










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.100 n.4 Pretoria Apr. 2010
ORIGINAL ARTICLES
Surgical practice in a maximum security prison - unique and perplexing problems
S J A SmitI; F KleinhansII
MB ChB, MMed (Gen Surg). Department of Surgery, University of the Free State, Bloemfontein
BA (Cur). Prison Clinic, Mangaung Maximum Security Prison, Bloemfontein
ABSTRACT
The practice of general surgery in a prison population differs considerably from that in a general surgical practice. We audited surgical consultations at the Mangaung Correctional Centre from December 2003 to April 2009. We found a high incidence of foreign object ingestion and anal pathology.
Understanding the medical and social aspects of prison life facilitates the treatment of inmates with surgical problems.
Prison medicine is not a well-known topic to most doctors. We aimed to provide insight into the unusual surgical (deliberate ingestion of foreign objects, an unusually high rate of anal pathology) and medico-social aspects (motivation for foreign object ingestion, surgical problems associated with homosexuality) prevailing in a prison population. The literature on foreign objects deals largely with the accidental swallowing of household items. Studies on the deliberate ingestion of foreign objects by prisoners are rare,1 and our study differs in aspects such as time to presentation, position and methods of retrieval of foreign bodies.
Patients and methods
The Mangaung Correctional Centre was established in terms of the Correctional Services Act as a Public Private Partnership. The prison is designed for and holds 2 928 male inmates who are all serving long-term sentences for a variety of crimes. The full-time medical staff of the prison comprises 3 general medical practitioners, a nurse manager and 21 registered nurses. Contract service is rendered by a physician, an orthopaedic surgeon, a general surgeon and a urologist. The prison has an infirmary that can accommodate 54 patients.
We audited the surgical consultations between December 2003 and April 2009 by reviewing the weekly statistics that were compiled by the visiting surgeon, and included only these patients. If needed, the clinical records of the individual patients were scrutinised for additional information. The provisional and final diagnoses of 1 112 surgical patients were analysed. Written consent for this study was granted by the Department of Correctional Services.
Results
The incidences of the surgical conditions seen are shown in Table I. The most common conditions were associated with the upper gastro-intestinal tract, including upper abdominal pain, dyspepsia, dysphagia and haematemesis. Upper gastrointestinal endoscopy was warranted in 110 patients and yielded 5% major pathology (ulcers and tumors). The most common minor pathologies among patients were Candida and reflux oesophagitis.
Anal and peri-anal diseases were the second most common conditions encountered. Anal fissures were the most common; peri-anal fistulas, condylomata accuminata and cases of disintegrating perineum syndrome were also seen. Symptomatic haemorrhoids made up a small proportion of consultations and decreased significantly after the banding system replaced operative haemorrhoidectomy.
Around 13% of the patients had skin appendage diseases including sebaceous cysts, ingrown toenails and superficial abscesses, which can be expected in this young male population.
Benign soft-tissue tumours were encountered in less than 10% of patients; the majority were lipomas, and other lesions included fibromas and warts.
Given the country's high HIV prevalence, it is surprising that AIDS-related lymphadenopathy accounted for only 6.2% of surgical consultations. The incidence of HIV positivity in this institution cannot be accurately determined as testing is voluntary. Statistics for 2009 showed an incidence of 33.4%, with 2 019 inmates having been tested.
The miscellaneous group of surgical consultations included trauma, appendicitis, hernias and malignancies such as Kaposi's sarcoma, etc.
Forty-five patients ingested foreign bodies. The deliberate ingestion of foreign bodies appears to be the surgical equivalent of a hunger strike and is used to force the prisoner's will upon the prison authorities as a form of attack against the justice system. Once prisoners become 'institutionalised', they adjust to their circumstances and refrain from this and other disturbing practices.
The local 'record' for an inmate is 24 separate incidents of foreign body ingestion, from December 2005 to January 2009. In our series, there were no fatalities from the ingestion of foreign bodies. The most common objects ingested were radio-opaque, including pieces of wire and screws, tooth brushes and other non-radio-opaque objects. Inmates favour radio-opaque objects because they want proof of their actions. Sometimes, the sharp ends of wires or screws were bent over or covered with plastic before being swallowed (Fig. 1). Swallowing is done as a circus artist swallows a sword. An abdominal X-ray may not give conclusive evidence of the location (presumably intraluminal) of the object (Fig. 2). The weight of the intragastric objects may result in the stomach hanging almost into the left iliac fossa (Fig. 3).



Patients were managed as follows:
Conservative management is often followed, based on the premise that an object that has passed the crico-pharyngeus will eventually be passed rectally. This process usually applies to short (<5 cm) and/or flexible objects (Fig. 4). Surprising objects can traverse the gastro-intestinal tract, with ingested glass, pins, short nails and screws seldom causing problems.

Endoscopic extraction using a 'crocodile' forceps is reserved for cases where the object is still in the oesophagus (Fig. 5) or stomach. Potential problems of endoscopic extraction of foreign bodies include:

• Inability to grasp the foreign object at its very end as a nail or pin cannot go sideways through the oesophagus when grasped in the middle. Changing the patient's position may allow the end of the object to be grasped.
• Multiple ingested objects may be entangled and impossible to remove one at a time (Fig. 1).
• Objects in the duodenum may also be removed endoscopically depending on how far the endoscopist can transverse the duodenum.
• After a difficult extraction by endoscope, chest and abdominal X-rays should be done to exclude covert visceral perforation.
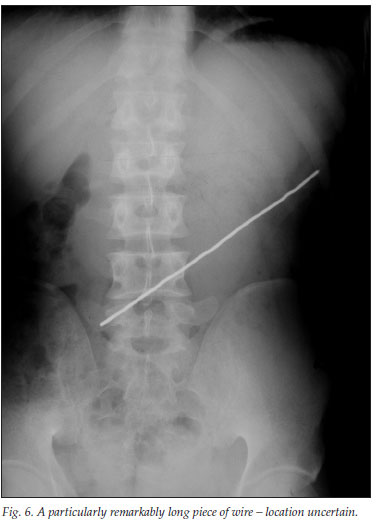
Operative intervention is reserved for specific indications including where the screw or wire that has been ingested is >10 cm in length (Fig. 6). If not removed endoscopically, these objects may transverse the pylorus only to be impeded at the ligament of Treitz owing to the acute duodeno-jejunal angle - which occurred in 3 patients in this series. Perforations may occur gradually without the usual signs of an acute abdomen. Operative intervention is therefore required if exceptionally long pieces of wire cannot be extracted endoscopically or if the foreign body remains impacted at a specific site and the patient develops progressive signs. Midline laparotomies should be avoided; it is preferable to do a small transverse incision where the foreign object has impacted. Multiple midline laparotomies for repeat foreign object ingestions have well-known problems and complications. If warranted, the object should be milked from a more difficult location (e.g. duodenum) to an easier location to expedite its removal. To ensure that all the objects are removed at the end of the procedure, intra-operative X-ray screening is advisable.
Discussion
History taking from long-term prisoners differs in several aspects. Most of them are appreciative of human interaction, especially from an outside source, and tend to provide superfluous histories. Prisoners' perception of time often becomes relative and appears to slow down; events from years ago become intertwined with present events so that histories may become complex and irrelevant.
Aspects of prison medicine that may be foreign to novices in this field of practice are the high incidence of anal pathology, the low yield of pathology in the upper gastro-intestinal endoscopies performed, and the practice of deliberate foreign body ingestion. Although representing a small proportion of the consultations, the deliberate swallowing of foreign objects by inmates remains a troublesome, emotional and timeconsuming clinical situation. Removal of the foreign object requires consideration of each object and site to determine what option is best for that patient.
The high incidence of anal pathology relates to three interrelated components: anal sexual intercourse, the high HIV positivity rate and the use of the rectum to store foreign objects. Homosexual activity occurs among prison inmates;2 heterosexual inmates may also engage in homosexual activities, regarding this as a temporary measure while incarcerated. Condoms are freely available in the prison.
The most common reason for surgical consultation by prisoners is an upper gastro-intestinal complaint; these have an extremely low yield (<5%) of pathologies when endoscopies are performed, which could arguably be partially due to the scarcity of tobacco and alcohol in the prison system. Smoking is allowed but no alcohol consumption is tolerated, although illegal alcohol may be made by fermenting fruit in sunlight. Other positive health-promoting factors may also play a role, and the prisoners' exposure to and participation in sport and gardening may protect against gastro-intestinal pathology.
The authors thank Professor David Stones, whose assistance made this manuscript a readable document.
References
1. Lee TH, Kang YW, Kim SM, et al. Foreign objects in Korean prisoners. Korean J Intern Med 2007; 22(4): 257-258. [ Links ]
2. Sagarin E. Prison homosexuality and its effect on post-prison sexual behavior. Psychiatry 1976; 39(3): 245-257. [ Links ]
Accepted 14 October 2009.
Corresponding author: S Smit (gnchsjas@ufs.ac.za)

