










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 no.11 Pretoria nov. 2008
SAMJ FORUM
MEDICINE AND ECONOMICS
Accounting for the full benefits of childhood vaccination in South Africa
Till BärnighausenI; David E BloomII; David CanningIII; Jennifer O'BrienIV
ITill Barnighausen is a family physician and Associate Professor of Health and Population Studies at the Africa Centre for Health and Population Studies, University of KwaZulu-Natal. His research is in HIV epidemiology, health systems and population health
IIDavid E Bloom is Clarence James Gamble Professor of Economics and Demography and Chair of the Department of Global Health and Population at the Harvard School of Public Health (HSPH). His research focuses on the interplay between demography, population health, and economic well-being
IIIDavid Canning is Professor of Economics and International Health in the Department of Global Health and Population at HSPH. His research focuses on the effect of demographic change and population health on economic growth
IVJennifer O'Brien is a researcher in the Department of Global Health and Population at HSPH. Her research focuses on vaccination campaigns, the biology of ageing, and urban health
While remarkable gains in health have been achieved since the mid-20th century, they have been unequally distributed, and mortality and morbidity burdens in some regions remain enormous. Of the almost 10 million children under 5 years of age who died in 2006, only 100 000 died in industrialised countries, while 4.8 million died in sub-Saharan Africa.1 In deciding whether to finance an intervention to improve population health, policy makers commonly weigh the expected population health gains against the costs of the intervention. Most vaccinations included in national immunisation schedules, such as measles vaccination, are both effective in preventing ill health and relatively inexpensive.2 Newer vaccinations, such as those with pneumococcal conjugate vaccine (PCV) or rotavirus vaccine, can effectively prevent child mortality and morbidity but are expensive relative to the vaccinations currently included in national immunisation schedules. Policy makers may therefore decide that - at current prices - the comparison of health gains with costs does not justify the free public provision of these vaccinations. We argue that in addition to the health benefits of vaccinations, their effects on education and income3 and their benefits for unvaccinated community members can be considerable and should therefore be included in calculations to establish the value of vaccinations.
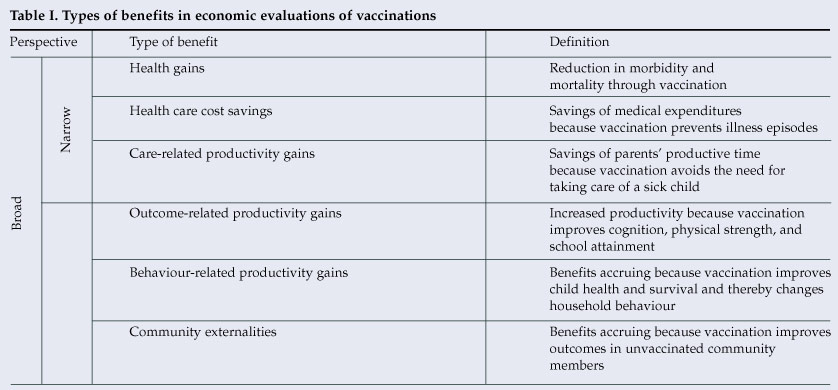
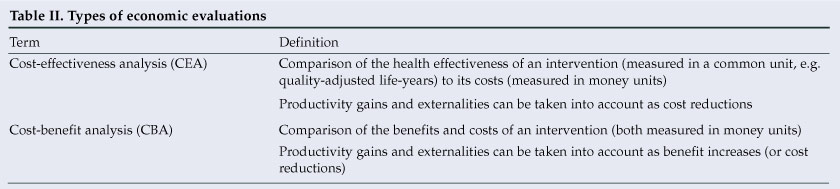
Most economic evaluations of vaccinations focus heavily on the benefits of avoided health care costs (Table I). While it is theoretically possible to take productivity gains into account in economic evaluation (Table II), traditionally, evaluations of vaccinations have either not considered such gains or have only included one particular type of gain: the value of the time that parents would have spent caring for a sick child had a disease episode not been averted by vaccination (care-related productivity gains, Table I).4 Such a narrow perspective may lead to substantial underestimates of the value of some vaccinations. It neglects lifetime productivity gains because a vaccination prevents diseases that can cause cognitive impairment, lead to physical handicap, or reduce school attendance (outcome-related productivity gains, Table I). Cost-benefit analyses (CBAs) in developing countries find return on investment in vaccinations (due to improved cognitive development and worker productivity)5 of similar magnitude to the return on investment in education.6
A narrow focus on care-related productivity gains further excludes increases in productivity due to changes in behaviour in response to vaccination effects (behaviour-related productivity gains, Table I). Many vaccinations significantly reduce child mortality from infectious diseases. As child mortality declines, parents realise that they can give birth to fewer children to attain their desired minimum number of offspring.7 Reduced fertilty leads to a decreasing ratio of economically dependent people in a population, which increases the labour force per capita and savings. Savings, in turn, can be invested in the physical and human capital needed for economic growth. As average family size decreases, parents are likely to invest more in the education and health of each child, leading to improved productivity in adulthood.
Most economic evaluations of vaccinations also do not consider the value of externalities in the wider community, i.e. the effect of a child's vaccination on non-vaccinated community members. Such community externalities (Table I) include reductions in infection rates in unvaccinated people because vaccinations reduce the probability that a healthy individual will encounter an infectious person (up to the point of herd immunity, where sufficient numbers of people are vaccinated such that infection of one individual will not result in an epidemic). They also include decreased rates of antibiotic resistance because less antibiotics are used when more children are protected by vaccination against bacterial infections.
Applying the broad perspective to value of vaccination in South Africa
Taking a broad perspective may be especially important in evaluating vaccinations in South Africa (Table I). From 1976 to 2006, the proportion of the South African population younger than 15 years of age fell from 42% to 32%8 as fertility declined,9 in part the result of HIV-related infertility and fetal loss.10 At the same time, the fraction of working-age adults increased (while the fraction of people aged 65 years and above remained approximately constant).8 When the ratio of children and elderly per working-age adult decreases, a country has an opportunity to develop economically because increased savings lead to greater investment in physical and human capital.7
Health is an important form of human capital, including health attained through vaccinations. South Africa has made great strides in increasing coverage of basic childhood immunisation. The South African Demographic and Health Survey reported coverage with routine vaccines in children 12 - 23 months of age ranging from 62% for measles vaccination to 81% for bacille Calmette-Guérin (BCG) vaccination in 2003.11
Vaccinations have contributed significantly to South Africa's decline in child mortality. From 1975 to 1990, under-5 mortality declined by almost half, from 110 to 60 deaths per 1 000 live births.9 However, this trend has been reversed recently, largely because of the HIV epidemic.12 The under-5 mortality rate in South Africa was 69 per 1 000 live births in 200611 and is therefore not on target to achieving the UN's Millennium Development Goal of reducing under-5 mortality by two-thirds between 1990 and 2015.
Many interventions that could reduce child mortality in South Africa - such as improved access to safe water and sanitation, improved childhood nutrition, or poverty reduction - require large infrastructure investment or sustained changes in social policy. In this situation, the recent decision by the South African Department of Health to add PCV and rotavirus vaccinations to the national immunisation schedule, despite their comparatively high prices,13 is noteworthy and may serve as an example for other countries to follow.
Pneumococcal diseases are a major cause of childhood mortality and morbidity in South Africa.14 PCV is effective in preventing pneumococcal diseases, including pneumonia, meningitis and otitis media. (While we describe productivity gains and externalities using the example of PCV vaccination, a similar case of substantial vaccination benefits can be made for the rotavirus vaccine.) Because HIV-infected children are at significantly higher risk of acquiring pneumococcal disease than uninfected children, PCV will prevent larger numbers of pneumococcal infections and deaths in HIV-infected children, even though they are less likely to develop a protective immune reaction in response to PCV than HIV-uninfected children.15 A large randomised controlled trial in South Africa found that PCV prevented 267 and 2 573 cases of pneumococcal pneumonia per 100 000 person-years in HIV-uninfected and HIV-infected children, respectively.14 PCV vaccination is therefore an appropriate intervention to mitigate the negative effect of HIV on child mortality. In addition to its health benefits, PCV coverage may lead to behaviour-related productivity gains, if the mortality reduction due to vaccination accelerates South Africa's current fertility decline.
PCV is further likely to lead to considerable outcome-related productivity gains. First, episodes of pneumococcal pneumonia will keep children, especially those who are HIV-infected, out of school for substantial periods of time, preventing cognitive development and learning.16 Second, survivors of pneumococcal meningitis frequently suffer from severe cognitive and neurological sequelae; a study in The Gambia found that 58% of children who had survived a bout of pneumococcal meningitis 'had clinical sequelae; half of them had major disabilities preventing normal adaptation to social life', such as mental retardation, hearing loss, motor abnormalities and seizures.17 Third, pneumococcal otitis media can impair cognitive development; a study in the USA found that time spent with middle ear effusion during the first 3 years of life was significantly associated with lower scores on tests of cognitive ability, speech and language, and lower school performance at age 7 years.18 Fourth, pneumococcal otitis media leads to hearing loss in a substantial proportion of affected children.19 While hearing-impaired children in developed countries receive specialised support necessary to attain educational levels on par with non-deaf children, such systems are lacking in many developing countries.20
Moreover, PCV coverage is likely to benefit unvaccinated community members. It decreases the rate of occurrence of antibiotic-resistant pneumococcal infections,21 avoiding the health costs of untreatable disease and the health care costs of using more expensive second-line antibiotics. As pneumococcal disease can cause substantial morbidity and mortality in the elderly and in the HIV-infected middle-aged, childhood PCV vaccination is likely to lead to substantial reduction in pneumococcal disease burden in population groups that will not routinely receive the vaccination. A study in the USA taking such herd effects into account found large benefits from the externality,22 but most other studies of PCV value have ignored them.23 Herd protection against pneumococcal disease may be especially important in South Africa, where a large proportion of the adult population is HIV-positive and therefore vulnerable to severe recurrent pneumococcal infections.
Conclusions
South Africa has proven its commitment to ensuring that children receive effective vaccines, attaining high national vaccination coverage levels. In 2006 the country pledged $20 million to the International Finance Facility for Immunization (IFFIm), the major source of finance for the GAVI Alliance's effort to extend coverage with new and under-used vaccines to low-income countries.24 More recently, South Africa decided to include PCV and rotavirus vaccinations in its national immunisation schedule.25 It is highly likely that coverage of children with the two vaccines will not only reduce child morbidity and mortality, but will also lead to significant productivity gains, contributing to South Africa's economic development, and benefit unvaccinated South Africans. The precise size of the contributions of these productivity gains and externalities to health and wealth in South Africa are unknown. Adding the two vaccinations to the national immunisation schedule offers an excellent opportunity to measure these effects, and evaluation studies should complement the vaccination roll-out. As the evidence grows, we expect the estimates of the value of many vaccinations to increase significantly, ensuring that policy makers have the necessary information to make optimal choices on vaccination provision.
The authors acknowledge financial support from The Pneumococcal Vaccines Accelerated Development and Introduction Plan (PneumoADIP) at the Johns Hopkins Bloomberg School of Public Health in connection with a multi-country research project on the value of vaccination.
1. UNICEF. The State of the World's Children 2008. New York: UNICEF, 2007. [ Links ]
2. World Health Organization. Vaccine-preventable disease. 2008. http://www.who.int/immunization_monitoring/diseases/en/ (accessed 4 September 2008). [ Links ]
3. Schultz TP. Evidence of returns to schooling in Africa from household surveys: monitoring and restructuring the market for education. 2003. http://www.econ.yale.edu/growth_pdf/cdp875.pdf (accessed 28 September 2008). [ Links ]
4. Ehreth J. The global value of vaccination. Vaccine 2003; 21: 596-600. [ Links ]
5. Bloom D, Canning D, Weston M. The value of vaccination. World Economics 2005; 6: 15-39. [ Links ]
6. Psacharopoulos G, Patrinos H. Returns on investment in education: a further update. Education Economics 2004; 12: 111-134. [ Links ]
7. Bloom D, Canning D, Sevilla J. The Demographic Dividend. Santa Monica, USA: RAND, 2003. [ Links ]
8. World Bank. World Development Indicators. Washington, DC: World Bank, 2008. [ Links ]
9. Moultrie TA, Timaeus IM. Trends in South African Fertility between 1970 and 1998. Cape Town: South African Medical Research Council, 2002. [ Links ]
10. Zaba B, Gregson S. Measuring the impact of HIV on fertility in Africa. AIDS 1998; 12: Suppl 1, S41-50. [ Links ]
11. Department of Health, Medical Research Council. South Africa Demographic and Health Survey 2003. Pretoria: Department of Health, 2007. [ Links ]
12. Nannan N, Bradshaw D, Timaeus IM, Dorrington R. The impact of HIV/AIDS on infant and child mortality in South Africa. In: 16th International Conference on AIDS, 2000, Durban, South Africa. http://gateway.nlm.nih.gov/MeetingAbstracts/ma?f=102238260.html (accessed 7 October 2008). [ Links ]
13. Ngcobo M. Improved pneumonia vaccine, but not for poor. 2007. http://www.health-e.org.za/news/article.php?uid=20031704 (accessed 8 September 2008). [ Links ]
14. Madhi SA, Kuwanda L, Cutland C, Klugman KP. The impact of a 9-valent pneumococcal conjugate vaccine on the public health burden of pneumonia in HIV-infected and -uninfected children. Clin Infect Dis 2005; 40: 1511-1518. [ Links ]
15. Zar HJ, Madhi SA. Pneumococcal conjugate vaccine - a health priority. S Afr Med J 2008; 98: 463-467. [ Links ]
16. Heiskanen-Kosma T, Korppi M, Leinonen, M. Serologically indicated pneumococcal pneumonia in children: a population-based study in primary care settings. Apmis 2003; 111: 945-950. [ Links ]
17. Goetghebuer T, West TE, Wermenbol V, et al. Outcome of meningitis caused by Streptococcus pneumoniae and Haemophilus influenzae type b in children in The Gambia. Trop Med Int Health 2000; 5: 207-213. [ Links ]
18. Teele DW, Klein JO, Chase C, Menyuk P, Rosner BA. Otitis media in infancy and intellectual ability, school achievement, speech, and language at age 7 years. Greater Boston Otitis Media Study Group. J Infect Dis 1990; 162: 685-694. [ Links ]
19. Tuomanen EI. Pathogenesis of pneumococcal inflammation: otitis media. Vaccine 2000; 19: Suppl 1, S38-40. [ Links ]
20. Berke J. Ways to help deaf people in developing countries. 2007. http://deafness.about.com/od/deafcommunity/a/waystohelp.htm (accessed 1 September 2008). [ Links ]
21. Kyaw MH, Lynfield R, Schaffner W, et al. Effect of introduction of the pneumococcal conjugate vaccine on drug-resistant Streptococcus pneumoniae. N Engl J Med 2006; 354: 1455-1463. [ Links ]
22. Ray GT, Whitney CG, Fireman BH, Ciuryla V, Black SB. Cost-effectiveness of pneumococcal conjugate vaccine: evidence from the first 5 years of use in the United States incorporating herd effects. Pediatr Infect Dis J 2006; 25: 494-501. [ Links ]
23. Beutels P, Thiry N, Van Damme P. Convincing or confusing? Economic evaluations of childhood pneumococcal conjugate vaccination - a review (2002 - 2006). Vaccine 2007; 25: 1355-1367. [ Links ]
24. GAVI Alliance. GAVI Alliance Progress Report 2007. Geneva: GAVI Alliance, 2007. [ Links ]
25. Govender S. South Africa: milestone vaccine rollout to fight infant mortality. 2008. http://allafrica.com/stories/200809120703.html (accessed 18 September 2008). [ Links ]


{kind=link}
{kind=link}