the 'Productive Ward and Productive Theatre' concept, with modest results, but the potential for further improvement was astounding. An average Trust (that has about 16 theatres) could save more than £7 million.7 This included savings on theatre time, consumables and specialist time.
Measuring theatre efficiency
Efficiency and productivity are often used as synonyms. Successful operating theatre work is based on interdependent communication and understanding between the involved parties. Unfortunately, there is still no overall definition of the concept of efficiency. Staff members generally believe that increased efficiency means increased stress and workload.8 Operating room efficiency outcomes should include patient safety, high quality of care, and cost-effectiveness and access. International indicators to measure theatre efficiency9 can be categorised into two main groups:
1. Pre-operative performance indicators
1.1 Admission time to procedure start time. This is the time difference between the admission time and the procedure start time for selected emergency procedures that may be further subdivided according to specific diagnoses. Examples are the time difference between admission time and procedure start time; e.g. stabbed abdomen (very acute), compound fracture (could probably be performed during day hours) and appendicitis (an emergency probably falling between the previous two).
1.2 Ratio elective/emergency cases. The percentage of elective and emergency cases by a hospital is also a vital measurement for measuring theatre efficiency. Hospitals that have 100% elective cases can be better and more efficiently organised than hospitals where the theatre load comprises only irregularly presenting emergencies. Studies have shown that elective cases can vary from a few per cent to 99%. Paediatric surgery units often have 70 - 80% of their cases categorised as emergencies, making theatre usage even more difficult.
1.3 Cancellation rates by reason. Measuring cancellation rates on the day of surgery by reason is an internationally accepted methodology to assess operating theatre efficiency and management. Typical categories for cancellation are: Insufficient theatre time, no postoperative bed available, changed clinical condition, cancelled by patient, and patient not ready for surgery. It may, however, be difficult to compare various hospitals since there are many complex factors that vary between hospitals that can influence the cancellation rates e.g. general workload and turn-over, and availability of both pre-and postoperative surgical beds (also specialised high care beds and intensive care beds required).
1.4 Availability of surgical beds. Availability of surgical beds is another performance indicator that assesses the availability of postoperative surgical beds (earmarked beds). The efficiency with which surgical beds are managed directly affects their availability at the right time.
2. Intra-operative performance indicators
2.1 Average procedure time. This analyses the average procedure done in minutes for common diagnoses. Studies show that few diagnoses can be compared because of the range of procedures for which it is not appropriate to calculate an average procedure time. Since South Africa's burden of disease differs from other countries, an analysis of the diagnoses that can be utilised for this measurement may be required. An innovative way to analyse this problem is to construct a 2 x 2 matrix that looks at procedure time and complexity; this allows planning around quadrants ranging from highly complex and of long duration v. highly complex and of short duration (Fig. 1).

A prerequisite for this specific measurement is to establish clear, strict and agreed-upon definitions of times e.g.:10
• Anaesthesia start time: The time when the anaesthetist is preparing the patient.
• Procedure/surgery start time: The earliest time of either specific positioning of the patient or skin preparation.
• Procedure/surgery finish time: The time when all instrument counts are complete and verified, all postoperative radiological studies performed and completed, and all dressings and drains secured.
• Patient out of room time: The time at which a patient leaves the operating theatre.
• Out of recovery time: The time at which the patient is transported out of the recovery room.
In the absence of clear definitions and understanding of these times by all staff, measurements will be insignificant.
2.2 Change-over time. Change-over time is the time between cases in minutes. There will be large differences between 'clean' and 'septic' as well as between 'emergency' and 'elective' cases. It is difficult to compare the change-over time between institutions and hospitals since many factors differ, e.g. cleaning and sterilisation of the theatre between cases may depend on the theatre infrastructure and equipment, the amount of contamination of the operating theatre during the previous procedure, and theatre staff availability.10 It is critical to determine the impact of 'controllable' hold-ups such as porters, laboratory results, equipment availability, and surgeon availability.
2.3 Ratio of utilised theatre time/total theatre time. Measuring the total procedure time as a percentage of the total time (Monday to Friday) is useful to improve the utilisation of non-surgical time through improving operating theatre management. Delays, preparation time and clean-up time or inefficient scheduling would typically account for non-surgical time.10 Theatre managers must ensure that departmental staffing matches the clinical activity and is sufficient to cover elective and emergency operating lists and to deal with the unexpected. Internationally, it is agreed that theatres should not run at 100% capacity and that a 70 - 80% utilisation is ideal. Many countries, including South Africa, run theatres at only 30 - 40%.
In these measurements, it is important to understand that any efficiency indicator of operating theatre management must consider the resource inputs to achieve such efficiency. Any overall measurements of theatre activity should be measured in terms of full staff equivalent, which is difficult in South Africa owing to shortages of nursing staff, anaesthetists and/or surgeons.
Discussion
How hospitals and operating theatres are managed and run varies significantly, and it is difficult to recommend a single format. Differences in practice of forecasting, utilisation, and management of working lists, sessions, non-elective surgery, discharge and posthospital care indicate the need for continuous system improvement.
Operating theatres are complex entities and could be described as the engine room of hospitals. To run a theatre efficiently, there must be interaction and close co-operation between theatre personnel (nurses, anaesthetists and surgeons) and many others such as porters, technicians, IT managers, supply chain people and pharmacists. Making a small change in theatre management affects the activities of many health professionals working inside and outside the theatre complex.
Effective operating theatre management depends on many external processes that may or may not co-ordinate with the operating theatres processes. The relevant and appropriateness of data and data collection processes to effectively manage operating theatres must be improved, including a strong case for considering theatre efficiencies. If a tertiary hospital with 20 theatres 'operates' 1 000 hours per week with theatres running at 60% efficiency, an increase to 70% could release over 5 000 hours of operating time per year. The emphasis should be on better utilisation of existing resources, and not solely on acquiring additional resources. This can be done in several ways by aligning demand and supply (where possible), ensuring support staff availability, maximising theatre utilisation, and optimising patient selection and surgical bed utilisation. Theatre time is said to cost R14 000 per hour.7 The relative cost saving could therefore be R70 million per annum for an institution.
We make three main recommendations to deal with these issues:
1. Allocating a director of theatre services with full budgetary authority, adequate sessional allowance, accountability and knowledge about information and administration systems is a key requirement.11 This director should be a senior staff member with a clear understanding and experience of working in operating theatres, and have a broad view across specialities.
2. A theatre manager must be appointed to each theatre, to be in charge of the day-to-day running of theatres and collecting accurate data. The appointee should preferably be a senior nurse or doctor located within the theatre complex. Both the departments of anaesthesia and surgery should appoint a specialist in each hospital, the so-called rota-maker, who ensures that all operating lists are staffed with a suitable trained clinician and that, where possible, medical staff are allocated to cover for absence.
3. Because of the complexity of theatre complex activities, proper communication is paramount. All hospitals should institute regular theatre management meetings with the different theatre user groups to anticipate and discuss problems, promulgate new ideas, agree on strategies, and report on theatre efficiency.
Conclusion
Although we tend to equate poor health care with lack of funding, the health care system can be improved by appropriate assessment of surgical procedures, taking the serious constraints into consideration. Improving the utilisation of available theatres and increasing their efficiency can be achieved by strengthening incentives for performance and linking funding more explicitly to efficiency and quality. Invigorating theatre management will add significant value and lead to better health for all.
We thank Dr A Reed and Mrs E Fourie for their valuable comments in compiling this manuscript.
1. World Health Organization. World Development Report 2001. Geneva: World Health Organization, 2001. [ Links ]
2. Department of Health. Annual report 2001/2002. Pretoria: Department of Health, 2002. [ Links ]
3. Health Systems Trust. South African Health Review 2000. Durban: Health Systems Trust, 2000. [ Links ]
4. van As AB, Navsaria P, Numanoglu A, McCulloch M. Modified sandwich vacuum pack technique for temporary closure of abdominal wounds: An African perspective. M Acta Clinica Belgica 2007;62(1):215-219. [ Links ]
5. National Treasury. Intergovernmental Fiscal Review. Pretoria: National Treasury, 2001. [ Links ]
6. Registrar of Medical Schemes. Annual Report 2001. Pretoria: Registrar of Medical Schemes, 2002. [ Links ]
7. NHS Institute. The productive theatre - improving quality and efficiency in the operating theatre. http://www.institute.nhs.uk/quality_and_value/productivity_series/the_productive_operating_theatre.html (accessed 28 February 2011). [ Links ]
8. Arakelian E, Gunningberg L, Larsson J. Job satisfaction or production? How staff and leadership understand operating room efficiency: a qualitative study. Acta Anaesthesiologica Scandinavica 2008;52(10):1423-1428. [ Links ]
9. NSW Health. Operating Theatre Management Project Report 2002. http://www.health.nsw.gov.au/pubs/2002/pdf/op_theatre_mgmt_repo.pdf (accessed 28 February 2011). [ Links ]
10. Friedman, AM, Sokal SM, Yuchiao Chang MSPH, Beger DL. Increasing operating rooom efficiency through parallel processing. Ann Surg 2006;243(1):10-14. [ Links ]
11. The Association of Anaesthesists of Great Britain and Ireland. Theatre efficiency; Safety, quality of care and optimal use of resources. August 2003. http://www.aagbi.org/publications/guidelines/docs/theatreefficiency03.pdf (accessed 31 January 2008). [ Links ]
Professor Sebastian van As is Head of the Trauma Unit at the Red Cross War Memorial Children's Hospital, and President of Childsafe South Africa.
Dr Zameer Brey is Research Assistant, Office of the Dean, UCT Medical School, and serves on the recently appointed Western Cape Health Independent Complaints Commission.
Professor Alp Numanoglu is Associate Professor in the Department of Paediatric Surgery at the Red Cross War Memorial Children's Hospital, and was heavily involved with the design of the new theatre complex.
Corresponding author: A van As (Sebastian.vanas@uct.ac.za)


{kind=link}