










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.101 n.2 Pretoria Feb. 2011
FORUM
CLINICAL IMAGES
Vascular cause for stridor in infants
Yusuf Seedat; Savvas Andronikou; Mala Modi; Mohammed Lorgat
The double aortic arch is a form of vascular ring that constitutes a class of congenital anomalies in which the trachea and oesophagus are encircled by connected segments of the aortic arch and its branches. Although it takes various forms, the common defining feature is that both the left and right aortic arches are present.1
Case presentation
A 6-month-old infant presented with a longstanding persistent cough, episodic spells of shortness of breath, gasping-like efforts after feeding, and an unusual noise while breathing, and was reported to have turned blue on two occasions after feeding. A chest X-ray showed significant narrowing of the trachea 2 cm above the carina. An upper gastro-intestinal study (Fig. 1) showed anterior bowing and extrinsic compression of the posterior wall of the oesophagus at the mid-thoracic level, and the trachea was narrowed and showed anterior bowing. The differential diagnosis included an aberrant right subclavian artery, and a double aortic arch was suspected. A thoracic computed tomography (CT) angiogram (Fig. 2) confirmed the presence of a vascular ring created by a double-sided aortic arch with compression of the trachea and oesophagus.

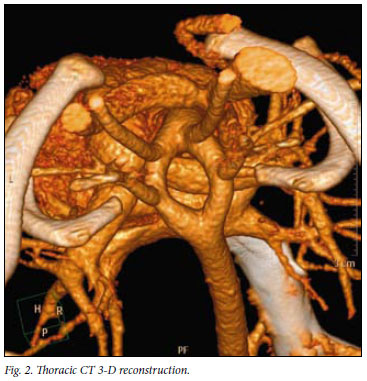
Oesophagography has a high sensitivity in detecting vascular compression of the trachea and oesophagus, and is the investigation of choice in some centres to screen for suspected vascular compression.2 In patients with a double aortic arch, bilateral indentation of the oesophagus is observed on the anteroposterior view, with the right-sided indentation superior to the left, and posterior indentation is observed on the lateral view. For a more thorough diagnostic study, CT or magnetic resonance imaging (MRI) should be performed.3 Multi-slice CT with 3-D reconstruction allows precise evaluation of any airway compromise and a detailed assessment of the anatomy of the vascular anomalies.4 MRI is also well suited for imaging vascular structures in the mediastinum without involving ionising radiation or the need for intravenously administered contrast material,5 which is a consideration in young patients, where radiation exposure should be avoided as much as possible.6
1. Chun K, Colombani PM, Dudgeon DL, Haller JA Jr. Diagnosis and management of congenital vascular rings: a 22-year experience. Ann Thorac Surg 1992;53:597-603. [ Links ]
2. Burch M, Balaji S, Deanfield JE, Sullivan ID. Investigation of vascular compression of the trachea: the complementary roles of barium swallow and echo. Arch Dis Child 1993;68:171-176. [ Links ]
3. Gürbüz A, Yetkin U, Lafçi B, Bayrak S, Göktoğan T, Özcem B. Diagnostic evaluation of incomplete double aortic arch (right dominance), VSD and PFO comorbidities with cardiac MRI. Internet Journal of Thoracic and Cardiovascular Surgery 2008;12(2). [ Links ]
4. Cerillo AG, Amoretti F, Moschetti R, Murzi B, Chiappino D. Sixteen-row multislice computed tomography in infants with double aortic arch. Int J Cardiol 2005;99(2):191-194. [ Links ]
5. Matsunaga N, Hayashi K, Okada M, Sakamoto I. Magnetic resonance imaging features of aortic diseases. Top Magn Reson Imaging 2003;14(3):253-266. [ Links ]
6. Harry MP, Kramer SS, Fellows KE. Current concepts on imaging of thoracic vascular abnormalities. Curr Opin Pediatr 2000;12(3):194-202. [ Links ]
Dr Seedat is a registrar in the Department of Radiology, University of the Witwatersrand, Johannesburg. Professor Andronikou is affiliated to the Department of Radiology, University of the Witwatersrand, and is President of the College of Radiologists of South Africa. Professor Modi was Head of the Department of Radiology, Chris Hani Baragwanath Hospital, Johannesburg, at the time of writing and is affiliated to the Department of Radiology, University of the Witwatersrand. Dr Lorgat is a paediatrician in private practice at Lenmed Clinic, Johannesburg.
Corresponding author: Y Seedat (yusufcdat@gmail.com)

