










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.100 no.12 Pretoria dic. 2010
FORUM
HEALTH POLICIES AND PRACTICE
Setting priorities for health in 21st-century South Africa
Karen J Hofman; Stephen M Tollman
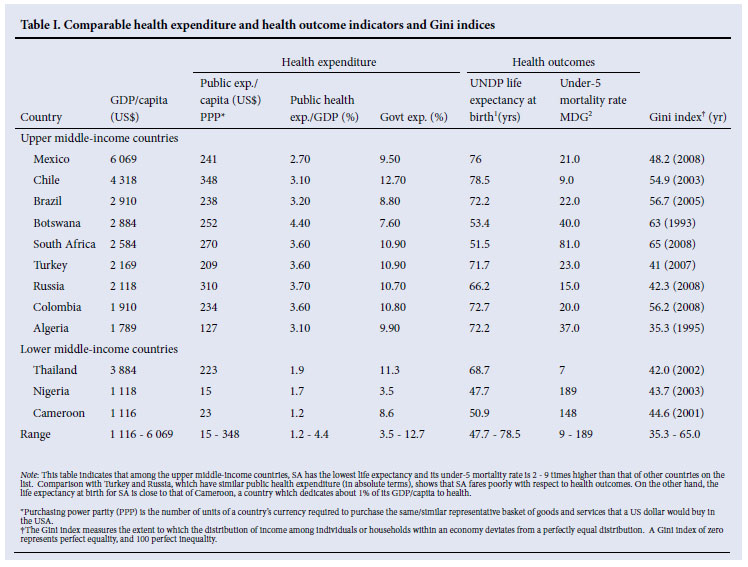
South Africa (SA) commands financial health care resources comparable to Brazil, Mexico and Thailand. Despite spending similar amounts in the public sector (3.5% of gross domestic product (GDP) in terms of purchasing power parity, these and other countries have far better health outcomes than SA on almost all measures including life expectancy and maternal mortality (Table I).1,2 While the combined impact of HIV and tuberculosis (TB) on all-cause mortality has been immense, this only partially explains the plummeting life expectancy in SA from 63 years in 1990 to 45 years in 2007. Furthermore, SA is one of only 12 countries worldwide with a marked reversal of maternal and infant mortality, reflecting the complex epidemiological transition underway.3 An increasing percentage of the population now dies from chronic, non-communicable diseases such as vascular illness, diabetes and cancers and from violence and injury.4
Despite the global economic crisis, annual national SA government health expenditures are projected to rise by an average of 7.1% per year between fiscal years 2009/10 and 2012/13, with costs close to ZAR 100 billion for 2009/10.5 After a decade that posed many challenges, issues of health care delivery and services are now squarely on the table. Given that 85% of the population depends on the public sector, in times of fiscal restraint two broad questions that should be addressed are: will the public be getting good value for their health care rand, and what criteria will be used to inform the allocation of resources that will ensure equal access to high quality health care?
What is the basis for health care spending in South Africa relative to similarly resourced nations, and how does it compare by district or province within the country itself? First, public sector expenditure, at approximately R1 600 or US$200 per person per annum, is approximately 4 times the sum expended in other countries of sub-Saharan Africa. Likewise, the per capita costs of a package of interventions to save maternal and neonatal lives in SA is 2 -4 times that of Cameroon and southern Nigeria, regions with similarly resourced health systems.6 The difference is largely a function of input costs, human resources in particular. Secondly, within SA the per capita expenditure on non-hospital primary care varies considerably by province and by district, ranging from a high of R505 per person to R220.7 These figures do not reflect out-of- pocket payments and direct costs to families and patients themselves. For example, in 2006 in one rural province, up to 60% of monthly expenditure was consumed on seeking health care, with transport costs accounting for a significant portion.8
Against this background, since the 2009 national elections the government has renewed assurances to improve health care, including:
• expanded social grants impacting on household income, with positive effects on nutrition and school attendance (National Treasury 2010)5
• promoting cost-effectiveness and phasing out or redesigning ineffective programmes to ensure greater value for money9
• improving health care at the district level10
• introducing a National Health Insurance (NHI) system. During these deliberations, several groups have developed projected costs, with little consensus. Some differences depend on the predicted extent of health coverage.11
Improved knowledge about effective health care interventions and policy systems requires more careful scrutiny of available evidence and ensuring that costs are taken into account. If this is not done, health care spending will continue to rise with uncertain benefits for population health.
Challenges
To ensure progress, many proposed policies imply that we need a better understanding of where efficiency gaps exist to avoid waste, and how to deploy existing resources more effectively to improve quality. In considering how to accomplish these goals, SA faces the following key challenges:
Expertise to perform health economic evaluations. While the National Department of Health (DOH) provides dedicated funding for HIV/AIDS programmes, the remaining budget for health is contingent on provincial allocations. This depends on effective provincial-level requests for resources that might otherwise be allocated to other sectors. The limited capacity in provincial health departments to negotiate budgets with the provincial treasury is part of a broader issue of lack of proficiency to undertake health economic evaluations across the country.
Costly and inefficient approaches to health personnel management. These have lagged behind developments elsewhere in sub-Saharan Africa, such as Malawi and Tanzania. Human resources are the major cost driver for health care in SA, ranging from 50% to 70% of costs. This suggests an urgent need to develop feasible South African responses to task shifting and effective structures, financial incentives and balancing the skill sets of diverse health workers.12
Health services delivery, especially at the primary care and district level. Considering the unique and extreme burden of HIV/AIDS and TB in SA,13 it should be appreciated that these infectious illnesses are paralleled by a rising burden of vascular disease, diabetes and cancer.4 Leveraging the current, predominantly vertical HIV programmes more broadly for other chronic diseases is essential. Even within successful integrated models of care, for example the integrated management of childhood illness (IMCI), a better understanding of specific priority interventions and how to adapt these to existing public health services is needed in SA.
Available data are seldom linked to the limited evidence base informing programme and system development. With respect to costs of providing services, we have some information in the areas of HIV and TB as well as maternal and child health.3,14 However, a preliminary review of utilisation costs and district-level data regarding chronic disease services suggests that such information is limited.
Fair access to services, or equity. In the post-apartheid era the Gini coefficient in SA has risen from 0.56 in 1995 to 0.67 in 2009.15,16 This means that the gap between rich and poor has risen significantly. Data on aggregate health outcomes mask ongoing disparities between groups that are largely based on race; in 2009 white South Africans were expected to live on average 23 years longer than blacks.17 Nearly 60% of all poor households in SA reside in rural areas with compromised access to health care. These and other concerns fuel the debate on how to embed the notion of equity when performing an economic evaluation. Poorer people bear a greater burden of illhealth, so many highly effective interventions would have greater impact on reducing the burden of disease if service coverage were high and patient/client access was good.
Moving forward
Cost-effectiveness work has been ongoing in SA, principally but not exclusively focused on HIV/AIDS. Other analyses have addressed the cost-effectiveness of vertical interventions related to tuberculosis, malaria, hypertension, food fortification and vaccines.18 Similarly, the World Health Organization CHOICE project developed data for 15 sub-regions including sub-Saharan Africa on effective interventions that can save lives at lower cost.19 However, none of this was tailored to specific country or sub-national settings.
Since 2009, an initiative called PRICELESS SA (Priority Cost Effective Lessons for Systems Strengthening - South Africa) has started addressing some of these needs. The project falls within the umbrella of the Disease Control Priorities Network at the University of Washington, Seattle, and is part of a wider network of countries, including India, that are beginning to undertake similar efforts.20 A key innovation taking place within PRICELESS SA is for economic evaluation, not just to measure the vertical intervention but to take account of the efficiencies possible from system-level interventions directed at the platforms used to deliver preventive and curative care. An example is the district level, which includes primary care, clinic services and vital surgical units.
The Secretariat for PRICELESS, hosted by the MRC/Wits Rural Public Health and Health Transitions Unit at the School of Public Health, University of the Witwatersrand, seeks to provide such information at a critical moment for SA policymakers. Governance is reflected in a Steering Committee which includes the DOH, the Medical Research Council (MRC), the Treasury, the Department of Science and Technology and the Health Systems Trust. This catalytic venture, guided by the Steering Committee, will address integrated care for chronic diseases (infectious and non-communicable) and maternal and child health, and how these fields map to the primary care delivery platform. The intent is to perform several analyses to demonstrate how economic evaluation can be used as a factor to guide priority investments in the health sector. The initiative seeks to strengthen local expertise to perform cost-effectiveness analysis and related work. An interactive website is under development to allow information and products to be shared with a wider national and regional/international audience and for contact with the secretariat (www.pricelesssa.ac.za).
Budget and expenditure monitoring must go beyond HIV/AIDS. This is as critical for the public as for policymakers. A SA government green paper has noted that when assessing performance, it is important to consider not only the service delivery outcomes (e.g. quality, access, equity, timeliness) but also the financial dimensions of performance (effectiveness, efficiency and economy).21 The PRICELESS project is aligned with these goals. Its accomplishments will depend on how well the resulting evidence is adapted and implemented, and also on the level of investment in building health economics capacity in SA. Its success also hinges on whether the examples generated are sufficiently compelling for this approach to be justified as one of several essential tools in priority setting. Demonstrating feasible solutions could allow for their application in other Southern African Development Community (SADC) countries and more widely across the region.
In SA and further afield there is a need to promote dialogue to strengthen the brokering of 'evidence to policy' between scientists and public sector leadership and management.22 One approach would be to establish a forum to encourage an ongoing exchange between government officials in Treasury and Health. Ideally this should take place simultaneously at provincial level, with efforts to institutionalise well-structured and ongoing brokering mechanisms. Of critical importance, knowledge and understanding of cost-effective health interventions could enable policy makers in the DOH to operate on a par with their counterparts in Treasury.
In summary, the intent of PRICELESS SA is to be catalytic, to show where efficiency can be gained at reasonable cost, and to stimulate further work along these lines. Ultimately it is hoped that policymakers and health care providers will value and incorporate this approach into future planning for health services at both the national and at the district level.
The authors have no conflict of interest. We wish to acknowledge the many individuals who have participated in workshops and have contributed to framing PRICELESS SA ideas and work-plan. We also appreciate the support of the MRC South Africa. We recognise assistance of Mandy Maredza and Patrizia Favini in preparation of the manuscript. The PRICELESS SA initiative receives funding from the Bill and Melinda Gates Foundation through the DCP-Network at the University of Washington, Seattle, and the Fogarty International Center at the US National Institutes of Health.
1. UNDP. Human Development Report 2009: Human development index 2007 and its components. 2010. http://hdrstats.undp.org/en/indicators/88.html (accessed 12 April 2010). [ Links ]
2. United Nations. Millennium Development Goals Indicators: The official United Nations site for the MDG indicators. 2010. http://unstats.un.org/unsd/mdg/SeriesDetail.aspx?srid=561 (accessed 12 April 2010). [ Links ]
3. Chopra M, Daviaud E, Pattinson R, Fonn S, Lawn JE. Saving the lives of South Africa's mothers, babies and children: can the health system deliver? Lancet 2009;374:835-846. [ Links ]
4. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet 2009;374:934-947. [ Links ]
5. National Treasury. National Budget Review - Social Security and Health Care Financing, Pretoria: Department: National Treasury, Republic of South Africa, 2010. [ Links ]
6. Kinney MV, Lawn JE, Kerber KJ, eds. Science in Action: Saving the Lives of Africa's Mothers, Newborns and Children. Cape Town: Report for the African Academy Science Development Initiative, 2009. [ Links ]
7. Day C, Monticelli F, Barron P, Haynes R, Smith J, Sello E, eds. The District Health Barometer 2008/09. Durban: Health Systems Trust, May 2010. [ Links ]
8. Goudge J, Gilson L, Russell S, Gumede T, Mills A. Affordability, availability and acceptability barriers to health care for the chronically ill: longitudinal case studies from South Africa. BMC Health Services Research 2009;9:75. [ Links ]
9. The Presidency, Republic of South Africa. Improving Government Performance: Our Approach. Pretoria: The Presidency, 2009. [ Links ]
10. Department of Health. National Department of Health Strategic Plan 2010/11-012/13. http://www.doh.gov.za/docs/misc/stratplan/201011-01213a/chapter_3.pdf (accessed 21 July 2010). [ Links ]
11. Innovative Medicines South Africa. Platform for the sharing of National Health Insurance information sources. http://www.imsa.org.za/files/Library/NHI/NHI%202010/IMSA%20NHI%20in%20South%20Africa%202010%20vF1%203%20February%202010.pdf (accessed 21 September 2010). [ Links ]
12. Fonn S, Ray S, Blaauw D. Innovation to improve health care provision and health systems in sub-Saharan Africa - promoting agency in mid-level workers and district managers. Global Public Health 2010;1-12. [ Links ]
13. Abdool Karim SS, Churchyard GJ, Abdool Karim Q, Lawn SD. HIV infection and tuberculosis in South Africa: an urgent need to escalate the public health response. Lancet 2009;374:941-953. [ Links ]
14. Cleary S. 'Long term costs and implications for sustainable budgeting', BEMF Inaugural meeting, 21 August 2009, Hillbrow Health Precinct, Johannesburg, 25 August, Section 27. http://www.section27.org.za/files/2010/03/Long-term-costs-and-implications-for-sustainable-budgeting-Susan-Cleary.pdf (accessed 21 July 2010). [ Links ]
15. Bhorat H, Van der Westhuizen C, Jacobs T. Income and Non-Income Inequality in Post-Apartheid South Africa: What are the Drivers and Possible Policy Interventions? Working Paper 96114. Cape Town: University of Cape Town Development Policy Research Unit, 2009. [ Links ]
16. The Presidency, Republic of South Africa. Development Indicators 2009. Pretoria: The Presidency, 2009. [ Links ]
17. South African Institute of Race Relations. http://www.sairr.org.za/research-and-publications/southafrica-survey-2008-2009 (accessed 21 July 2010). [ Links ]
18. Disease Control Priorities Project. http://www.dcp2.org/main/Home.html (accessed 29 October 2010). [ Links ]
19. WHO CHOICE project. http://www.who.int/choice/en/ (accessed 21 September 2010). [ Links ]
20. Jha P, Laxminarayan R. Choosing Health: An Entitlement for All Indians. Toronto: Centre for Global Health Research, 2009. [ Links ]
21. The Presidency, Republic of South Africa. Improving Government Performance: Our Approach. Pretoria: The Presidency, 2009. http://www.info.gov.za/view/DownloadFileAction?id=106599 (accessed 21 September 2010). [ Links ]
22. Alliance for Health Policy and Systems Research, World Health Organization. Sound Choices: Embracing Capacity for Evidence-informed Health Policy, Geneva: World Health Organization, 2007. [ Links ]
Karen Hofman, MB BCh, is Director of the Division of International Strategic Planning, Policy and Evaluation at the Fogarty International Center at the National Institutes of Health and has developed a range of novel programmes to build research proficiency in low-and middle-income nations. A paediatrician with sub-specialty training in childhood disabilities and genetic disorders, she is an Honorary Associate Professor at the School of Public Health, University of the Witwatersrand, and co-director of the PRICELESS-SA initiative based at the MRC/Wits Rural Public Health and Health Transitions Research Unit.
Steve Tollman, BSc, MMed, MA, MPH, PhD, directs the MRC/Wits Rural Public Health and Health Transitions Research Unit (Agincourt), heads the Health and Population Division in the School of Public Health, University of the Witwatersrand, and is guest professor in the Centre for Global Health Research, Umeå University, Sweden. The MRC/Wits-Agincourt Unit supports a broad-based initiative to apply economic evaluation to health development in South Africa. Steve was founding Board chair of INDEPTH (International Network for the Demographic Evaluation of Populations and Their Health) and is principal investigator for Network efforts in adult health and ageing.
Corresponding author: K J Hofman (hofmank@mail.nih.gov)


{kind=link}