










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.99 n.8 Pretoria Aug. 2009
ORIGINAL ARTICLES
Fifty years of thoracic surgical research in South Africa
A LinegarI, *; F SmitII; P GoldstrawIII; G van ZylIV
IMB ChB, FC (Cardio) SA, PhD, Department of Cardiothoracic Surgery, University of the Free State, Bloemfontein
IIMB ChB, MMed (Cardiothor), Department of Cardiothoracic Surgery, University of the Free State, Bloemfontein
IIIFRCS, Imperial College and Royal Brompton Hospital, London
IVMFamMed, MBA, PhD, Medical School, University of the Free State
ABSTRACT
AIM: To investigate the scope and trends in clinical research in South African thoracic surgery between 1955 and 2006 and to measure its impact on clinical practice.
METHOD: A systematic review of all SA thoracic surgical publications was performed.
RESULTS: There were 252 general thoracic publications and a marked decrease in publications was noted after the peak period of productivity of the 1980s. There was a shift toward the private sector as an origin of articles and toward a local, non-indexed journal. Inflammatory lung disease was the most frequent topic of publication. Case series and case reports were the most frequent type of article.
CONCLUSION: The vulnerability of a small specialty in a developing country is illustrated by the clear trends that
emerged. The study provides important indicators for future research, highlights the need for a national database of clinical experience, and emphasises the importance of rekindling interest and a culture of research in thoracic surgery.
We aimed to investigate the scope and trends in clinical research in South African thoracic surgery between 1955 and 2006 and to measure its impact on clinical practice. The vulnerability of a small specialty in a developing country is illustrated by the clear trends that emerged. The study provides important indicators for future research, highlights the need for a national database of clinical experience, and emphasises the importance of rekindling interest and a culture of research in thoracic surgery.
Method
An electronic search was performed of Medline via Pubmed, The Africa-Wide:NiPad database of African and South African publications (Africa-Wide:NiPad) and the Cochrane Libraries of systematic reviews and clinical trials and a manual search was done of the SA Respiratory Journal, SA Radiology Journal (previously Imaging SA), Cardiovascular Journal of SA and SA Heart Journal.
The search covered 52 years between January 1955 and December 2006. It was performed using the names of specialist surgeons who have practised cardiothoracic surgery in South Africa (SA), universities in SA that have departments of cardiothoracic surgery, academic teaching hospitals, cities in which the university teaching units are found, and the word 'cardiothoracic'.
Articles that originated in SA and that reported on SA patients in medical journals were included. Congress abstracts, textbooks and chapters in textbooks were not included.
Research quality was evaluated using the Oxford Centre for Evidence-based Medicine levels of evidence.1 Journals in which the articles were published were listed according to their citation impact factor.2
Results
Eight hundred and sixty-three cardiothoracic publications were produced by the 169 surgeons who worked in SA during the 52-year period between 1955 and 2006.
No publications were found in the Cochrane clinical trials or Cochrane systematic review libraries (Fig. 1).
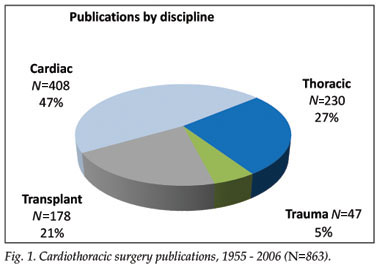
General thoracic surgical publications totalled 252, including 22 non-cardiac trauma publications.
Publication trends
The quantitative trend in thoracic publications is shown in Fig. 2. Peak productivity occurred between 1980 and 1989, with a total of 99 (9.9 publications per year). The mean annual publication rate over the 52 years was 4.8 for thoracic publications (standard deviation (SD) 4.0), compared with 11.2 publications per year for the combined cardiac and transplantation literature.

University publications decreased markedly after the 1980s, with a shift towards the private sector. The private sector provided 14% of the national output after 1995 and 20% after 2000, placing it third in the rankings of publications after the University of Cape Town (31) and the University of KwaZulu-Natal (11) since 1995.
Journals
The publications appeared in 56 journals, and the most frequently used are shown in Table I. The South African Medical Journal (S Afr Med J) published most publications (35%) up to 1995. After 1995, a shift toward the non-indexed SA Respiratory Journal (SA Resp J) occurred, accounting for 30% of all articles and 41% of publications with a thoracic surgeon as first author. The citation index rating in Table I reveals that 50% of the publications appeared in journals with a rating of less than 2.

Patient numbers
A total of 7 481 patients were discussed in 193 clinical publications over the 52-year period. The largest series of patients were in 2 papers, one on penetrating thoracic injuries in 1 000 patients3 and the other on 896 pneumonectomies.4
Topics of publication
Pleuro-pulmonary disease (N=147), specifically inflammatory disease (N=72), was the most frequent topic of publication (inflammatory disease accounted for 37% of the 193 clinical publications). Oesophageal disease accounted for 17% of publications, airway pathology for 8%, pericardial disease for 4%, mediastinal masses for 3%, chest wall tumours for 3%, conditions of the diaphragm for 1% and the chyle duct for 0.5%. Ten papers on empyema collectively reported on 465 patients. None reported on the management of the very common problem of persistent pleural spaces in chronic empyema with or without broncho-pleural fistula.
The influence of the human immunodeficiency virus (HIV) on thoracic surgical patients was discussed in 2 papers, one on chronic lung disease in 194 patients5 and the other on issues confronting the surgeon treating HIV-infected patients.6
Twenty articles reported on 798 patients with carcinoma of the bronchus: 9 were surgical in focus (558 patients), while 6 dealt with chemotherapy and/or radiotherapy in lung cancer. Multimodality therapy in advanced disease was reviewed in 2 papers, one of which dealt with the importance of staging and survival after complete resection in patients with or without N2 disease.7 Thoracic surgeons were first authors in 11 papers on bronchial carcinoma (55%).
There were 19 papers on oesophageal carcinoma, reporting on 678 patients in total. Articles discussing palliation of dysphagia accounted for most of these, and there were also 4 scientific studies, 1 investigating the role of the human papillomavirus and 3 chromosomal changes in oesophageal carcinoma.
There were 47 trauma publications from cardiothoracic surgeons, 22 (1 133 patients) discussing non-cardiac and non-great vessel trauma. Penetrating trauma was the most common topic.
Study design
Clinical observations in thoracic surgery were reported in 193 (77%) of all publications: 2 randomised controlled trials (RCTs), 6 cohort studies, 87 descriptive series reviews, 94 case reports and 4 letters. There were no systematic reviews or meta-analyses (Table II).
One RCT comparing cefoxitin with cephalothin in 19 patients treated for chronic destructive pneumonia8 had a thoracic surgeon as first author. The other RCT, investigating etoposide scheduling in the treatment of small-cell lung carcinoma in a series of 78 patients,9 had a surgeon as a co-author.
Of the 6 cohort studies, 5 were retrospective and 1 was prospective. One retrospectively compared the survival of pleuro-pneumonectomy with parietal pleurectomy in mesothelioma.10 A second compared surgical with medical management of childhood bronchiectasis.11 Goldstraw and Bach12 compared gastric emptying after oesophagectomy with normal controls. Goldstraw13 also examined the influence of pleural irrigation and antibiotics on the incidence of post-pneumonectomy empyema. A 5th study compared postoperative 5-year survival between groups of patients with microscopic pN2 disease and those with less advanced nodal staging in non-small-cell lung cancer.7 A non-randomised prospective study reported on the effect of normovolaemic haemodilution in 10 patients before thoracic surgery.14
Of the 252 publications, 189 (75%) had a thoracic surgeon as first author, of which 141 reported clinical data in case reports or patient series. These 141 papers were assessed on the Oxford Centre for Evidence-based Medicine model for levels of evidence1 (Table II), and 5% of papers with a thoracic surgeon as first author were rated grade B. Statistical analysis in the reports on patient series was almost exclusively by simple proportions.
Discussion
The overall number of publications (252), and especially the number of publications with a thoracic surgeon as first author (189), is low relative to the size of the SA population, the burden of thoracic disease and the number of surgeons who practised cardiothoracic surgery over the 50-year period (169).15 The overall mean output per university is low at 0.6 publications per year; 5 of the 8 university departments of cardiothoracic surgery in SA collectively published only 22 (9%) thoracic surgery articles (Fig. 2). Similar reviews could not be found for comparison with other countries, or with other specialist disciplines in SA.
The most obvious trends from this analysis are the decrease in publications and the shift to a non-indexed journal for publication since the 1980s. It is not surprising that inflammatory pleuro-pulmonary disease is the most frequent topic of publication, as it represents the bulk of admissions to thoracic surgical wards in SA. However, this literature does not address the complex, frequent and most debilitating problem of persistent pleural spaces in chronic empyema with or without bronchopleural fistulas. Moreover, tuberculosis and HIV are poorly represented in the SA thoracic surgical literature in spite of their high incidence in our communities.
Considering their burden of disease, there are few publications on lung and oesophageal cancer. The few trauma publications may be explained by trauma units increasingly managing chest trauma, with few cases being referred to cardiothoracic surgeons.
The SA thoracic surgical literature is almost entirely observational in design. There are no RCTs investigating surgical topics, and no systematic reviews or meta-analyses. This is not necessarily a major criticism as most of the international thoracic surgery literature is observational with few published RCTs.
In the opinion of some, the emphasis on observational studies has devalued surgical research.16 Of 119 RCTs published in three major cardiothoracic journals in 1989 and 1999, only 6 were thoracic surgical.17 Problems inherent in conducting RCTs in cardiothoracic surgery were illustrated; in only 15% could recommendations be made for practice change. The authors concluded that, comparative analyses of large series could possibly provide stronger evidence for clinical recommendations. Based on the grades of recommendation in Table II, few SA publications appear to be able to influence clinical practice.
Explaining the decrease in research activity in thoracic surgery in SA since the mid-1980s requires understanding of a complex interplay of many factors. The loss of surgeons with an interest in thoracic surgery from academic practice to emigration, retirement and private practice is significant. At the end of 2006 an estimated 31% (34/109) of clinically active SA cardiothoracic surgeons were working abroad,15 similar to Health Systems Trust 2006 statistics showing that 37% of SA-trained medical doctors were working abroad.18
Rapid private practice development in the 1980s has provided highly accessible clinical services for approximately 7 million of the 47 million people in SA. Private practice has become increasingly attractive to health care professionals owing to the wide differential in income and general working conditions between state and private practice.15,18
Investigating the factors responsible for the critical shortage of general surgeons in SA,19, 20 the Association of Surgeons of SA (ASSA) concluded that the remuneration of state specialist surgeons lagged far behind other state professions such as engineers, judges, magistrates, municipal managers and airline pilots. Salaries also compared poorly with surgical counterparts in the UK, Australia, New Zealand and the SA private sector. Poor remuneration was a main cause of the diminishing interest in general surgery as a career and particularly as an academic pursuit. These conclusions apply equally to thoracic surgery in SA, where many cardiothoracic surgeons and trainees hold the view that an academic career has become unattractive.15 Furthermore, most cardiothoracic surgeons in SA are more interested in cardiac than thoracic surgery as a career. At the end of 2006, SA had 8 surgeons practising thoracic surgery exclusively;15 since 2006, 1 has retired, 1 has died, 1 has emigrated, and 2 might retire within the next 5 years.
Finally, health care reform policy since 1994 has reduced state funding of tertiary medicine, resulting in far fewer referrals and operations performed in teaching departments.15 Professor W van der Merwe, in an address to the Free State Branch of the South African Medical Association on 28 May 2008, reported that 31% of consultant posts in SA tertiary level training hospitals are unfilled and remain frozen by the state This understaffing of academic departments at all levels diminishes the ability to sustain many important departmental functions, the most vulnerable of which is research.
References
1. Phillips B, Ball C, Sackett D, et al. Oxford Centre for Evidence-based Medicine Levels of Evidence. Oxford Centre for Evidence-based Medicine, 2007. URL:http://www.cebm.net (accessed 14 February 2009). [ Links ]
2. Thomson Reuter. ISI Web of Science, Journal Citation Reports. 2007. http://thomsonreuters.com (accessed 29 September 2008). [ Links ]
3. Von Oppell UO, Bautz P, De Groot M. Penetrating thoracic injuries: what we have learnt? Thorac Cardiovasc Surg 2000; 48: 55-61. [ Links ]
4. Shama DM, Odell JA. Esophagopleural fistula after pneumonectomy for inflammatory disease. J Thorac Cardiovasc Surg 1985; 89: 77-81. [ Links ]
5. Jeena PM, Coovadia HM, Thula SA, Blythe D, Buckels NJ, Chetty R. Persistent and chronic lung disease in HIV-1 infected and uninfected African children. AIDS 1998; 12: 1185-1193. [ Links ]
6. De Groot KM. HIV and the thoracic surgeon. SA Respiratory Journal 1985; 3: 143-145. [ Links ]
7. Linegar AG. The importance of staging in non-small cell lung cancer. SA Respiratory Journal 2001; 7: 144-148. [ Links ]
8. le Roux BT, Cameron E, Whitton ID, Williams MA. Cefoxitin sodium in the management of destructive suppurative pneumonia. J Antimicrob Chemother 1978; 4: 251-253. [ Links ]
9. Abratt RP, Willcox PA, de Groot M, Goodman HT, Jansen ER, Salton DG. Prospective study of etoposide scheduling in combination chemotherapy for limited disease small cell lung carcinoma. Eur J Cancer 1991; 27: 28-30. [ Links ]
10. de Vries WJ, Long M. Treatment of mesothelioma in Bloemfontein, South Africa. Eur J Cardiothorac Surg 2003; 24: 434-440. [ Links ]
11. Lee DJ, Conlan AA. Bronchiectasis in urban black children. S Afr Med J 1985; 67: 817-819. [ Links ]
12. Goldstraw P, Bach P. Gastric emptying after oesophagectomy as assessed by plasma paracetamol concentrations. Thorax 1981; 36: 493-496. [ Links ]
13. Goldstraw P. Prophylaxis of post-pneumonectomy empyema. Thorax 1980; 35: 107-109. [ Links ]
14. Moyes DG, Mistry BD, Conlan AA. Normovolaemic haemodilution using dextran 70 in thoracic surgery. S Afr Med J 1985; 67: 762-764. [ Links ]
15. Linegar A. 2009. A model for the development of thoracic surgery in central SA. PhD thesis, Department of Cardiothoracic Surgery, Faculty of Health Sciences, University of the Free State. [ Links ]
16. Horton R. Surgical research or comic opera: questions, but few answers. Lancet 1996; 347: 984-985. [ Links ]
17. Anyanwu AC, Treasure T. Surgical research revisited: clinical trials in the cardiothoracic surgical literature. Eur J Cardiothorac Surg 2004; 25: 299-303. [ Links ]
18. Day C, Gray A. Health and related indicators. In: Ijumba P, Padarath A, eds. South African Health Review 2006. Durban: Health Systems Trust, 2006. http://www.hst.org.za/generic/29 (accessed 3 March 2009). [ Links ]
19. Kahn D, Pillay S, Veller MG, Panieri E, Westcott MJR. General Surgery in crisis – factors that impact on a career in general surgery. S Afr J Surg 2006; 44: 108-112. [ Links ]
20. Kahn D, Pillay S, Veller MG, Panieri E, Westcott MJR. General Surgery in crisis – comparatively low levels of remuneration. S Afr J Surg 2006; 44: 96-107. [ Links ]
Accepted 26 May 2009.
* Corresponding author: A Linegar (al@thoracicsurgery.co.za)

