










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 n.11 Pretoria Nov. 2008
ORIGINAL ARTICLES
Fetal alcohol syndrome among Grade 1 schoolchildren in Northern Cape Province: Prevalence and risk factors
Michael UrbanI; Matthew F ChersichII; Leigh-Anne FourieIII; Candice ChettyIV; Leana OlivierV; Denis ViljoenVI
IMB BCh, FCP (SA), Cert (Med Genet). Division of Human Genetics, University of Cape Town
IIMB BCh, PhD. International Centre for Reproductive Health, Kenya, and University of Ghent, Belgium
IIIMDiac, BA Hons. Foundation for Alcohol Related Research (FARR), Johannesburg
IVMA, BSc Hons. Foundation for Alcohol Related Research (FARR), Johannesburg
VBCur, BSocSc, BA Hons. Foundation for Alcohol Related Research (FARR), Cape Town
VIMB ChB, FCP, MD, DCH. Foundation for Alcohol Related Research (FARR), Cape Town
ABSTRACT
OBJECTIVE: To describe the prevalence, characteristics and risk factors for fetal alcohol syndrome (FAS) and partial FAS among schoolgoing children in Grade 1 in Northern Cape Province, South Africa.
DESIGN: A cross-sectional study using a two-tiered method for ascertainment of FAS/partial FAS cases, comprising: screening of growth parameters, diagnostic assessment for screen-positive children using clinical and neurocognitive assessments, and maternal history of drinking during pregnancy. Mothers or caregivers of FAS children and matched controls were interviewed.
SETTING: Primary schools in De Aar (8) and Upington (15).
SUBJECTS: Grade 1 pupils in 2001 (De Aar, N=536) and 2002 (Upington, N=1 299).
OUTCOME MEASURES: FAS or partial FAS.
RESULTS: The prevalence of FAS/partial FAS was high: 64/536 (119.4/1 000, 95% CI 93.2 - 149.9) in De Aar, and 97/1 299 (74.7/1 000, 95% CI 61.0 - 90.3) in Upington. Overall, 67.2 per 1 000 children (95% CI 56.2 - 79.7) had full FAS features.
Growth retardation was also common in this population: 66.6% (1 181/1 774) were underweight, 48.3% (858/1 776) stunted, and 15.1% had a head circumference <2 SD for age. Mothers of children with FAS were less likely to have full-time employment or have attended secondary school and had lower body mass index, and about 80% currently smoked. Over two-thirds of all pregnancies had been unplanned.
CONCLUSIONS: A very high proportion of pupils (nearly 1 in 10) had FAS/partial FAS, the rate in De Aar being the highest yet described in South Africa. FAS/partial FAS may contribute to the extremely high rate of growth retardation in South Africa as a whole and is a major cause of learning disability. These epidemiological features are important in designing preventive interventions.
Fetal alcohol syndrome (FAS) was described as an entity in 1973.1 It is the severe end of a spectrum of deleterious effects caused by prenatal exposure to alcohol, including some or all of the following features: facial dysmorphism, prenatal and/or postnatal growth retardation, and neurological, cognitive and behavioural abnormalities. The term 'fetal alcohol spectrum disorder' describes the effects that can occur in an individual who is prenatally exposed to alcohol, encompassing FAS, partial FAS (PFAS) and other adverse outcomes.2 Our study focuses on FAS and PFAS because dysmorphic features make them more specific and recognisable diagnoses.
FAS/PFAS is among the most common causes of learning disability worldwide, but especially high rates have been described in parts of South Africa. Whereas the average prevalence of FAS in high-income countries has been estimated at 0.97/1 000,3 rates reported from Wellington, Western Cape Province, have ranged between 40.5 and 54 per 1 000.4,5
The reasons for South Africa's high FAS burden are incompletely understood, and relate to risky maternal alcohol consumption and other maternal personal, social and perhaps genetic factors that increase the risk of FAS. The answers are necessarily multifaceted. Regular binge-drinking (heavy episodic drinking of 5 or more units of alcohol per occasion) is the most risky drinking pattern for FAS.6 High rates of binge-drinking were found among women attending antenatal clinics in the Western Cape.7 The dop system (alcohol forming part of labourers' wages on wine farms) is believed to have played a role in entrenching binge-drinking.
Maternal factors also linked to increased risk of having a child with FAS include: older age at pregnancy, smoking and low socio-economic status;3,5,8-10 the latter may be a blanket term for numerous poorly defined factors including psychological depression, unintended pregnancies and poor nutrition that provoke, or interact with, alcohol consumption to exacerbate the effects of high-risk drinking patterns.
We aimed to describe and investigate the prevalence of and risk factors for FAS and PFAS in Grade 1 children in De Aar and Upington, two large towns in Northern Cape Province.
Methods
The study took place from 2001 to 2004, using the identical methods in De Aar and Upington. Upington is a centre of the viticulture industry on the banks of the Orange River. De Aar is in a sheep-farming area in the Upper Karoo region. Eight schools in De Aar and 15 in Upington participated. Permission for the study was obtained from the Northern Cape Department of Education. All Grade 1 pupils at these schools in 2001 (in De Aar) and in 2002 (in Upington) were enrolled if parents or legal guardians consented. Since primary school attendance is compulsory, it was anticipated that most children in the community would be reached. The study was approved by the University of the Witwatersrand Committee for Research on Human Subjects (M00/11/14).
The prevalence of FAS was determined by active case ascertainment using a two-tier screening method:4 an initial screening stage followed by a comprehensive diagnostic stage (clinical evaluation, neurocognitive assessment and maternal interview). Identified FAS or PFAS cases were matched with controls.
Stage one: screening
Study nurses obtained anthropometric measurements. Using standard methods, height, weight and head circumference (HC) were measured. Children who were <10th percentile of the National Center for Health Statistics charts for height and weight, or alternatively <10th centile for HC, were recorded as screen-positive and invited for clinical assessment. This method is very sensitive, although not very specific, for FAS/PFAS.4
Stage two: diagnostic evaluation
Screen-positive children were assessed by two experienced dysmorphologists for clinical features of FAS including: history of birth events, developmental milestones and medical problems (obtained from the caregiver and the road-to-health card). Pregnancy history was not included, to ensure that the investigators remained blinded to the history of alcohol consumption. Children were also examined for dysmorphic features, neurological signs and intercurrent illness. To standardise the assessment of dysmorphic features, a checklist was used that yielded a 'dysmorphology score', with a maximum of 35.
The Institute of Medicine (IOM) criteria11 were used to diagnose FAS and PFAS. Diagnosis of facial features was based on 'gestalt' appearance and included a smooth upper lip and narrow upper vermilion border, and short palpebral fissures on measurement (<10th centile for age). Positive evidence of neurological abnormality required an HC <10th centile, the presence of 'hard' signs on neurological examination, or significant abnormalities on neurocognitive assessment (below 'average range' score in more than 4 of 10 tests).
A diagnosis of FAS required two of the three primary facial features, together with growth retardation and neurological abnormalities. A PFAS diagnosis required at least two of the three FAS facial features and one of growth retardation, neurological abnormality or abnormal neurocognitive assessment. The clinical diagnosis of FAS, but not PFAS, is considered distinctive even in the absence of a history of maternal alcohol consumption in pregnancy.
Children were classified on the clinical assessment into: FAS if they fulfilled the IOM criteria as determined by both clinicians; deferred if they were uncertain or there was a discrepancy between their diagnoses; or not FAS if there were no clinical features of FAS/PFAS. A dysmorphic syndrome other than FAS was considered in children with dysmorphic features.
For each child classified as FAS or deferred, one control was selected from the not FAS group and matched for child's age, sex and ethnicity. Child development and possible maternal risk factors for FAS were compared between cases and controls.
Trained interviewers completed a structured questionnaire with mothers of children in the FAS, deferred or control groups. A shorter proxy interview was used with a guardian if the mother was deceased or untraceable. Interviews obtained data on demographics, socio-economic status, alcohol consumption and other risk factors for having a child with FAS/PFAS. History of alcohol consumption was elicited using a timeline follow-back method.13
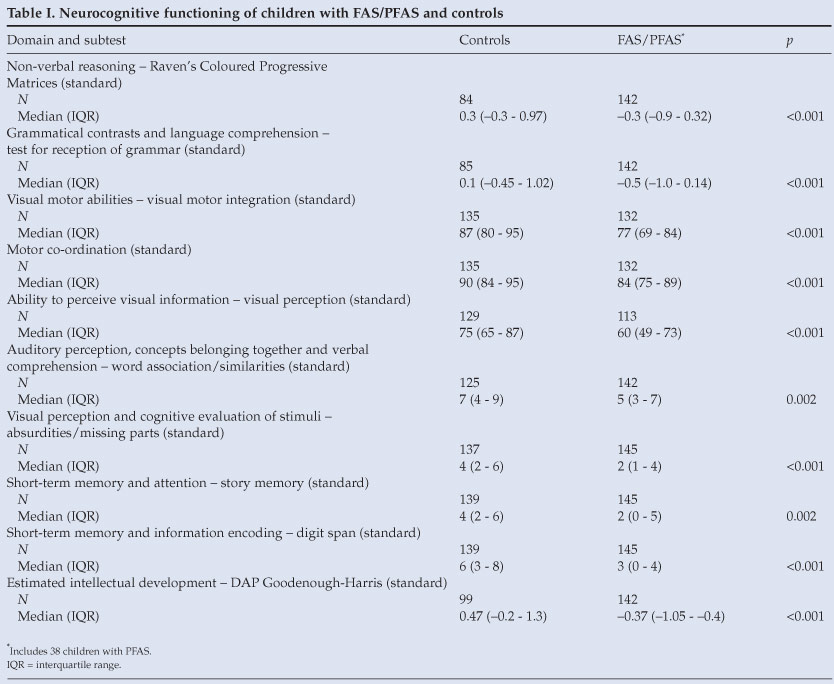
Children in the FAS, deferred and control groups received a neurocognitive assessment, conducted by a registered psychometrist blinded to the clinical diagnosis; this comprised 10 subtests, each assessing a neurocognitive domain (Table I). All subtests had been validated in South Africa except for Test for Reception of Grammar and DAP Goodenough-Harris, for which raw scores were standardised by converting the raw score to a z score and then comparing each child's z score to the average standard score. South African normative ranges exist for Raven's Coloured Progressive Matrices, but its raw scores were also converted into a standard score since participants did not fall within available age ranges.
A case conference made a final diagnosis; the final diagnostic categories were FAS, PFAS and FAS-negative.
Children identified as having FAS/PFAS were referred to local professionals and other services, including speech and hearing therapists, occupational therapists and physiotherapists. With parental permission, school personnel were informed of each child's diagnosis to facilitate educational support, remedial assessment and follow-up by the Department of Education. Children with other medical conditions were linked with local and regional medical services, as required.
Statistical analysis
Intercooled Stata 8.0 (Stata Corporation, College Station, Texas, USA) was used for statistical analysis. For analysis of categorical variables, the chi-square test was used; for continuous variables, we used an unpaired Student's t-test or Mann-Whitney U-test for normally and non-normally distributed data, respectively. Mantel-Haenszel techniques were used for analysis of categorical data from matched cases and controls; only discordant pairs contributed to this analysis.
Results
Characteristics of study sample
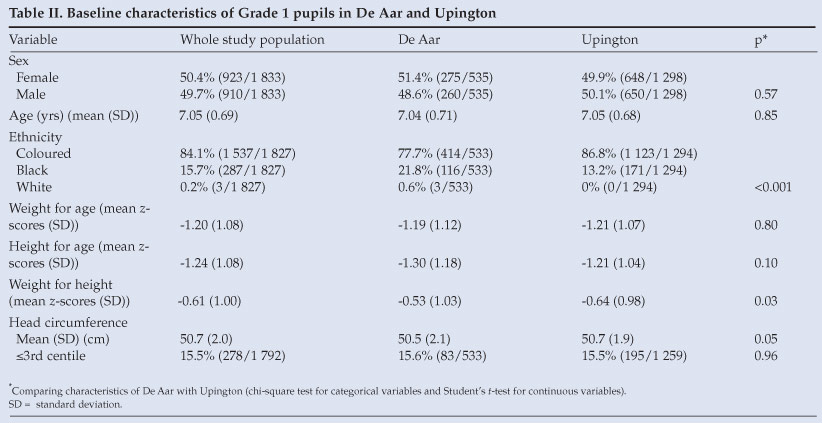
A total of 1 830 pupils were screened in stage 1. In De Aar and Upington, a high proportion of the study population had growth retardation: 66.6% (1 181/1 774) were underweight (<80% of expected weight-for-age); 48.3% (858/1 776) were stunted (<90% of expected height-for-age); and 42.7% (755/ 1 768) were of low weight-for-height (<80% of expected weight-for-height). As a result, many subjects were screen-positive for FAS/PFAS: more in De Aar (66.4%; 354/533) than Upington (57.4%; 744/1 297; p<0.001) (Table II). Differences in denominator are due to missing information.
Prevalence of fetal alcohol spectrum disorders
A total of 123 children were diagnosed with FAS and 38 with PFAS, yielding a FAS prevalence of 67.2/1 000 (95% CI 56.2 -79.7) and a PFAS prevalence of 20.8/1 000 (95% CI 14.7 - 28.4). The overall rate of FAS/PFAS in De Aar was 64/536 (119.4/ 1 000, 95% CI 93.2 - 149.9) and in Upington 97/1 299 (74.7/ 1 000, 95% CI 61.0 - 90.3). Children in De Aar were 1.7 times more likely to have FAS/PFAS than children in Upington (95% CI for OR (odds ratio) 1.2 - 2.4; p=0.002).
Children with FAS/PFAS were a mean 4.6 months older than non-FAS children (95% CI 3.3 - 5.9 months; p<0.001) which may be due to children repeating Grade 1 because of poor performance or delayed school entry. Since the standard school starting age is the year in which a child turns 7, the FAS/PFAS rate was assessed for children who were <7 years when the year began (i.e. children of standard school-entry age). The FAS/PFAS rate was 10.9/1 000 (51/469) in De Aar and 49/ 1 000 (53/1 087) in Upington.
No differences were noted in FAS prevalence among ethnic groups: 7.2% (108/1 501) for coloured children versus 5.3% (15/282) for black children (p=0.25). However, in De Aar, coloured children were significantly more likely to have FAS than black children (p=0.007; OR 3.8, 95% CI 1.3 - 10.8). There were insufficient numbers of white children for meaningful comparisons.
Clinical features of children with FAS/PFAS
Growth parameters of FAS/PFAS children were globally abnormal; 98.3% (112/114) were underweight, 89.5% (102/114) stunted, and 86.8% (99/114) low weight-for-height. Mean dysmorphology scores were 12.0 (SD 5.4) for children with FAS, 8.8 (SD 8.8) for children with PFAS, and 3.7 (SD 3.8) for FAS-negative children.
Neurological and neurocognitive results
Microcephaly (HC <2SD for age and sex) was present in 71.9% (82/114) of children with FAS, 44% (16/36) of those with PFAS and 11.0% (180/1 639) of the non-FAS group. Children with FAS/PFAS performed significantly worse than the control children in all 10 neurodevelopmental subtests (Table I).
Interviews
A total of 223 interviews were conducted with mothers (146), grandmothers (37) or other proxies (40) of 95 children with FAS, 29 with PFAS and 99 matched controls. The overall response rate for interviews related to children with FAS/PFAS was 77% (124 of 161 cases).
Differences between mothers of children with FAS/PFAS and control women were noted in socio-demographic characteristics, especially maternal education and employment (Table III). Women with a FAS/PFAS child also had a lower BMI than other women (median 25.9 v. 22.8 kg/m2; p<0.001).
Discussion
This survey of Grade 1 children found an extremely high prevalence of FAS - higher than that previously reported in Western Cape Province.4,5,13 Although comparisons of FAS rates can be misleading owing to differences in methodology and diagnostic criteria, we believe that the similar methods we used and the referenced studies in Western Cape Province make them relatively comparable. Rates of FAS reported from South Africa are generally much higher than other countries, where rates of FAS seldom exceed 10/1 000, even in high-risk populations.14
These results broaden the evidence that FAS is of considerable public health importance in the Western and Northern Cape provinces, although information available for other provinces of South Africa is limited.
Since mental disability is the most significant effect of FAS, comparing these FAS/PFAS rates to published overall prevalence rates for mental disability due to all causes, is of interest. Worldwide, mental disability rates in developing countries vary from 4 to 138 per 1 000.15 The fact that FAS/ PFAS rates in our study are at the high end of this range indicates the magnitude of the problem.
In South Africa, FAS is often linked to the historical legacy of the dop system in wine-farming areas, and stereotypical assumptions are made that FAS is peculiar to the coloured communities that comprised the local workforce. It is noteworthy that the FAS rate is higher in De Aar (a sheep-farming area) than Upington (a wine-farming area), and that there was no overall difference in FAS/PFAS between black and coloured subjects. Therefore, FAS is limited neither to viticultural areas nor to a specific ethnic group.
Maternal drinking during pregnancy was much more frequently reported in mothers of children with FAS/PFAS than in controls. Alcohol consumption was not confirmed in a minority of FAS cases because families could not be traced or proxy interviewees were not always aware of alcohol histories, rather than because a history of alcohol consumption was denied.
The reported rates of drinking in the control and FAS groups remained high across a 7-year interval from the index pregnancy to the time of interview. It is unclear whether stable drinking rates are maintained in alcohol dependency, or the influence of other factors such as social acceptability, which will be important to clarify for identifying appropriate interventions to reduce alcohol consumption.
In this study, children with FAS and PFAS performed poorly across a broad range of neurodevelopmental domains, with significantly lower results than controls in all tests. Markedly lower intellectual functioning and attention deficits were noted during the assessment. Children with FAS/PFAS particularly struggled with language skills - speaking, writing and basic understanding of words. There was a delay in speed and accuracy of problem solving and practically implementing tasks compared with expected developmental age. Neurocognitive deficits were global and not specific to 'executive functioning' as found by some authors.16
Small HC is a common clinical feature of FAS, and was used as a screening and diagnostic feature of FAS. The difference in mean HC between the FAS and control groups was therefore not surprising, but the high rate of microcephaly (11%) in children not diagnosed with FAS/PFAS was unexpected. It is unclear whether this represents undetected cases of significant prenatal alcohol exposure (a history of maternal alcohol consumption was only sought in cases and controls) or is due to other known causes of poor brain growth, such as malnutrition occurring either prenatally (owing to poor placental blood flow) or in early childhood.17
There was such a high rate of growth retardation in the study population that we feel that most cases resulted from malnutrition rather than FAS. This resulted in a high false-positive rate for the initial screening test, limiting its usefulness in this population.
The low education levels and employment rates indicate that the study sample is generally of low socio-economic status. The higher rate of FAS/PFAS in women who smoke, are less educated, or lack full-time employment, is consistent with previous reports.3
Mothers of FAS/PFAS children had lower BMIs than controls at the time of interview, confirming the findings of a previous small study.18 The significance is uncertain and may be the result of heavy drinking and/or malnutrition, or be a risk factor for FAS. Further investigation is warranted.
The high rate of unplanned pregnancies and low levels of contraceptive use, especially among mothers of children with FAS, is cause for concern. A previous child with FAS is a strong risk factor for having another child with FAS. Unplanned pregnancy hinders modification of drinking behaviour in early pregnancy, which is important because the first trimester is the period of maximal sensitivity to the embryotoxic effects of alcohol.
Study limitations
The complexities of diagnosing FAS hamper efforts to quantify its burden of disease and institute ongoing FAS surveillance. The most important adverse effects relate to neurodevelopment. Neurocognitive assessments were performed only on children clinically suspected of FAS and matched controls, which may cause under-assessment of fetal alcohol spectrum disorder.
The diagnosis of FAS/PFAS remains clinical, and optimal criteria are under debate,19,20 with different diagnostic criteria leading to variations in frequency of diagnosis. Our widely used criteria define FAS features less strictly than some other classifications, which may lead to more frequent diagnosis of FAS. Differences in rates of diagnosis of FAS between different classification systems, but similar overall rates of FAS, have been demonstrated.20
Although we used a comprehensive battery of neurocognitive subtests, there were shortcomings in the assessment tools. The tests have mostly been validated in South Africa, but the applicability of these tests to children from diverse backgrounds is of concern. Nevertheless, significant differences were found between the FAS/PFAS and the control groups across all domains tested.
The interview response rate was suboptimal as tracing mothers and arranging interviews was more difficult than anticipated, particularly because of the death of a key interviewer. The denominators varied between questions since collateral informants could not answer some questions, and some information was available only for the Upington site.
Generalising our findings to other geographical areas is uncertain as there may be systemic differences between the populations studied and those of other rural or urban areas. The likelihood that our results reflect the burden of FAS in the province is strengthened by the use of two towns in different regions. The unique demographics of the Northern Cape suggest that the results are not generalisable to other parts of South Africa.
We thank the staff at the De Aar and Upington study sites of the Foundation for Alcohol Related Research (FARR) for their input and assistance; and we dedicate this paper to the memory of our late co-worker, Stefanie Schön.
References
1. Jones KL, Smith DW. Recognition of fetal alcohol syndrome in early infancy. Lancet 1973; 2: 999-1001. [ Links ]
2. Bertrand J, Floyd RL, Weber MK, et al. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis. Atlanta, Ga.: Centers for Disease Control and Prevention, 2004: 14. [ Links ]
3. Abel EL, Hannigan JH. Maternal risk factors in fetal alcohol syndrome: provocative and permissive influences. Neurotoxicol Teratol 1995; 17(4): 445-462. [ Links ]
4. May PA, Brooke LB, Gossage JP, et al. Epidemiology of fetal alcohol syndrome in a South African community in the Western Cape province. Am J Public Health 2000; 90(12): 1905-1912. [ Links ]
5. May PA, Gossage JP, Marais AS, et al. The epidemiology of fetal alcohol syndrome and partial FAS in a South African community. Drug Alcohol Depend 2007; 88: 259-271. [ Links ]
6. Jacobson JL, Jacobson SW, Sokol RJ, Ager JW. Relation of maternal age and pattern of pregnancy drinking to functionally significant cognitive deficit in infancy. Alcohol Clin Exp Res 1998; 22(2): 345-351. [ Links ]
7. Croxford J, Viljoen D. Alcohol consumption by pregnant women in the Western Cape. S Afr Med J 1999; 99: 962-965. [ Links ]
8. May PA, Gossage JP, Brook LE, et al. Maternal risk factors for fetal alcohol syndrome in the Western Cape Province of South Africa: a population-based study. Am J Public Health 2005; 95: 1190-1199. [ Links ]
9. Leonardson GR, Loudenberg R. Risk factors for alcohol use during pregnancy in a multistate area. Neurotoxicol Teratol 2003; 25: 651-658. [ Links ]
10. May PA, Gossage JP, White-Country M, et al. Alcohol consumption and other maternal risk factors for fetal alcohol syndrome among three distinct samples of women before, during, and after pregnancy: the risk is relative. Am J Med Genet 2004: 127C: 10-20. [ Links ]
11. Institute of Medicine. Stratton KR, Howe CJ, Battaglia FC, eds. Fetal Alcohol Syndrome: Diagnosis, Epidemiology, Prevention and Treatment. Washington, DC: National Academy Press: 1996. [ Links ]
12. Sobell S, Agarwal S, Annis H, et al. Cross-cultural evaluation of two drinking assessment instruments: alcohol timeline follow-back and inventory of drinking situations. Subst Use Misuse 2001; 36: 313-331. [ Links ]
13. Viljoen DL, Gossage JP, Brooke L, et al. Fetal alcohol syndrome epidemiology in a South African community: a second study of a very high prevalence area. J Stud Alcohol 2005; 66(5): 593-604. [ Links ]
14. May PA, Gossage J-P. Estimating the frequency of fetal alcohol syndrome, a summary. Alcohol Res Health 2001; 25: 159-167. [ Links ]
15. Roeleveld N, Zielhuis GA, Gabreels F. The prevalence of mental retardation: a critical review of recent literature. Devel Med Child Neurol 1997; 39: 125-132. [ Links ]
16. Jacobson JL, Jacobson SW. Drinking moderately and pregnancy. Effects on child development. Alcohol Res Health 1999; 23(1), 25-30. [ Links ]
17. Ivanovic DM, Leiva BP, Perez HT, et al. Head size and intelligence, learning, nutritional status and brain development. Neuropsychologia 2004; 42: 1118-1131. [ Links ]
18. Khaole NC, Ramchandani VA, Viljoen DL, Li TK. A pilot study of alcohol exposure and pharmacokinetics in women with or without children with fetal alcohol syndrome. Alcohol Alcohol 2004; 39(6): 503-508. [ Links ]
19. Hoyme HE, May PA, Kalberg WO, et al. A practical approach to diagnosis of fetal alcohol spectrum disorders: Clarification of the 1996 Institute of Medicine criteria. Pediatrics 2005; 115(1): 39-47. [ Links ]
20. Astley SJ. Comparison of the 4-digit diagnostic code and the Hoyme diagnostic guidelines for fetal alcohol spectrum disorders. Pediatrics 2006; 118: 1532-1545. [ Links ]
 Correspondence:
Correspondence:
D Viljoen
(viljoend@iafrica.com)
Accepted 18 April 2008.


{kind=link}
{kind=link}
{kind=link}