










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.100 no.12 Pretoria dic. 2010
SCIENTIFIC LETTERS
HIV prevalence and incidence in people 50 years and older in rural South Africa
C WallrauchI; T BärnighausenII; M L NewellIII
IMD, MSc. Africa Centre for Health and Population Studies, University of KwaZulu-Natal, Somkhele, KwaZulu-Natal
IIMD, ScD, MSc, MSc. Africa Centre for Health and Population Studies, University of KwaZulu-Natal, Somkhele, and Department of Global Health and Population, Harvard School of Public Health, Boston, USA
IIIPhD, MSc, MB. Africa Centre for Health and Population Studies, University of KwaZulu-Natal, Somkhele, and Centre for Paediatric Epidemiology and Biostatistics, UCL Institute of Child Health, London, UK
To the Editor: Studies of HIV prevalence in sub-Saharan Africa usually focus on the age group 15 -49 years.1 However, estimates of HIV prevalence in older people are required for health policy and planning. The health care and social needs of older HIV-infected individuals differ from younger people; e.g. because of different co-morbidities,2 different responses to antiretroviral treatment (ART),3 and the central role of older adults in African households.4 In South Africa, a nationally representative survey provided first insights into the burden of HIV in the population >50 years of age, reporting HIV prevalence in men/women as 10.4%/10.2% (in the age group 50 -54 years), 6.2%/7.7% (55 -59 years), and 3.5%/1.8% (>60 years).5 However, the South African HIV epidemic is highly heterogeneous6 with substantial variation by geographic location and ethnic group, limiting the value of national averages.
Method
We measured HIV prevalence in the age group >50 years in one of the rural communities hardest hit by the HIV epidemic in South Africa7-9 and compared it with national estimates. In addition, we estimated HIV incidence in this age group to assess whether HIV infections were acquired only among younger ages or also in older adults. We used data from the longitudinal population-based HIV surveillance conducted at the Wellcome Trust-funded Africa Centre for Health and Population Studies (Africa Centre), University of KwaZulu-Natal (UKZN), in Umkhhanyakude District, northern KwaZulu-Natal.10,11 HIV status was assessed by ELISA antibody testing of dried blood spot samples in the Africa Centre virology laboratory.10 Ethics permission for the study was obtained from the Medical Ethics Committee at UKZN. Statistical analyses were performed using STATA 10.0.
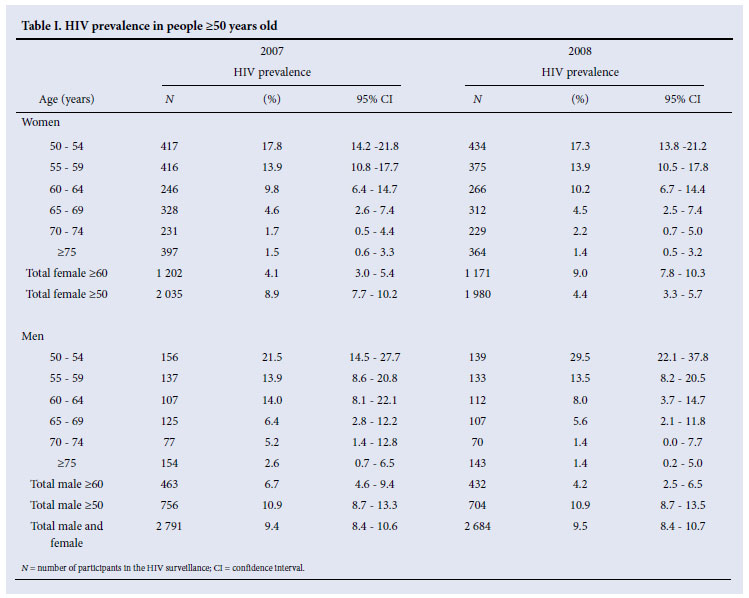
The surveillance area is largely rural, but includes a township and peri-urban informal settlements. The resident population consists of about 65 000 Zulu-speaking people.11 From 2003 to 2006, the annual HIV surveillance was limited to the age groups 15 -54 years (for men) and 15 -49 years (for women). From 2007 onwards, all adults >15 were eligible to participate. In 2007 (2008), 2 791 (2 684) people >50 years of age participated in the HIV surveillance. The crude HIV prevalence among participants was 9.4% (95% confidence interval (CI) 8.4 -10.6) in 2007, and 9.5% (95% CI 8.4 -10.6) in 2008.
Results
Table I shows HIV prevalence estimates by sex and 5-year age group for 2007 and 2008. When we accounted for selective HIV survey non-response by sex and age, the HIV prevalence estimates differed only slightly from the crude estimates: 10.6% in 2007 (11.9% in men and 8.9% in women) and 8.9% in 2008 (12.9% in men and 7.8% in women). A previous study found that controlling for selection on observed factors did not significantly affect HIV prevalence estimates in sub-Saharan Africa;12 more recent studies demonstrate that selection on unobserved factors can substantially bias results in HIV surveys in the region.13,14 In the case that people know their HIV status and refuse to participate in an HIV survey if they are HIVpositive, non-response is clearly correlated with unobserved HIV status. Future studies need to investigate the extent to which selection on unobserved factors could have biased the estimates shown here.
We regressed HIV status against demographic and geographic factors in multivariable logistic regression: sex, age (50 -64 v. >65 years old), marital status (currently married; widowed, separated or divorced; single), place of residence (urban or peri-urban v. rural), distance from the participant's household to the nearest primary road (<5 km v. >5 km), and distance from the household to the nearest primary health care clinic (<3 km v. >3 km). For individuals who participated in the HIV surveillance in 2007 and 2008, we used data from the 2008 surveillance round.
Factors independently associated with positive HIV status were: age >65 years (adjusted odds ratio (aOR) 0.20, p<0.001); currently married (aOR 0.46, p=0.001); being widowed, separated or divorced (aOR 0.47, p=0.029); and distance from household to nearest primary road >5 km (aOR 0.57, p=0.028). Associations with sex, place of residence, and distance to the nearest primary healthcare clinic did not reach significance at the 5% level.
These findings are plausible. Firstly, past studies in this demographic surveillance area found steadily declining HIV prevalence with age in men and women after peak HIV prevalence in the middle age groups,15 and the age relationship found in this regression extents this pattern to the oldest age groups. Secondly, the length of time that individuals spent without a married partner is likely to be associated with HIV risk factors, such as lifetime partners and number of risky sex acts, and hence with positive HIV status. In turn, at any given age, individuals who are currently married, widowed, separated or divorced will have spent less time without a married partner than individuals who have been single throughout their entire lifetime. Finally, investigations in the Africa Centre demographic surveillance area showed that HIV prevalence in individuals <50 years old decreases with distance from the primary roads, a relationship suggesting that easy access to transport increases the risk of HIV acquisition.16 We find that this pattern generalises to older populations.
Comparing 5-year age groups, HIV prevalence estimates in older people in this rural setting are considerably higher than national South African estimates (Table I).5 This is not surprising as the study took place in a community in South Africa with the most severe HIV epidemic among younger people.7-9 Moreover, local coverage with ART and HIV care has expanded rapidly since 2005. At the end of 2008, an estimated 21% of all HIV-infected individuals in the community were receiving ART.17 Such high ART coverage probably significantly increased average survival of HIV-infected individuals,18 which we would expect to lead to increasing HIV prevalence rates.
For HIV incidence estimation, we selected all individuals >50 years old who participated at least twice in the HIV surveillance in the period 2006 -2008, and tested HIV-negative in 2006 or 2007. Among the 1 549 participants (410 men, 1 139 women) included in the sample for HIV incidence analysis, 8 (4 women, 4 men) seroconverted in 1 575 person-years at risk. HIV incidence was 0.5 (95% CI 0.3 - 1.0) per 100 person-years overall; 0.9 in men (95% CI .3 - 2.4) and 0.4 in women (95% CI 0.1 - 1.0).
Estimates of HIV incidence in older people are rare, because longitudinal HIV surveys commonly limit data collection to younger adults. We show that HIV incidence among older adults is high in a community in rural KwaZulu-Natal. This finding is important but may not be surprising: global studies have consistently found substantial sexual activity in older men and women.19
HIV infection in older people has several distinct features - the speed of disease progression increases with age at infection,20 older people do not respond as quickly to ART, and age-related conditions may limit HIV treatment options.21 HIV prevalence is likely to increase in future years as HIV-related mortality in younger HIV-infected people continues to decrease because of ART coverage.18 Although further studies are urgently needed to identify and understand the specific HIV treatment and prevention needs of older adults in rural South Africa, our findings suggest they should not be ignored.
We thank Phumzile Dlamini, Thobeka Mngomezulu, Zanomsa Gqwede, Kobus Herbst, and the field staff at the Africa Centre for Health and Population Studies at the University of KwaZulu-Natal for their work in collecting the data used in this study, and the communities in the Africa Centre demographic surveillance area for their support and participation in this study.
The Africa Centre for Health and Population Studies in Somkhele is funded by the Wellcome Trust, UK. CW and TB received additional salary support from the Centre for International Migration (CIM), Germany. TB was supported by Grant 1R01-HD058482-01 from the National Institute of Child Health and Human Development (NICHD), National Institutes of Health, USA.
References
1. Garcia-Calleja JM, Gouws E, Ghys PD. National population based HIV prevalence surveys in sub-Saharan Africa: results and implications for HIV and AIDS estimates. Sex Transm Infect 2006;82 Suppl 3:iii64-70. [ Links ]
2. Bärnighausen T, Welz T, Hosegood V, et al. Hiding in the shadows of the HIV epidemic: obesity and hypertension in a rural population with very high HIV prevalence in South Africa. J Hum Hypertens 2008;22:236-239. [ Links ]
3. Manfredi R, Chiodo F. A case-control study of virological and immunological effects of highly active antiretroviral therapy in HIV-infected patients with advanced age. AIDS 2000;14:1475-1477. [ Links ]
4. Schatz E, Ogunmefun C. Caring and contributing: the role of older women in rural South African multi-generational households in the HIV/AIDS era. World Development 2007;35:1390-1403. [ Links ]
5. Shisana O, Rehle T, Simbayi LC, et al. South African national prevalence, incidence, behaviour and communication survey: a turning tide among teenagers? Cape Town: HSRC Press; 2009. [ Links ]
6. Tanser F, Bärnighausen T, Cooke GS, Newell ML. Localized spatial clustering of HIV infections in a widely disseminated rural South African epidemic. Int J Epidemiol 2009;38:1008-1016. [ Links ]
7. Welz T, Hosegood V, Jaffar S, Batzing-Feigenbaum J, Herbst K, Newell ML. Continued very high prevalence of HIV infection in rural KwaZulu-Natal, South Africa: a population-based longitudinal study. AIDS 2007;21:1467-1472. [ Links ]
8. Bärnighausen T, Tanser F, Newell ML. Lack of a decline in HIV incidence in a rural community with high HIV prevalence in South Africa, 2003-2007. AIDS Res Hum Retroviruses 2009;25:405-409. [ Links ]
9. Bärnighausen T, Tanser F, Gqwede Z, Mbizana C, Herbst K, Newell ML. High HIV incidence in a community with high HIV prevalence in rural South Africa: findings from a prospective populationbased study. AIDS 2008;22:139-144. [ Links ]
10. Bärnighausen T, Hosegood V, Timaeus IM, Newell ML. The socioeconomic determinants of HIV incidence: evidence from a longitudinal, population-based study in rural South Africa. AIDS 2007;21 Suppl 7:S29-38. [ Links ]
11. Tanser F, Hosegood V, Bärnighausen T, et al. Cohort Profile: Africa Centre Demographic Information System (ACDIS) and population-based HIV survey. Int J Epidemiol 2008;37:956-962. [ Links ]
12. Mishra V, Barrere B, Hong R, Khan S. Evaluation of bias in HIV seroprevalence estimates from national household surveys. Sex Transm Infect 2008;84 Suppl 1:i63-i70. [ Links ]
13. Reniers G, Eaton J. Refusal bias in HIV prevalence estimates from nationally representative seroprevalence surveys. AIDS (London, England) 2009;23:621-629. [ Links ]
14. Bärnighausen T, Bor J, Wandira-Kazibwe S, Canning D. Correcting HIV prevalence estimates for survey nonparticipation using Heckman-type selection models. Epidemiology 2011;22(1) (in press). [ Links ]
15. Bärnighausen T, Tanser F, Mbizana C, et al. Measuring the force of the HIV epidemic in a rural area of South Africa. Oral presentation, 15th Conference on Retroviruses and Opportunistic Infections (CROI) Boston, USA: 3-6 February 2008. [ Links ]
16. Tanser F, Barnighausen T, Cooke GS, Newell ML. Localized spatial clustering of HIV infections in a widely disseminated rural South African epidemic. Int J Epidemiol 2009;38:1008-1016. [ Links ]
17. Cooke G, Tanser F, Bärnighausen T, Newell ML. Population uptake of antiretroviral treamtent through primary care in rural South Africa. BMC Public Health 2010;10:585. [ Links ]
18. Herbst AJ, Cooke GS, Bärnighausen T, KanyKany A, Tanser F, Newell ML. Adult mortality and antiretroviral treatment roll-out in rural KwaZulu-Natal, South Africa. Bull World Health Organ 2009;87:754-762. [ Links ]
19. Nicolosi A, Laumann EO, Glasser DB, Moreira ED Jr, Paik A, Gingell C. Sexual behavior and sexual dysfunctions after age 40: the global study of sexual attitudes and behaviors. Urology 2004;64:991-997. [ Links ]
20. Time from HIV-1 seroconversion to AIDS and death before widespread use of highly-active antiretroviral therapy: a collaborative re-analysis. Collaborative Group on AIDS Incubation and HIV Survival including the CASCADE EU Concerted Action. Concerted Action on SeroConversion to AIDS and Death in Europe. Lancet 2000;355:1131-1137. [ Links ]
21. Martin CP, Fain MJ, Klotz SA. The older HIV-positive adult: a critical review of the medical literature. Am J Med 2008;121:1032-1037. [ Links ]
Accepted 16 August 2010.
Corresponding author: T Bärnighausen (tbarnighausen@africacentre.ac.za)


{kind=link}