










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.100 no.2 Pretoria Fev. 2010
SAMJ FORUM
CLINICAL IMAGES
Intestinal pseudo-obstruction: the massive abdomen and the red herring
P Naidoo; S Schwartz; S Murphy; R D Mohanlal; H Greeves
A 13-year-old boy presented with a 1-year history of a gradually distending abdomen that was associated with constitutional symptoms, haematemesis and haematochezia that were exacerbated after taking traditional medicament. Admissions for similar episodes when he was 4 and 9 years old had yielded no diagnosis. A previous non-full-thickness rectal biopsy reported nonspecific changes. He was markedly cachexic with a grossly distended abdomen (Fig. 1) that was difficult to palpate. Shifting dullness was elicited and the flanks were dull. There was central hyper-resonance on percussion. Rectal examination was normal.

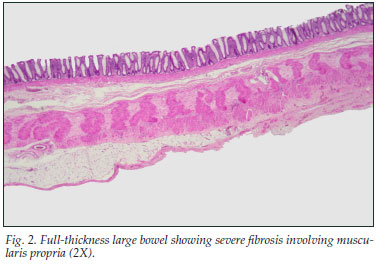
An X-ray of the abdomen revealed a grossly distended large intestine. Ultrasound showed increased ascitic fluid. A total colectomy with an ileostomy was performed. Histological examination of the colon (Fig. 2) was consistent with a diagnosis of hollow viscus myopathy. The patient died after a second laparotomy.
Discussion
Chronic intestinal pseudo-obstruction (CIPO) is a rare, severe syndrome with impaired gastro-intestinal motility leading to functional obstruction resembling mechanical obstruction. It usually affects elderly people with underlying co-morbidities, and early recognition and appropriate management are essential to reduce life-threatening complications.1 The condition may be idiopathic or secondary to other conditions. Most cases are sporadic. Familial forms with either dominant or recessive autosomal inheritance have been described. Histologically, it is classified into neuropathies, mesenchymopathies and myopathies, according to the predominant involvement of enteric neurons, interstitial cells of Cajal or smooth-muscle cells, respectively.2 Hollow visceral myopathy (HVM) is a myopathic cause of CIPO.
HVM is a rare clinical entity characterised by impaired intestinal function and motility secondary to a smooth-muscle defect.3,4 Familial visceral myopathy is the most common type, with an autosomal dominant or recessive inheritance.5 Any part of the gastro-intestinal tract, and occasionally the urinary tract, may be involved. Presenting symptoms may be gastro-intestinal, ranging from abdominal pain and bloating to constipation or diarrhoea; or urological, ranging from recurrent urinary tract infections to urinary retention.4
A previous non-full-thickness biopsy did not identify any pathological changes. However, a full-thickness biopsy after colectomy identified pathology confirming that full-thickness biopsy is superior.6
This case was challenging because of the long duration, presence of constitutional symptoms, recent ingestion of traditional medicament, shifting dullness and dullness in the flanks on clinical examination, previous non-significant rectal biopsy, ascites revealed on ultrasound examination, and unhelpful laboratory investigations.
1. De Giorgio R, Knowles CH. Acute colonic pseudo-obstruction. Br J Surg 2009; 96(3): 229-239. [ Links ]
2. Antonucci A, Fronzoni L, Cogliandro L, et al. Chronic intestinal pseudo-obstruction. World J Gastroenterol 2008; 14(19): 2953-2961. [ Links ]
3. Isaacson C, Wainwright HC, Hamilton DG, et al. Hollow visceral myopathy in black South Africans. A report of 14 cases. S Afr Med J 1985; 67(25): 1015-1017. [ Links ]
4. Ghavamian R, Wilcox DT, Duffy PG, et al. The urological manifestations of hollow visceral myopathy in children. J Urol 1997; 158: 1286-1290. [ Links ]
5. Jones SC, Dixon MF, Lintott DJ, et al. Familial visceral myopathy; a family with involvement of four generations. Dig Dis Sci 1992; 37: 464. [ Links ]
6. Arslan M, Bayraktar Y, Oksuzoglu G, et al. Four cases with chronic intestinal pseudoobstruction due to hollow visceral myopathy. Hepatogastroenterology 1999; 46(25): 349-352. [ Links ]
Drs Naidoo, Schwartz and Murphy work in the Department of Paediatrics; Dr Mohanlal in the Department of Anatomical Pathology; and Dr Greeves in the Department of Paediatric Surgery, University of the Witwatersrand, Johannesburg.
Corresponding author: P Naidoo (barrys@nicd.ac.za)

