










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.100 n.11 Pretoria Nov. 2010
ORIGINAL ARTICLES
Pharmacological testing in Horner's syndrome - a new paradigm
Derrick P Smit
MB ChB, Dip Ophth, MMed (Ophth), FC Ophth (SA). Division of Ophthalmology, Faculty of Health Sciences, Stellenbosch University, W Cape
ABSTRACT
For more than three decades, topical cocaine has been used to confirm the diagnosis and hydroxyamphetamine to localise the causative lesion in oculosympathetic palsy or Horner's syndrome. More recently, other drugs have demonstrated the ability to point to the diagnosis or anatomical site. Apraclonidine and phenylephrine, given their similar diagnostic efficacy and increased availability, may have superseded cocaine and hydroxyamphetamine as firstline pharmacological testing agents in Horner's syndrome.
Thompson and Mensher1 described the topical use of cocaine to confirmthediagnosisofHorner'ssyndrome andhydroxyamphetamine to distinguish between pre-and postganglionic causative lesions. For almost 40 years, these drugs have been the mainstay of pharmacological testing in Horner's syndrome. Recently, however, other drugs have been studied that assist in diagnosing or localising the lesion. These include pholedrine, apraclonidine, adrenaline and phenylephrine. A Pubmed search combining each of these drugs with Horner's syndrome was conducted to ensure that recent, relevant evidence is included in the discussion of each drug.
Pharmacological testing
Cocaine
Topical cocaine 2 -10% causes mydriasis in normal pupils, as it inhibits the re-uptake of noradrenaline (NA) at postganglionic sympathetic nerve endings.2 NA therefore accumulates in the synaptic cleft and stimulates the dilator muscle of the pupil. If the sympathetic innervation is disrupted anywhere along its course, no NA will be secreted and cocaine will therefore not cause mydriasis, confirming the diagnosis of Horner's syndrome. This test is highly effective in distinguishing between patients with and those without Horner's syndrome. In one study, anisocoria of 0.8 mm after the instillation of topical cocaine 10% in both eyes gave an odds ratio of 1 050:1 that Horner's syndrome was present.3 Some authors advocate anisocoria of >1 mm as a positive test outcome, given the difficulty of accurately measuring pupil size below 1 mm.4
Unfortunately, the cocaine test has drawbacks: (i) some clinicians find it difficult to obtain the drug owing to its scheduling status, and in some countries it is not available at all; (ii) cocaine inhibits the uptake of hydroxyamphetamine from the nerve terminal and the two tests therefore cannot be conducted on the same day; (iii) metabolites of cocaine may remain in urine for up to 2 days after an ophthalmological test, which has implications for patients who may be subjected to a drug-screening test of their urine;5 (iv) sensitivity of the test is reduced in cases where the interruption of the sympathetic pathway is incomplete; and (v) the response in patients with dark irides may be extremely slow, and up to 3 hours should be allowed before interpreting the results.
Hydroxyamphetamine
Hydroxyamphetamine belongs to a group of indirect-acting adrenergic mydriatics, e.g. tyramine, amphetamine and ephedrine.1 These drugs cause endogenous NA to be released from sympathetic nerve endings and therefore do not stimulate the effector cells directly. In 1971, hydroxyamphetamine (Paredrine) was readily available and widely used and therefore chosen as the drug of choice to distinguish between postganglionic and preganglionic or central causes of oculosympathetic palsy (OSP).
If a central or preganglionic lesion is present, instillation of hydroxyamphetamine should cause mydriasis of the pupil, as the postganglionic neuron is intact and therefore able to release NA. Damage to the postganglionic neuron will result in less or no NA being released, and mydriasis will be incomplete or absent in response to topical hydroxyamphetamine.
There are drawbacks regarding the use of hydroxyamphetamine: (i) it is no longer available commercially; (ii) the test cannot be performed on the same day as the cocaine test; and (iii) falsenegative results from a variety of causes have been reported in acute OSP.6,7 These have been ascribed to NA stores in postganglionic oculosympathetic terminals that are probably not yet depleted in the acute phase of the syndrome.
Pholedrine
Pholedrine is the N-methyl derivative of hydroxyamphetamine and has been suggested as an alternative drug in localising the causative lesion in OSP. In a study by Bates et al.,8 pholedrine correctly distinguished between pre-and postganglionic lesions in all 13 patients with OSP. The mean potency compared with hydroxyamphetamine is 0.62, and a 1% concentration has a similar effect to a 0.5% concentration of hydroxyamphetamine.8 Unfortunately, its use is restricted owing to its limited availability in some countries.
Apraclonidine
Apraclonidine (Iopidine; Alcon, Fort Worth, Texas) is an alphaadrenergic receptor agonist normally used for the short-term reduction of intra-ocular pressure (IOP). Its IOP-lowering effect results from reduced production of aqueous humour via its action on postjunctional α2-receptors in the ciliary body. The α1-activity of apraclonidine does not affect aqueous production, but results in conjunctival vasoconstriction that is often noted with its use.9 In OSP, sympathetic denervation results in upregulation of α-receptors which, in turn, unmasks the weak effect of apraclonidine on α1-receptors in the pupil dilator muscle by causing mydriasis.
In 6 patients with both pre-and postganglionic OSP, one drop of 1% apraclonidine caused mydriasis of between 1.0 mm and 4.5 mm in the affected pupil. Unaffected eyes showed <0.5 mm of mydriasis and consequently the instillation of 1% apraclonidine caused reversal of anisocoria, with the miotic OSP pupil becoming larger than the normal pupil. This reversal of anisocoria is easily detected with the naked eye.10 Another study, with 0.5% apraclonidine, showed reversal of anisocoria of at least 0.5 mm in 7 out of 8 patients with OSP.11
The exact sensitivity of apraclonidine in the diagnosis of Horner's syndrome remains uncertain, largely owing to small sample sizes. One study calculated the sensitivity of apraclonidine compared with that of cocaine in the diagnosis of all forms of OSP as 91% (N=11),12 while another reported a sensitivity of 100% (N=9).13 More recently, apraclonidine testing for OSP was reported in 65 patients in whom the diagnosis had previously been confirmed with cocaine testing. Two false-negative results were recorded, while in 3 patients reversal of anisocoria only occurred under high illumination.14,15 This finding implies an overall sensitivity of 96.9% compared with cocaine, but a formal meta-analysis has yet to be done. Apraclonidine 1% has been successfully used to diagnose OSP in paediatric patients,10 even though 5 infants experienced systemic side-effects after topical use of 0.5% and 1.0% apraclonidine.16 The side-effects included lethargy, difficulty to rouse, bradycardia and shallow respiration with decreased oxygen saturation of 8 - 10 hours, which are similar to those with topical brimonidine. Four of the infants were younger than 6 months. It has been suggested that apraclonidine should be used with caution, or not at all, in this age group, owing to relative immaturity of the blood-brain barrier. No adverse systemic effects were reported when 0.5% apraclonidine was used to test 10 children over the age of 1 year, and 0.5% apraclonidine was equally sensitive compared with 4% cocaine.17
Another drawback of apraclonidine is that up-regulation of α1-receptors takes between 5 and 8 days to develop,18 which explains why false-negative results may be obtained with apraclonidine testing in acute cases of OSP.19 The shortest reported latency period between sympathetic damage and a positive apraclonidine test is 14 days.14 Cocaine and apraclonidine are both useful in confirming the diagnosis of OSP, but cannot distinguish between pre- and postganglionic causes of the syndrome.
Apraclonidine achieves its peak IOP-lowering effect 3 -5 hours after topical administration and has an elimination half-life of 8 hours.20 The duration of mydriasis is not specified, but additional testing to localise the lesion should be postponed by a few days because of the relatively long half-life of the drug. No studies addressing this issue have been published. Despite these limitations, many authors have recently suggested the use of apraclonidine as a first-line diagnostic tool for OSP, with cocaine being reserved for cases where apraclonidine testing is negative despite strong clinical suspicion.
Adrenaline
Adrenaline is a direct-acting sympathomimetic because of its structural similarity to NA that acts as the neurotransmitter in the sympathetic pathway. It therefore directly stimulates effector cells such as the dilator muscle of the pupil if the concentration is sufficient and causes mydriasis. Should denervation hypersensitivity develop, marked mydriasis will occur - even in minute concentrations of adrenaline, e.g. 1:1 000.
Monoamine oxidases (MAO) A and B are located on the outer membrane of the mitochondria inside most neurons, including those of the sympathetic pathway, where they are responsible for the oxidative deamination of monoamines such as NA and adrenaline into the corresponding aldehyde and ammonia.
Should a lesion that causes OSP affect the preganglionic neuron, MAO in the postganglionic neuron will still inactivate any adrenaline or NA present and, despite denervation hypersensitivity, neither pupil will dilate after the instillation of adrenaline 1:1 000. However, should the postganglionic neuron be affected, no MAO will be present to metabolise any adrenaline. As a result of denervation hypersensitivity, the affected pupil will dilate while the normal pupil will be insensitive to the low concentration of adrenaline. As such, adrenaline 1:1 000 may help to distinguish between pre- and postganglionic lesions causing OSP.
Unfortunately, adrenaline penetrates the cornea poorly and sensitivity to the drug differs greatly, often causing inconclusive results and thereby diminishing its clinical value.1
Phenylephrine
Thompson and Mensher1 found that phenylephrine was more useful than adrenaline when testing supersensitivity of the iris dilator muscle, but they mostly used a 10% solution that causes extensive mydriasis even in a normal pupil.
A study comparing pupil responses to phenylephrine 1% and hydroxyamphetamine 1% in 14 consecutive patients with OSP after previously confirming the diagnosis with cocaine 10%21 found that phenylephrine 1% increased pupil size in postganglionic OSP by a mean of 2.3 mm compared with 0.2 mm in the contralateral normal pupil. It proved to be 81% sensitive and 100% specific in dilating the pupil in postganglionic OSP. This compared favourably with the 93% sensitivity and 83% specificity of hydroxyamphetamine 1%.
However, the use of phenylephrine has limitations. The extent of denervation determines the degree of supersensitivity. It may therefore be difficult to distinguish preganglionic lesions from partial postganglionic lesions. False-positive or negative errors may result from variable drug penetration through the cornea. Sensitivity of the iris to phenylephrine increases by 0.23 mm per decade after the age of 20 years. Denervation hypersensitivity develops over time, although positive phenylephrine tests have been reported as early as 10 days after symptoms were noted.22
Given the limited availability of hydroxyamphetamine and the similarities in sensitivity and specificity of the two drugs in localising a lesion to the postganglionic neuron, phenylephrine 1% appears to be the more reliable and readily available alternative.
Conclusion
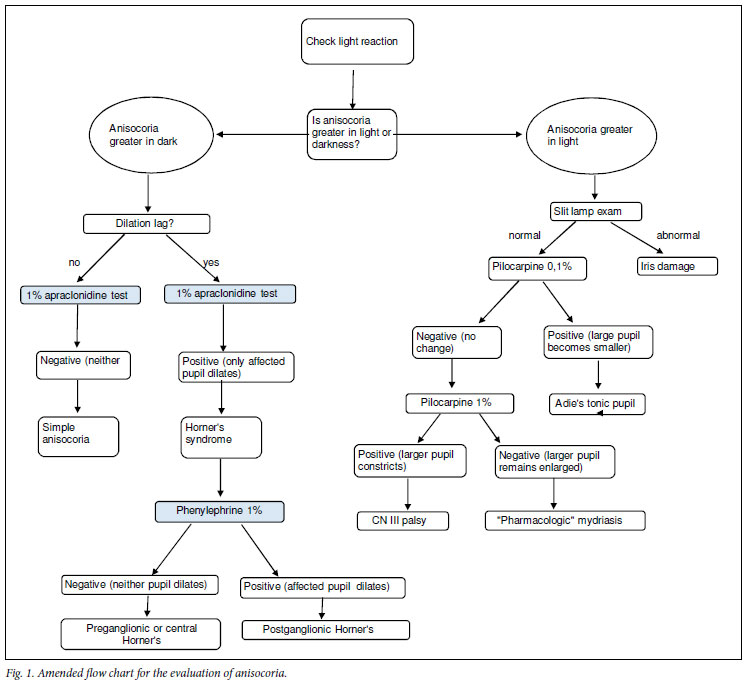
Thompson and Pilley2 compiled a flow chart for use in sorting out anisocorias. For more than 30 years, cocaine 2 -10% has been the gold standard in the diagnosis of unilateral Horner's syndrome and hydroxyamphetamine 1% recommended to localise the causative lesion. As neither is readily available, drugs recommended for primary use in pharmacological testing of this syndrome are being reconsidered. It seems that apraclonidine 0.5% or 1% is a suitable alternative to cocaine in confirming the diagnosis of OSP, and that phenylephrine 1% is a reliable and readily available alternative to hydroxyamphetamine. I therefore propose an amended flow chart for anisocorias (Fig. 1) and support the use of these drugs as first-line agents in unravelling the intricacies of Horner's syndrome.
References
1. Thompson HS, Mensher JH. Adrenergic mydriasis in Horner's syndrome. Hydroxyamphetamine test for diagnosis of postganglionic defects. Am J Ophthalmol 1971;72:72-480. [ Links ]
2. Thompson HS, Pilley SF. Unequal pupils. A flow chart for sorting out the anisocorias. Surv Ophthalmol 1976;21:45-48. [ Links ]
3. Kardon RH, Denison CE, Brown CK, Thompson HS. Critical evaluation of the cocaine test in the diagnosis of Horner's syndrome. Arch Ophthalmol 1990;108:384-387. [ Links ]
4. Burde RM, Savino PJ, Trobe JD. Clinical Decisions in Neuro-Ophthalmology. 3rd ed. St Louis: Mosby, 2002: 246-258. [ Links ]
5. Jacobson DM, Berg R, Grinstead GF, Kruse JR. Duration of positive urine for cocaine metabolite after ophthalmic administration: implications for testing patients with suspected Horner syndrome using ophthalmic cocaine. Am J Ophthalmol 2001;131(6):742-747. [ Links ]
6. Donahue SP, Lavin PJ, Digre K. False-negative hydroxyamphetamine (Paredrine) test in acute Horner's syndrome. Am J Ophthalmol 1996;122(6):900-901. [ Links ]
7. Moster ML, Galiani D, Garfinkle W. False negative hydoxyamphetamine test in Horner syndrome caused by acute internal carotid artery dissection. J Neuroophthalmol 2003;23(1):22-23. [ Links ]
8. Bates AT, Chamberlain S, Champion M, et al. Pholedrine: A substitute for hydroxyamphetamine as a diagnostic eyedrop test in Horner's syndrome. J Neurol Neurosurg 1995;58:215-217. [ Links ]
9. Morales J, Brown SM, Abdul-Rahim AS, Crosson CE. Ocular effects of apraclonidine in Horner syndrome. Arch Ophthalmol 2000;118:951-954. [ Links ]
10. Bacal DA, Levy SR. The use of apraclonidine in the diagnosis of Horner syndrome in pediatric patients. Arch Ophthalmol 2004;122:276-279. [ Links ]
11. Brown SM, Aouchiche R, Freedman KA. The utility of 0.5% apraclonidine in the diagnosis of Horner syndrome. Arch Ophthalmol 2003;121:1201-1203. [ Links ]
12. Freedman KA, Brown SM. Topical apraclonidine in the diagnosis of suspected Horner syndrome. J Neuroophthalmol 2005;25:83-85. [ Links ]
13. Koc F, Kavuncu S, Kansu T. The sensitivity and specificity of 0.5% apraclonidine in the diagnosis of oculosympathetic paresis. Br J Ophthalmol 2005;89(11):1442-1444. [ Links ]
14. Bohnsack BL, Parker JW. Positive apraclonidine test within two weeks of onset of Horner syndrome caused by carotid artery dissection. J Neuroophthalmol 2008;28(3):235-236. [ Links ]
15. Chen PL, Hsiao CH, Chen JT, et al. Efficacy of apraclonidine 0.5% in the diagnosis of Horner syndrome in pediatric patients under low or high illumination. Am J Ophthalmol 2006;142(3):469-474. [ Links ]
16. Watts P, Satterfield D, Lim MK. Adverse effects of apraclonidine used in the diagnosis of Horner syndrome in infants. J AAPOS 2007;11(3):282-283. [ Links ]
17. Chen PL, Chen JT, Lu DW. Comparing efficacies of 0.5% apraclonidine with 4% cocaine in the diagnosis of Horner syndrome in pediatric patients. J Ocul Pharmacol Ther 2006;22(3):182-187. [ Links ]
18. Moodley AA, Spooner RB. Apraclonidine in the diagnosis of Horner's syndrome. S Afr Med J 2007; 97(7):506-507. [ Links ]
19. Dewan MA, Harrison AR, Lee MS. False-negative apraclonidine testing in acute Horner syndrome. Can J Ophthalmol 2009;44(1):109-110. [ Links ]
20. The Merck Manuals: Online Medical Library. Apraclonidine. Available at: http://www.merck.com/mmpe/lexicomp/apraclonidine.html (accessed 1 December 2009). [ Links ]
21. Danesh-Meyer HV, Savino P, Sergott R. The correlation of phenylephrine 1% with hydroxyamphetamine 1% in Horner's syndrome. Br J Ophthalmol 2004;88(4):592-593. [ Links ]
22. Falzon K, Jungkim S, Charalampidou S, et al. Denervation supersensitivity to 1% phenylephrine in Horner syndrome can be demonstrated 10 days after the onset of symptoms. Br J Ophthalmol 2009; 93(1):30. [ Links ]
Accepted 7 December 2009.
Corresponding author: D Smit (dpsmit@sun.ac.za)


{kind=link}