










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 no.6 Pretoria jun. 2011
IZINDABA
Stillbirths - an invisible earthquake
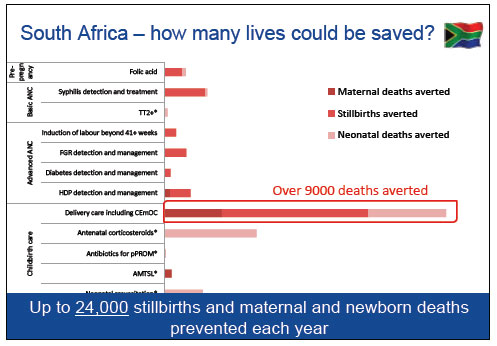
For an annual extra R35 of health care spending per person, South Africa could provide universal coverage of key interventions for maternal and infant health and prevent 49 500 annual deaths, saving the affected families a lifetime of heartache.
That optimal scenario would give a triple return on investment, avoiding 23 000 stillbirths (61 per day), 21 000 newborn deaths and 4 500 maternal deaths annually, mainly via three generic interventions. These would be: improved quality of care, (especially during childbirth), addressing overcrowding and understaffing in mainly district hospitals and developing the skills and commitment of health care workers. These interventions would also enable emergency obstetric care and treatment of maternal infections and conditions which alone would prevent up to 44% of stillbirths
These were among the interpretations of data to emerge from a comprehensive series of papers on stillbirth collated by the World HealthOrganization(WHO)and TheLancet.1 They included top South African input and boasted the first-ever international estimates of this previously unseen phenomenon. The results of the global project, published in a special edition of The Lancet this April, broke a centuries-old stigma-fuelled silence on stillbirths and began to fill a huge data vacuum, complicated by country variations in the definition of stillbirth and a baffling array of classification systems.
Professor Robert Pattinson, Director of the South African Medical Research Council and the University of Pretoria's Maternity and Infant Strategies Unit, and several of his local and international peers singled out the three generic interventions for South Africa and most other medium- to low-income countries. In South Africa, however, their efficacy would be hugely enhanced because an estimated 91% of women actually give birth in health care facilities.
South Africa well below par in reducing stillbirths
That South Africa is way behind where it should be, given its health care spending and infrastructure, is dramatically illustrated by a country-to-country comparison of the stillbirth data. Using stillbirth weights of at least 1 kg or gestational age of at least 28 weeks as the definition, they reveal South Africa to be ranked 176th among 193 countries in its numbers of stillbirths. It lies 148th in the global stillbirth rate rankings which have on average declined by 1.1% between 1995 and 2009 (the SA average decline is 0.7%). By comparison, Columbia and Mexico (comparable countries), have halved their stillbirth rates over this time. South Africa languishes alongside countries with far lower per capita incomes. Besides weak quality care systems and management, South Africa gets by with just one physician, nurse and/or midwife for every 206 people.
Dr Joy Lawn, from Saving Newborns' Lives, Save the Children (an international NGO), said that prior to the WHO/Lancet research project, only babies that died from five minutes after birth were counted in the global data. Deaths any time before this (including in utero) were excluded from the dataset, she stressed, adding forcefully, 'that's not how women count a loss!' In most countries the Millennium Development Goals (MDGs) drove maternal and child health, but stillbirths remained uncounted - and thus not addressed. Lawn said a critical issue driving the new data collection initiative was that stillbirth losses remained hidden because of the enormous societal stigma and denial attached to them. The Lancet's introductory article to its special edition, entitled 'Bringing stillbirths out of the shadows', describes the grief associated with stillbirth as 'unlike any other form of grief: the months of excitement and expectation, planning, eager questions, and the drama of labour - all magnifying the devastating incomprehension of giving birth to a baby bearing no signs of life'.
Professor Sue Fawcus, head of obstetrics at Mowbray Maternity Hospital, where the WHO/Lancet data were presented, said 42% of deliveries in South Africa happened at district hospitals, 30% at regional hospitals, 17% at community health centres and 11% at tertiary hospitals. Despite high levels of both antenatal care coverage and deliveries by a skilled birth attendant, there had only been a 0.7% reduction in stillbirths since 1995. She said the South African component of The Lancet study found that 16% of perinatal deaths were due to shortage of oxygen for the fetus in labour, while maternal conditions such as high blood pressure and placental bleeding accounted for another 23% of perinatal deaths. Other contributors (in declining proportion) were maternal diabetes, maternal infections, fetal growth restriction and congenital abnormalities. She stressed that many stillbirths occurred because 'things that should be done are not being done in the health care system', citing the 46% of perinatal deaths during childbirth thought to be avoidable and the 26 -30% of perinatal deaths related to hypertension. Other contributors to South Africa's high stillbirth toll include the lack of patient recognition of problems and access to facilities, the lack of transport between facilities and the actual lack of facilities (e.g. for C-sections). The poor quality of care included non-detection of syphilis, non-detection of poor fetal growth, non-recognition of hypertension, non-detection of maternal diabetes and substandard management of labour.
Inequities in access to health care a big driver
South African positives included folate supplementation or fortification (by law included in all bread) and the detection and management of HIV infection. The interaction of HIV and pregnancy and its effect on stillbirths remained a key research question, Fawcus emphasised. She said the South African data collected by the Perinatal Problem Identification Programme (PPIP) characterised South Africa's main challenge as enabling equitable access to improved quality of care (something the National Health Insurance plan hopes to address from next year).
The WHO/Lancet study found that globally every day more than 7 200 babies are stillborn - 'a death just when parents expect to welcome a new life' - and that 98% of them occur in low-and middle-income countries. Almost half of all stillbirths happened when the woman was in labour and were directly related to 'the lack of skilled care at this critical time for mothers and babies'.
Malika Ndlovu, a local mother, poet and performer whose third child, a daughter, Iman Bongiwe, was stillborn just over eight years ago, helped transform the data into universal tearful compassion for the Mowbray Lancet launch audience with a reading from her journal. She neatly summed up the experience of her sisters world-wide when she read: 'Except for the few birth photos, the birth and death certificate we have locked in our safe, the small grave on a hill near our home, there is little physical evidence that our daughter ever existed. Yet the entire landscape of all our lives has fundamentally changed.'2
Chris Bateman
chrisb@hmpg.co.za
1. The Lancet 2011;377:1353-1366. [ Links ]
2. Ndlovu M. Invisible Earthquake. A Woman's Journal through Stillbirth. Modjaji Books, CC, 2009 (modjaji.books@gmail.com). [ Links ]

