










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 no.12 Pretoria Dez. 2008
ORIGINAL ARTICLES
Performance data of screening mammography at a dedicated breast health centre
J P ApffelstaedtI; V SteenkampII; K BaatjesIII
IMMed (Chir), FCS (SA). Department of Surgery, Stellenbosch University, W Cape
IIMMed (Chir), FCS (SA). Department of Surgery, Stellenbosch University, W Cape
IIIMB ChB. Panorama, W Cape
ABSTRACT
BACKGROUND: Mammographic screening has become part of routine health care. We present a first analysis of screening mammography in a dedicated breast health centre in Africa.
OBJECTIVE: To establish a performance benchmark and provide data for health care policy and funding decisions on screening mammography.Method. All mammography performed between January 2003 and August 2008 was entered into a prospective database. Mammography was performed exclusively by certified mammographers and double-read by experienced readers.
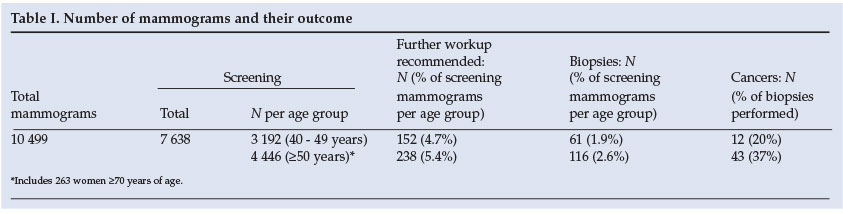
RESULTS: Outcomes were classified in a simplified classification system based on the Breast Imaging Reporting and Data System (BIRADS). In 40 - 49-year-old women, 3 192 mammograms led to a recall rate of 4.7%, a biopsy rate of 1.9% and a cancer diagnosis rate of 3.8 per 1 000 examinations; for women of 50 years and older, the corresponding figures were 4 446, 5.4%, 2.6% and 9.7 per 1 000. Of the cancers detected, 31% were in situ and, of the invasive cancers, 81% were node-negative. These figures were established by a dedicated surgeon-led team and fall within the range expected in organised screening programmes in resource-rich environments, providing a first benchmark for screening mammography in Africa.
In Western societies, mammographic screening is part of routine health care and has been instrumental in reducing the mortality of this dreaded disease.1 An editorial by Dent and Panieri 2 reflected on screening mammography and elicited lively debate. In our opinion, they missed the point, as it was based on a re-assessment of data gathered over 20 years ago with obsolete technology - data that had been gathered in populations that might have had markedly different prevalence and incidence patterns from South African populations. Furthermore, the background of a resource-restricted country has an influence on the interpretation of screening data. A database search yielded not a single publication detailing results of screening mammography in Africa, indicating a crucial lack of data for this important health care topic from the continent. Cognisant of these limitations, we present a first analysis of screening mammography in a dedicated breast health centre in Africa, establishing a performance benchmark and providing data to expedite health care policy and funding decisions.
Methods
All mammograms performed between January 2003 and August 2008 at a dedicated breast centre were entered into a prospective database, with permission of the patients. Mammography was performed exclusively by certified mammographers on state-of-the-art equipment, initially film-screen and, from July 2006, full-field digital equipment (GE Healthcare, Chalfont St Giles, UK). Double reading by experienced readers was performed with consensus after the second reading. Readers were practising clinicians with a special interest in breast health, or certified mammographers who had completed an internationally recognised course in mammography interpretation, had read at least 2 000 mammograms annually, and had a minimum of 50 hours annually of continued professional development in clinico-pathological and imaging correlation in breast health.
Data recorded were: age and gender, indications for mammography and outcomes. Indications for screening mammography as published by the American Cancer Society3 were adhered to. Outcomes were classified in a simplified classification system based on the Breast Imaging Reporting and Data System (BIRADS).4 BIRADS categories 3 and 4 were combined as indeterminate; patients with these lesions were either asked to return for further imaging examinations and a short-term follow-up examination, or a tissue sample was obtained for pathological examination. Patients not returning for follow-up examination were contacted telephonically to ensure compliance. All lesions categorised as BIRADS 5 underwent tissue acquisition for histopathological testing.
Data were entered into and analysed with a commercially available software package (MS Office XP Pro, Microsoft Corporation, Washington, USA).
Results
The number of mammograms and their outcome is shown in Table I.
The analysis of screening performance indicators is shown in Table II.
Discussion
Breast cancer screening in women is well researched, with well-known early studies and later in-service experience establishing the benefits of mammographic screening in defined populations.1 As a result, performance benchmarks have been established; any screening should adhere to these to minimise the harm resulting from increased anxiety, false-positive results and increased cost.5,6 If benchmarking for screening is undertaken, the prevalence and incidence of the screened condition in the population should ideally be known; however, in many resource-limited countries, this is not the case. In South Africa, the accuracy of figures in the National Cancer Registry reports for different population groups has been questioned. Available data indicate that the breast cancer incidence in whites is comparable with that of England; in other population groups, the incidence is much lower but still comparable with other countries that have instituted a population screening programme, such as Singapore7 (except for black population groups). Applying the National Cancer Registry data is problematic as they do not stratify for socioeconomic factors, and racial classification may be construed as offensive and may not measure what it is intended to.8 In patients who present for screening, socio-economic factors may play a more important role than race and ethnicity. Socio-economic status as expressed by voluntary participants in screening correlates well with breast cancer risk.9
The availability of the service attracts individuals who wish to be screened. Consequently, most examinations at our centre are screening examinations. In opportunistic screening, less emphasis is placed on quality controls than on organised screening programmes.10
A decade-long effort to improve the mammographic quality in Michigan11 illustrates that, even in a litigious environment like the USA, the mere presence of a mammographic service does not guarantee quality levels sufficient for effective screening. Consequently, complex mechanisms have been established to ensure mammographic quality in the USA,12 the European Union13 and Australia.14 In a resource-restricted environment such as South Africa, it is unrealistic to contemplate the establishment and maintenance of such complex components of societal infrastructure. A simplified system of quality control would be more appropriate to ensure that scarce resources are employed effectively and based on the principal outcome measures of efficacy and safety. Table III details these outcome measures and how the present series compares with international standards.
The caseload/quality relationship is well documented in mammography, with specialised readers with caseloads of more than 2 000 mammograms per year working in dedicated breast units, detecting more cancers and generating less false-positives than general readers.
Africa, in common with much of the developing world, has a lamentable shortage of radiologists and educational resources, specifically in mammography.19 Evidence from large series examining the interpretation of mammograms by radiographers in Canada, the Netherlands and England indicates that radiographers in screening programmes can read mammograms 'at least as well as' radiologists. Surgeons also can read mammograms as accurately as radiologists.20 This is further supported by data on interventional diagnostics which demand an accurate understanding of breast imaging; in the USA, about a quarter of all stereotactic biopsies are performed by surgeons, and surgeons perform ultrasound-guided biopsies with results comparable to those of radiologists.21-25 Indeed, performance of these interventions by surgeons was found to be less inconvenient and more cost-effective.23 In Germany, gynaecologists and radiologists read mammograms. For the series that we analysed, mammography reading was conducted entirely by surgeons and mammographers dedicated to breast health management. The results achieved not only compare favourably with those achieved in community screening series worldwide,26 but also are similar to results achieved in high-quality organised screening programmes in resource-rich environments, and are within 'the desirable range recommended for highly skilled radiologists' in the USA.5 While this in itself does not confirm the cost-effectiveness of mammographic screening in a resource-restricted environment, it indicates that, in the community screened in this series, cancer detection rates are well within the rage of environments where mammographic screening is a recognised health intervention. It further confirms the importance of dedication to breast health and stringent quality control at all levels of the diagnostic process in the achievement of good outcomes in breast cancer screening over professional qualifications of the professionals involved. We hope that other professionals in the screening arena in South Africa will join us in our quest to provide breast health services of the highest quality to the women of our country. A crucial step in this is to publish screening performance data, as given above, to establish the effectiveness of their service to the public, funders and health authorities. Mammographic screening should be restricted to institutions that provide evidence of effective screening to ensure optimal application of scarce resources.
The authors thank Ms Karlien La Douce, Ms Norah Mabota and Ms Jolanta Mlodawski for the excellent mammography, which formed the basis of this paper, that they provided.
References
1. Dixon JM. Screening for breast cancer. BMJ 2006; 332(7540): 499-500. [ Links ]
2. Dent DM, Panieri E. Screening for breast cancer - finding a place between common sense and the evidence base. S Afr Med J 2004; 94(5): 354-355. [ Links ]
3. American Cancer Society. Can breast cancer be detected early? http://www.cancer.org (accessed 8 Aug 2008). [ Links ]
4. American College of Radiology. ACR Breast Imaging Reporting and Data System. 4th ed. Reston, VA, USA: American College of Radiology, 2003. [ Links ]
5. Rosenberg RD, Yankaskas BC, Abraham LA, et al. Performance benchmarks for screening mammography. Radiology 2006; 241(1): 55-66. [ Links ]
6. Smith RA, Duffy SW, Gabe R, Tabar L, Yen AMF, Chen THH. The randomized trials of breast cancer screening: what have we learned? Radiol Clin North Am 2004; 42(5): 793. [ Links ]
7. Tan PH. Breast screening in Singapore: implications for pathology. Ann Acad Med Singapore 2007; 36(10): 827-833. [ Links ]
8. Ncayiyana DJ. Racial profiling in medical research: what are we measuring? S Afr Med J 2007; 97(12): 1225-1226. [ Links ]
9. Chia KS, Reilly M, Tan CS, et al. Profound changes in breast cancer incidence may reflect changes into a Westernized lifestyle: a comparative population-based study in Singapore and Sweden. Int J Cancer 2005; 113(2): 302-306. [ Links ]
10. Miles A, Cockburn J, Smith RA, Wardle J. A perspective from countries using organized screening programs. Cancer 2004; 101(5 Suppl): 1201-1213. [ Links ]
11. Osuch JR, Camburn JF, Sienko DG, Potchen EJ. The history and the effect of the mammography quality assurance legislation in Michigan. Cancer 1994;74(1 Suppl): 263-270. [ Links ]
12. Monsees BS. The Mammography Quality Standards Act: An overview of the regulations and guidance. Radiol Clin North Am 2000; 38: 759-772. [ Links ]
13. Perry N, Broeders M, de Wolf C, et al. European Guidelines for Quality Assurance in Breast Cancer Screening and Diagnosis. 4th ed. Luxembourg: Office for Official Publications of the European Communities, 2006. [ Links ]
14. Giles GG, Amos A. Evaluation of the organised mammographic screening programme in Australia. Ann Oncol 2003; 14(8): 1209-1211. [ Links ]
15. NHS Breast Screening Programme and Associations of Breast Surgeons at BASO. An Audit of Screen Detected Breast Cancers for the Year of Screening April 2006 to March 2007. Birmingham, UK: West Midlands Cancer Intelligence Unit, 2008. [ Links ]
16. The Information Centre. 2006-2007 Breast Screening Tables. Government Statistical Service. Sheffield, UK: NHS. [ Links ]
17. BreastScreen Australia Monitoring Report 2004-2005. 2008 ed. Canberra: Australian Institute of Health and Welfare, 2008. [ Links ]
18. Tan PH, Chiang GS, Ng EH, Low SC, Ng FC. Screen detected breast cancer in an Asian population: pathological findings of the Singapore breast screening project. Breast 1999; 8(3): 120-125. [ Links ]
19. Rabinowitz DA, Pretorius ES. Postgraduate radiology training in sub-Saharan Africa: a review of current educational resources. Acad Radiol 2005; 12(2):224-231. [ Links ]
20. Vidya R, Dixon JM. Should surgeons as well as radiologists report mammograms in symptomatic patients? Breast 2001; 10(2): 140-142. [ Links ]
21. Burns RP, Brown JP, Roe SM, Sprouse LR, Yancey AE, Witherspoon LE. Stereotactic core-needle breast biopsy by surgeons: minimum 2-year follow-up of benign lesions. Ann Surg 2000; 232(4): 542-548. [ Links ]
22. Dowlatshahi K, Snider H, Lerner AG. Who should perform image-guided breast biopsy and treatment? Am J Surg 2007; 194(3): 275-277. [ Links ]
23. Roe SM, Mathews JA, Burns RP, Sumida MP, Craft P Jr, Greer MS. Stereotactic and ultrasound core needle breast biopsy performed by surgeons. Am J Surg 1997; 174(6): 699-703. [ Links ]
24. Staren ED. Ultrasound-guided biopsy of nonpalpable breast masses by surgeons. Ann Surg Oncol 1996; 3(5): 476-482. [ Links ]
25. Stolier AJ. Stereotactic breast biopsy: a surgical series. J Am Coll Surg 1997; 185(3): 224-228. [ Links ]
26. Elmore JG, Nakano CY, Koepsell TD, Desnick LM, D'Orsi CJ, Ransohoff DF. International variation in screening mammography interpretations in community-based programs. J Natl Cancer Inst 2003; 95(18): 1384-1393. [ Links ]
 Correspondence:
Correspondence:
J Apffelstaedt
(jpa@sun.ac.za)
Accepted 7 October 2008.


{kind=link}
{kind=link}
{kind=link}