










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 n.5 Pretoria May. 2011
FORUM
ISSUES IN PUBLIC HEALTH
Silent casualties from the measles outbreak in South Africa
Christine Albertyn; Helen van der Plas; Diana Hardie; Sally Candy; Tamiwe Tomoka; Edward B LeePan; Jeannine M Heckmann
South Africa, home to the world's largest population of people living with HIV (5.7 million), experienced a measles outbreak that started in late 2009.1 There was a stepped increase in cases of measles, with the highest incidence reported in March 2010.2 By September 2010, more than 17 000 new measles cases had been reported to the National Institute of Communicable Diseases since January 2009. A mass vaccination campaign from mid-April to early May 2010 resulted in a significant decline in new measles cases.
The measles virus is highly contagious, and outbreaks are fuelled by overcrowding and poor vaccine coverage, making elimination status in South Africa difficult to attain. Measles may infect the central nervous system (CNS) as acute viral encephalitis, or result after 2 - 4 weeks in a post-infectious immune-mediated inflammatory disorder or acute disseminated encephalomyelitis (ADEM). There are 2 further rare and latent CNS complications resulting from a preceding measles infection: subacute sclerosing panencephalitis (SSPE) caused by years of viral persistence in a seemingly immunocompetent host,3 and subacute measles encephalitis (SME), occurring in an immunocompromised host.4
SME manifests 1 -7 months after the acute measles infection.5 Patients present with seizures, often epilepsy partialis continua, and altered mental status.5 It carries a mortality rate of 85% and survivors often have significant psychomotor retardation.5 SME has hitherto only been described in single case reports as a rare complication of measles in the context of organ transplantation,6,7 immunosuppressive therapy or immunodeficiencies,5,8 and HIV and AIDS.5,9,10 We report 8 cases of SME in HIV-infected patients who presented to a tertiary referral hospital between July and October 2010.
Case reports
The index case (Patient 1), known to be HIV-positive, presented with a 2-week history of focal twitching and clumsiness of the right hand and secondary generalised seizures on 3 occasions. Three months earlier, she contracted measles complicated by pneumonitis (Table I). She was unable to recall ever receiving measles vaccination. She recovered and commenced antiretroviral treatment (ART) 4 weeks later as well as co-trimoxazole prophylaxis. Her nadir CD4 cell count was 67 cells/µl. She had never travelled and did not abuse illicit substances.
Other than the epilepsy partialis continua (focal motor status epilepticus) of the right hand with dystonic posturing of the left foot and intermittent leg twitching, she was initially relatively well. She reported no headache, and on examination was afebrile, co-operative and not encephalopathic. Serum biochemistry including glucose was normal. She had evidence of immune reconstitution with a CD4 count of 286 and an undetectable serum HIV viral load. Cerebrospinal fluid (CSF) was acellular with normal biochemistry and negative tests for neurosyphylis and cryptococcal antigen. CSF cultures for bacteria, fungi and tuberculosis were negative. CSF polymerase chain reaction (PCR) tests were repeatedly negative for herpes simplex virus 1 and 2, cytomegalovirus, JC virus, Epstein Barr virus, herpesvirus 6, fungi, toxoplasmosis, enteroviruses and measles. The HIV viral load in the CSF was undetectable. The electroencephalogram (EEG) showed left periodic lateralised epileptiform discharges (PLEDs). Brain imaging showed no abnormalities, but there was subtle non-enhancing left frontal cortical hyperintensity on the TR sequences of the initial MRI (week 3 of SME).
The patient deteriorated rapidly over the following weeks from being independent to requiring assistance with walking and feeding. Her vision deteriorated and she developed dilated, sluggishly reactive pupils. There was no evidence of corneal or retinal involvement and no papiloedema. A repeat brain MRI showed contiguous spread of the left frontal lesion (Fig. 1) and additional multifocal T2-hyperintensities, but again limited to the cortical ribbon. A brain biopsy revealed non-necrotising encephalitis with eosinophilic inclusions, suggestive of viral aetiology. Measles PCR on brain tissue was positive, confirming SME. The seizures were finally controlled with a combination of valproate, levitiracetam and clonazepam. Despite commencement on oral ribavirin, her level of consciousness deteriorated. She is currently mute and unresponsive.

We identified a further 7 patients with either definite or probable SME. We classified as 'definite SME' a suggestive clinical picture (focal seizures and/or encephalopathy) and a positive measles PCR in either brain biopsy, CSF or urine. 'Probable SME' was diagnosed in the context of a suggestive clinical picture, normal CSF findings in the absence of other identifiable pathogens, and with supportive features such as MRI demonstrating multifocal grey matter signal abnormalities and/or positive CSF measles serology (IgG).
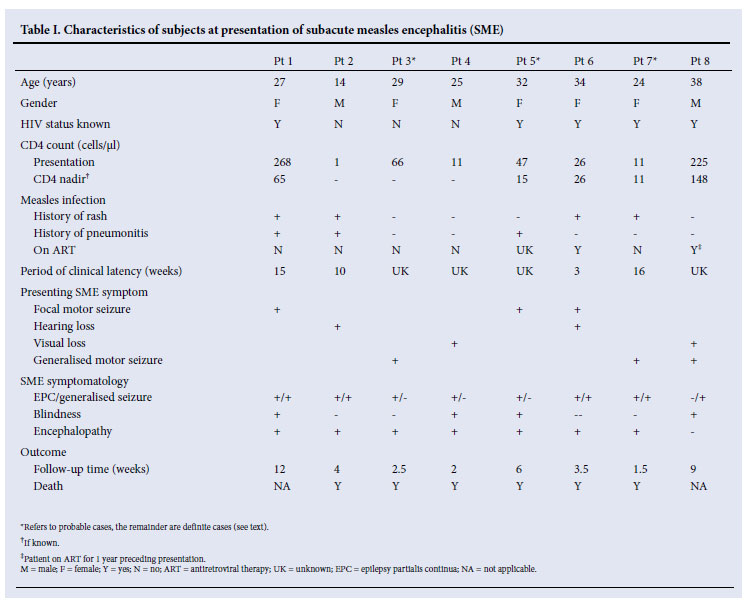
Table I shows the clinical characteristics of the 8 patients with definite and probable SME (N=3). The median age was 28 years (range 14 - 38); all were HIV-positive (newly diagnosed in 3); one was known to be on ART at the time of measles infection. The median CD4+ count at presentation was 37 (range 1 - 268); 4 had a history of a morbiliform rash, and the median time to presentation with SME following rash was 12.5 weeks. All patients developed seizures, but 3 presented with focal motor status or epilepsia partialis continua. Blindness and deafness constituted the other modes of presentation. Patient 2 developed hearing loss a few weeks after being immunised against measles as part of the nationwide measles campaign (his HIV status unknown at the time). Subsequent genotyping of the measles virus detected in his CSF revealed wild-type measles and not the vaccine strain. SME was fatal in 6 patients, and the mean time between onset of SME and death was 21 days. The clinical and radiological picture of patient 8, who may have been on ART at the time of measles infection, appears to have stabilised prior to the initiation of ribavirin between 9 and 10 weeks. He presently has normal higher mental functions and seizures are controlled on valproate.
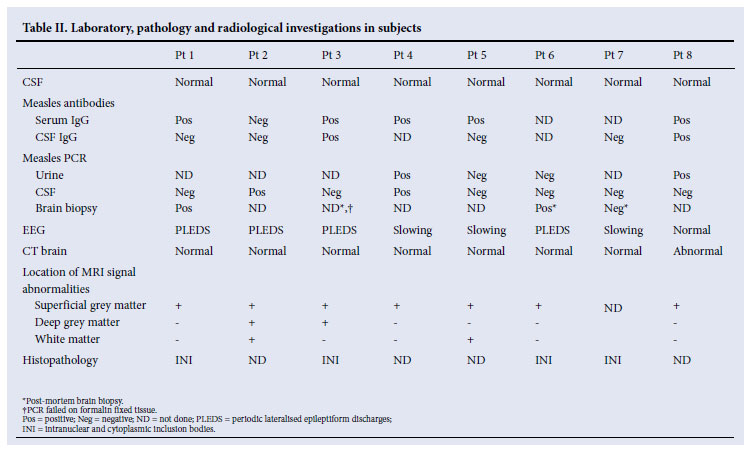
The laboratory and radiological investigations are shown in Table II. Routine CSF examinations were non-contributory. The MRI appearance was remarkably similar in the 7 patients scanned: T2-signal abnormality in a distinctive patchy cortical distribution, but in some also involving the deep basal ganglia consistent with a polioencephalopathy. White-matter abnormalities were variable and infrequent.
Discussion
This is the largest SME case series to date - and, alarmingly, collected over 4 months. All patients were HIV-positive and, with one exception, had CD4 counts <100 cells/µl at the time of measles infection, consistent with SME as an opportunistic infection in an immunocompromised host.4 The measles virus enters the CNS with the initial viraemia, but it is thought that a poor cell-mediated immune response allows virus to persist in this compartment with the potential for SME.4 Interestingly, the 2 survivors were those with the least compromised CD4 counts; one had reconstituted on ART and the other was the least affected clinically. In immunosuppressed animals infected with the measles virus, the repopulation of lymphocytes was associated with the elimination of viraemia,4 suggesting that immune reconstitution in HIV-infected patients may enable a more robust immune response. Furthermore, human leukocyte antigen (HLA) polymorphisms influence measles antibody responses, which may be a modifying factor influencing susceptibility to this measles complication.11
Focal seizures are well described in SME although the mechanism by which the measles virus induces epileptogenicity is not clear. When neurotropic measles virus is inoculated into mouse brain, neuroglial excitotoxicity (probably via N-methyl D-aspartate (NMDA)-receptor signaling) preceded neuronal hyperexcitability resulting in intermittent and later continuous seizures, followed by neuronal cell loss.12
Acute onset visual loss and deafness have been infrequently reported in SME; however, sensorineural hearing loss,13 keratitis and corneal scarring resulting in blindness, particularly in the presence of vitamin A deficiency, are known complications of acute measles.13 Preferential involvement of occipital, thalamic and putaminal areas occur in SSPE.14 In our patients with visual impairment, there was clinical evidence of anterior visual pathway involvement (abnormal pupillary responses) and, on MRI, posterior (occipital and/or temporal lobe) visual pathway involvement (Fig. 2). The recognition of visual and hearing loss may be important in considering a diagnosis of SME.

SME is an elusive diagnosis. The preceding measles rash may be subtle or absent in an immunocompromised host.4 The CSF examination may be normal, and specific measles testing using antibodies and more sensitive PCR may be negative. Absence of measles virus DNA in the CSF is probably due to the intraneuronal location of the measles virus and, unlike non-neuronal cells, viral budding and shedding does not occur in the CNS.15 Further, in the CNS, measles viral transmission occurs via trans-synaptic neuronal spread,15 which may explain the contiguous cortical spread on sequential MRI brain images (Figs 1a, b). Therefore, in the absence of finding evidence of ongoing measles virus infection in the CSF, a definitive diagnosis would require brain biopsy.
Two outbreaks of measles have occurred in South Africa in the last decade, with one still ongoing.16 Failure to vaccinate a critical percentage of the population is the probable cause. Vaccine effectiveness may be lowered in HIV infection, but the population vaccine effectiveness remained high,16 underscoring the importance of immunisation programmes in an HIV-endemic population.
The fatal intersection of HIV and measles has resulted in a cluster of patients in South Africa with subacute measles encephalitis, many of whom might have died before reaching medical attention, which serves to remind clinicians of the importance of a vigilant and effective measles immunisation programme. By reporting these patients who present with focal seizures, often with hearing and visual loss and with evidence of a polioencephalopathy on MRI, we aim to raise awareness of this devastating complication. Although insensitive, we propose the use of measles virus PCR in CSF and/or urine as a time- and cost-effective way of confirming the diagnosis of SME in the absence of a brain biospy.
The authors thank the Groote Schuur Hospital doctors who referred their cases, and Drs Hewlett and Tu who assisted with the neuropathological examinations of the post mortem specimens. HvdP is funded by PEPFAR/ USAID through the ANOVA Health Institute. The UCT research ethics committee approved the reporting of the clinical material (487/2010).
1. Siegfried CS, Wiysonge D, Pienaar N. Too little, too late: measles epidemic in South Africa. Lancet 2010;376(9736):160. [ Links ]
2. Measles Outbreak. Pretoria: National Institute of Communicable Diseases. http://www.nicd.ac.za (accessed 16 September 2010). [ Links ]
3. Reuter D, Schneider-Schaulies J. Measles virus infection of the CNS: human disease, animal models, and approaches to therapy. Med Microbiol Immunol 2010;199:261-271. [ Links ]
4. Permar SR, Griffin DE, Letvin NL. Immune containment and consequences of measles virus infection in healthy and immunocompromised individuals. Clin Vaccine Immunol 2006;13:437-443. [ Links ]
5. Mustafa MM, Weitman SD, Winick NJ, et al. Subacute measles encephalitis in the young immunocompromised host:report of two cases diagnosed by polymerase chain reaction and treated with ribavirin and review of the literature. Clin Infect Dis 1993;16(5):654-660. [ Links ]
6. Freeman AF, Jacobsohn DA, Shulman ST, et al.A new complication of stem cell transplantation: measles inclusion body encephalitis. Pediatrics 2004;114:657-660. [ Links ]
7. Kidd IM, Booth CJ, Rigden SPA, et al. Measles-associated encephalitis in children with renal transplants: a predictable effect of waning herd immunity? Lancet 2003;362:832. [ Links ]
8. Gazzola P, Cocito L, Capello E, et al. Subacute measles encephalitis in a young man immunosuppressed for ankylosing spondilitis Neurology 1999:52:1057-1059. [ Links ]
9. Budka H, Urbanits S, Liberski PP, et al. Subacute measles virus encephalitis: A new and fatal opportunistic infection in a patient with AIDS. Neurology 1996;46:586-587. [ Links ]
10. Poon TP, Tchertkoff V, Win H. Subacute measles encephalitis with AIDS diagnosed by fine needle aspiration biopsy. A case report. Acta Cytol 1998;42(3):729-733. [ Links ]
11. Dhiman N, Jacobson RM, Poland GA. Measles virus receptors: SLAM and CD46. Rev Med Virol 2004;14:217-229. [ Links ]
12. Lehrmann E, Guidetti P, Löve A, Williamson J, Bertram EH, Schwarcz R. Glial activation precedes seizures and hippocampal neurodegeneration in measles virus-infected mice. Epilepsia 2008;49(suppl. 2):13-23. [ Links ]
13. Perry RT, Halsey NA. The clinical significance of measles: A review. J Inf Dis 2004;189(suppl 1):4-16. [ Links ]
14. Prashanth LK, Taly AB, Ravi V, et al. Adult onset subacute sclerosing panencephalitis: clinical profile of 39 patients from a tertiary care centre. J Neurol Neurosurg Psychiatry 2006;77(5):630-633. [ Links ]
15. Lawrence DMP, Patterson CE, Gales TL, et al. Measles virus spread between neurons requires cell contact but not CD46 expression, syncytium formation, or extracellular virus production. J Virol 2000;74(4):1908-1918. [ Links ]
16. McMorrow ML, Gebremedhin G, van den Heever J, et al. Measles outbreak in South Africa, 2003 - 2005. S Afr Med J 2009;99:314-319. [ Links ]
Christine Albertyn, Edward B LeePan and Jeannine M Heckmann are affiliated to the Division of Neurology, Department of Medicine, University of Cape Town;
Helen van der Plas to the Division of Infectious Disease and HIV Medicine, Department of Medicine, University of Cape Town;
Diana Hardie to the Division of Virology, Department of Clinical Laboratory Sciences, University of Cape Town and the National Health Laboratory Service;
Sally Candy to the Department of Radiology, University of Cape Town;
and Tamiwe Tomoka to the Division of Anatomical Pathology, Department of Clinical Laboratory Sciences, University of Cape Town and the National Health Laboratory Service.
Corresponding author: J Heckmann (Jeanine.Heckmann@uct.ac.za)


{kind=link}
{kind=link}