










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.100 n.1 Pretoria Jan. 2010
SAMJ FORUM
CLINICAL IMAGES
G S IsaacsI; B SinghII,*
IMB ChB (Stellenbosch), was doing his internship at King Edward VIII Hospital, Durban, at the time of this submission
IIFCS (SA), MD, is a consultant surgeon at the same hospital
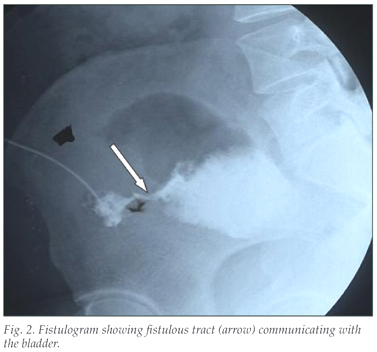
A 14-year-old girl presented with a 4-year history of a clear, intermittent discharge oozing from the umbilicus (Fig. 1), which was confirmed to be urine on biochemical evaluation. A fistulogram demonstrated a tract communicating the umbilicus with the bladder (Fig. 2), consistent with a urachal fistula, which was successfully resected surgically.

The intra-embryonic cloaca, destined to become the bladder, is connected to the extra-embryonic allantois derived from the caudal end of the yolk sac through the urachus. During normal development the urachus obliterates to form the median umbilical ligament at around 32 weeks' gestation. Incomplete closure of this embryological communication may result in a urachal fistula, urachal sinus, urachal cyst or urachal diverticulum (Fig. 3).1, 2 A urachal fisutula, as in the above case, results from failure of the urachus to atrophy completely. Failure of the umbilical and the bladder ends of the urachus to obliterate results in development of urachal sinus and bladder diverticulum, respectively. Patency of a segment of the urachus along its extent may result in a urachal cyst.
Urachal fistula is the commonest of urachal anomalies (48% of cases), followed by urachal cyst (31%). Urachal remnant disorders are rare, occurring in less than 2% of adults, with a 2:1 male/female ratio. Patients usually present with nonspecific abdominal or urinary tract signs and symptoms such as pain and retraction of the umbilicus during micturition. However, patients with urachal cysts may present with severe infection or a tender midline infra-umbilical mass. A purulent umbilical or frankly urinary discharge may be associated with a urachal sinus or fistula, respectively.3 Typically urachal fistulas present between 6 weeks and 6 years of age. Urachal cysts are usually undetected during childhood and may become clinically evident as a tender mass when infected. The otherwise asymptomatic urachal diverticulum may be associated with calculus formation and urinary tract infection.
Ultrasonography, computed tomography, a fistulogram or a cysto-urethrogram may be used to make the definitive diagnosis. Distal obstruction to the urinary tract must be excluded in patients with a urachal fistula.
Anomalies associated with urachal remnants such as vesico-ureteral reflux, meatal stenosis, hypospadias, umbilical and inguinal hernias, cryptorchidism, anal atresia, omphalocele and crossed renal ectopia are rare, but should also be considered.
Treatment begins with intravenous antibiotics followed by complete excision of the urachal remnant, including a cuff of the bladder, which may be undertaken laparoscopically, when there is communication with the bladder.
1. Choi YJ, Kim JM, Ahn SY, Oh J-T, Han SW, Lee JS. Urachal anomalies in children: a single center experience. Yonsei Med J 2006; 47(6): 782-786. [ Links ]
2. Carlisle EM, Mezhir JJ, Glynn L, Liu CD, Slatter MB. The umbilical mass. Pediatr Surg Int 2007; 23(8): 821-824. [ Links ]
3. Ward TT, Saltzman E, Chiang S. Infected urachal remnants in the adult: case report and review. Clin Infect Dis 1993; 16: 26-29. [ Links ]
* Corresponding author: B Singh (singhb3@ukzn.ac.za)

