










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 n.10 Pretoria Oct. 2008
ORIGINAL ARTICLES
Symptomatic hyperlactataemia in adults on antiretroviral therapy: A single-centre experience
June FabianI; Willem D F VenterII; Louisa MkhabelaIII; Jonathan B LevinIV; Lee BakerV; Saraladevi NaickerVI
IFCP (SA), Cert Neph (SA). Division of Nephrology, Department of Medicine, University of the Witwatersrand, Johannesburg
IIFRCP (Lond), PhD. Division of Nephrology, Department of Medicine, University of the Witwatersrand, Johannesburg
IIIFCP (SA), DTM&H, Dip HIV Management. Reproductive Health and HIV Research Unit, University of the Witwatersrand, Johannesburg
IVMB BCh. HIV Clinic, Johannesburg Hospital, Gauteng Department of Health
VPhD. Biostatistics Unit, Medical Research Council of South Africa, Johannesburg
VIDip Pharm. Amayeza (Medicines) Information Services, Johannesburg
ABSTRACT
OBJECTIVE: There are limited data on symptomatic hyperlactataemia caused by antiretroviral therapy (ART) in resource-limited settings. We assessed individuals who developed symptomatic hyperlactataemia on ART in an outpatient clinic in South Africa.
DESIGN: A retrospective record review was performed on patients attending the clinic from January 2004 to December 2005.
RESULTS: Thirty-five patients, all on stavudine-containing regimens, developed symptomatic hyperlactataemia. The incidence in this population was 20.5 cases per 1 000 person-years of ART with an associated mortality of 21%. The major risk factor was being female (risk ratio (RR) 3.27). Significant clinical symptoms preceding symptomatic hyperlactataemia include nonspecific gastrointestinal symptoms, weight loss, and development of symptomatic neuropathy.
CONCLUSIONS: The incidence of symptomatic hyperlactataemia in our population was high. Simple clinical measures, such as neuropathy symptoms and monitoring of weight, may alert the clinician to impending symptomatic hyperlactataemia. Early diagnosis expedites safe outpatient care and switching of ART regimens without interruption, in many cases.
The use of nucleoside reverse transcriptase inhibitors (NRTIs) in combination with other antiretroviral drugs in a schedule of antiretroviral therapy (ART) is considered standard-of-care for those living with HIV.1-3 ART has led to significant decreases in morbidity and mortality, compared with untreated HIV-infected patients. This benefit also extends to those in developing countries.1,2
Public sector access to ART was initiated in 2004 in South Africa. The recommended first-line regimen comprises two NRTIs in combination with a non-nucleoside reverse transcriptase inhibitor (NNRTI).4 The combination most frequently used is stavudine, lamivudine and efavirenz ('regimen 1a'). Nevirapine is recommended instead of efavirenz (owing to teratogenicity concerns) for women of child-bearing potential ('regimen 1b'). 'Regimen 2' includes the combination of didanosine, zidovudine and lopinavir/ritonavir. Criteria for initiation of ART in the public sector for adults and adolescents are CD4 <200 cells/µl irrespective of clinical stage, or World Health Organization stage IV illness irrespective of CD4 count.4
Several serious ART-related complications have been noted in the era of chronic, effective treatment, including NRTI-related symptomatic hyperlactataemia. At present, although more is understood regarding its pathogenesis, the best treatment is a high index of clinical suspicion, early detection and prompt cessation of the offending agents.5-7
We performed a retrospective review of records from a large clinic in Johannesburg to identify the incidence of symptomatic hyperlactataemia and its risk factors.
Methods
Study population
Johannesburg Hospital runs a large ART outpatient clinic. We retrospectively reviewed the records of all patients attending the outpatient clinic, and extracted data from those with documented symptomatic hyperlactataemia for the period 1 January 2004 to 31 December 2005. Data included race, age and gender of all patients and, in those with hyperlactataemia, weight, details of antiretroviral drug history, CD4 cell count, viral load, clinical signs, symptoms and events, and relevant blood tests. Testing for hyperlactataemia is only performed if clinically indicated, and routine screening is not done. Death was defined as in-hospital mortality. Lactic acidosis was defined as pH <7.35, bicarbonate <20 mmol/l and raised lactate (>5.0 mmol/l). Severe hyperlactataemia was defined as a lactate measurement >5.0 mmol/l and therefore includes lactic acidosis.8 Those with lactate <5.0 mmol/l and other potential causes for hyperlactataemia were excluded.
The study was approved by the Human Research Ethics Committee, University of the Witwatersrand (protocol number M0500933).
Statistical analysis
Data were exported to the statistical package Stata Release 8.0 for analysis. Descriptive analyses were carried out with continuous variables being summarised using means, standard deviations, medians, interquartile ranges and ranges; in some cases, 95% confidence intervals (CIs) for the mean were calculated. Categorical variables were summarised using frequencies and percentages of non-missing values.
Results
For the time period under review (1 January 2004 -31 December 2005), a total of 2 587 patients >18 years were initiated on ART; 1 674 (65%) were females and 913 (35%) were males. A total of 39 patients with lactate levels >5.0 mmol/l were identified. Of these, 4 were excluded: a 27-year-old woman with sepsis, haemolytic anaemia and jaundice; a 23-year-old woman with diarrhoea; a 30-year-old woman with a history of lactic acidosis in 2003 on dual regimen didanosine and stavudine (she interrupted therapy for 11 months, was recommenced on stavudine, and died from Pneumocystis jirovecii pneumonia immune reconstitution inflammatory syndrome); and the fourth patient because no clinic records were found. Of the remaining 35 patients, 5 (14%) were male, 30 (86%) female and 34/35 were black (Table I).
ART choice and ART-related side-effects before onset of symptomatic hyperlactataemia
Of all patients in the clinic, 82.6% were started on stavudine, lamivudine and efavirenz; 10.4% on stavudine, lamivudine and nevirapine; 0.8% on zidovudine, didanosine and lopinavir/ ritonavir; and 6.2% on various combinations. Of the 35 patients who developed symptomatic hyperlactataemia, all were on a stavudine-containing regimen, with 3 on a stavudine-didanosine combination. This latter combination was the most affordable NRTI treatment available before the State ART programme, and some patients and clinicians elected not to change if viral suppression was achieved and the combination well tolerated. In those with symptomatic hyperlactataemia, 2 males developed gynaecomastia without other symptoms of lipodystrophy; 8 patients experienced onset of a symptomatic neuropathy after commencement of ART; and 1 patient developed acute pancreatitis followed 6 months later by admission for frank diabetic ketoacidosis (no prior diagnosis of diabetes mellitus).
Symptoms at the time of the symptomatic hyperlactataemia
Most patients presented with nonspecific symptoms. Gastrointestinal complaints were the most common: epigastric/abdominal pain, vomiting, loss of appetite, loss of weight, nausea, diarrhoea, heartburn and dyspepsia. Cardiorespiratory complaints were documented as shortness of breath, cough, chest pain and palpitations. Neuropsychiatric symptoms included neuropathy, dizziness and depressed mood. Other symptoms were bipedal oedema, cramping, and swelling of hands/fingers.
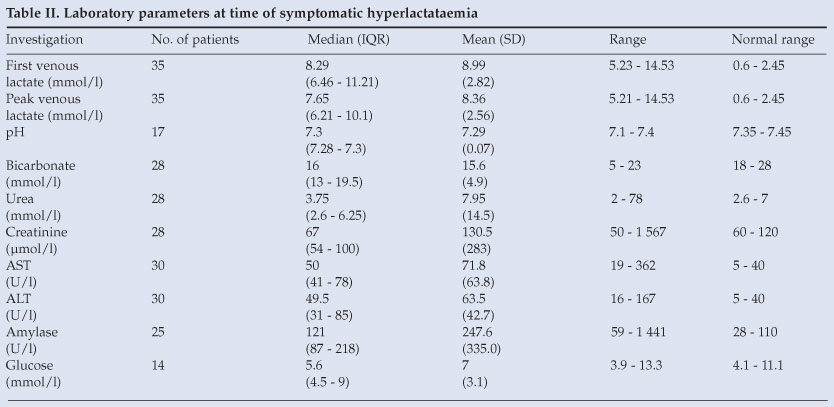
Features on clinical examination and laboratory findings at the time of symptomatic hyperlactataemia (Table II)
One patient gained weight; 4 had stable weights when compared with their measured weights from preceding visits. There was no record of preceding weights in 7 patients. Twenty-three patients lost weight before their presentation; the objective weight loss in 2 of these patients was not recorded. In the remaining 21 patients, mean weight loss was 4.75 kg (95% CI 2.28 - 7.22). Many patients started losing weight several visits before the diagnosis of symptomatic hyperlactataemia. Symptoms suggestive of neuropathy were evident in 13 of 35 patients (37%); 17 of 35 patients had no features of a neuropathy (49%); and there was no documentation in 5 cases (14%). Baseline venous lactate level used for the purpose of this analysis was the first lactate taken to make the diagnosis. Peak venous lactate levels, where known, have been included as this parameter has been shown to be a poor prognostic marker.9
Outcome
One patient was lost to follow-up. Twelve out of 34 (35%) were treated as outpatients, all of whom survived. Twenty-two out of 34 (65%) were inpatients, of whom 7 died. Of those who died, 2 were admitted to the intensive care unit for multiple organ failure and received dialysis support. No other patients were dialysed. The median duration of admission, from data available for 19 patients, was 11 days (range 1 - 21). The overall mortality was 21% (7/34). Of those who died, 5/7 (71%) had peak venous lactate levels >10 mmol/l compared with those who survived, of whom only 8/27 (30%) had peak venous lactate levels >10.0 mmol/l. The survival rate among the remaining 27 patients was 100% after a mean follow-up of 26.7 weeks. Twelve (45%) were successfully changed from stavudine to zidovudine with no recurrence of symptoms. Six of these were successfully switched as outpatients with no interruption. Of all patients in the clinic who were commenced on ART during the review period, 30/1 674 women (1.79%) and 5/913 men (0.55%) developed symptomatic hyperlactataemia. The relative risk in this study of women developing symptomatic hyperlactataemia compared with men was therefore 3.27 (95% CI 1.27 - 8.41).
Discussion
To our knowledge, this is the largest published series of symptomatic hyperlactataemia from a single site. However, here have been large numbers of anecdotal reports in our region,10,11 leading to local guidelines for the treatment of this condition.12 A study in Uganda reported low rates (0.5%) of lactic acidosis with similar ART regimens.13
Symptomatic hyperlactataemia/lactic acidosis is part of the spectrum of mitochondrial toxicity associated with NRTI therapy. It has been reported in persons receiving both single-and dual-NRTI regimens.5-7,14 The quoted incidence of lactic acidosis varies, depending upon definitions used, but ranges from 1.3 to 25.2 cases per 1 000 person-years of ART.15 The incidence of symptomatic hyperlactataemia in this study was 20.5 cases per 1 000 person-years of ART. 'Threshold' lactate levels are proposed by some as a prognostic marker. In one study, lactate levels of >9 mmol/l were associated with a positive predictive value for death of 81.82% and a negative predictive value of 94.44%. Others have used a 'threshold' of >10 mmol/l to predict mortality ranging from 60% to 80%.16 In our series, a lactate >10 mmol/l was associated with amortality of 71%.
Stavudine and didanosine are the most frequent NRTIs implicated in mitochondrial toxicity. The combination of stavudine and didanosine is associated with the greatest relative risk.6,7,14,15 All the patients who developed symptomatic hyperlactataemia in this study were on a stavudine-containing regimen; 8 patients in the entire clinic were on a stavudine/didanosine combination and, of these, 3 developed symptomatic hyperlactataemia, confirming the long experience of severe mitochondrial toxicity with this combination.
The risk of symptomatic hyperlactataemia may vary with demographics, being somewhat more common in black women, the obese and those with hepatitis B or C co-infection, but this is based on small case series.5,6,15 The role of female gender and obesity as potential predisposing factors may be applicable to our study population. A study comparing metabolic side-effects of ART in men and women showed 59% of women were of Haitian or African origin. After adjusting for age, CD4 cell count, viral load, time since HIV diagnosis, history of AIDS-defining illnesses and year of ART initiation, no sex/gender differences were observed in the overall incidence of hyperglycaemia, hypercholesterolaemia and lipodystrophy. Women did, however, have a significantly higher risk of developing lactic acidosis than men (5.2% v. 2.2%; p=0.0009).17 Similarly, there is a higher incidence of symptomatic hyperlactataemia in women compared with men in our series, with a relative risk of 3.27 for females. This figure is higher than that found in another review where the relative risk was 2.5.5 The median body weight among those who developed symptomatic hyperlactataemia was 72 kg, but the retrospective nature of this record review precludes further analysis of the significance of this finding. It has been suggested that being overweight may be a risk factor.14,18 It is postulated that being overweight, or weight gain, may predispose to hepatic steatosis, compromising the liver's ability to clear excess lactate.14 Of patients attending the clinic, 92% are black, the rest being white, coloured or of Indian descent.19 A single case was seen in a white patient, making analysis of race as a risk factor difficult.
Pre-existing chronic hepatitis B and C infection have been identified as risk factors for milder, asymptomatic forms of nucleoside-analogue-related liver toxicity, but a clear association with symptomatic hyperlactataemia has not been established.20 It is not routine practice to screen for hepatitis B or C infection in this clinic as the prevalence of hepatitis C infection in our indigenous population is extremely low, although one case from our clinic had documented infection and was one of the fatalities. The prevalence of chronic hepatitis B infection in the clinic population, and its influence on the development of this complication, is an area for further research. Renal and hepatic laboratory abnormalities (Table II) in our patients at the time of diagnosis were similar to those in other studies.6,14
Studies have confirmed that asymptomatic hyperlactataemia in patients on ART does not predict for development of symptomatic hyperlactataemia.21,22 From these data, there may be a few laboratory or clinical indicators that clinicians can utilise to detect the condition early, as it appears to be insidious in onset and progressive in nature, with nonspecific symptoms. The most powerful tool at present is a health care practitioner who can diagnose and intervene early with minimal investigation.
Gastrointestinal complaints were by far the most common symptoms reported. In many patients, these symptoms were documented at clinic visits before the diagnosis of symptomatic hyperlactataemia. 'Easy to detect' clinical signs are unexplained weight loss and neuropathy. It is imperative that weight is routinely monitored. Weight loss, in 83% of our patients, has been documented in other series14 and, when it occurs, must be quickly investigated. This is attainable in resource-limited settings. Another potential sign is the onset of neuropathy after commencement of ART. In our clinic, 37% of patients had neuropathy at the time of diagnosis. Early switching to zidovudine may prevent the more severe manifestations of mitochondrial toxicity.
Therapeutic intervention for symptomatic hyperlactataemia included the immediate discontinuation of all antiretroviral agents at the time of diagnosis or strong suspicion thereof. If admitted to the hospital, supportive care was offered in the form of intravenous fluids, glucose and bicarbonate solution. In patients with suspected sepsis, empirical antibiotics were administered. Those with pancreatic dysfunction were kept nil per os until pancreatic function normalised, clinicians having the impression that cessation of enteral feeding enhanced their recovery. Others have described the use of total parenteral nutrition as part of their care.14 Haemodialysis was performed on 2 patients in intensive care, and both died. In our experience, patients who progress rapidly to multiple organ dysfunction/failure carry the worst prognosis.
The mortality rate in our group was 21%, which appears to be less than that reported by other centres, where mortality from symptomatic hyperlactataemia ranged from 25% to 60%.9,14,16 It is noteworthy that of those treated as outpatients, 100% survived.
Confounding factors that may have introduced bias in our survival data may have been the retrospective nature of this record review, partial data collection, interpretation biases and incomplete medical records. Bias could also have been introduced because some patients with symptomatic hyperlactataemia might have been misdiagnosed and subsequently died; some patients might have been admitted to other hospitals in the area and died, or died at home without our knowledge. However, a recently completed drive within the clinic to trace defaulters and patients who died, showed that most patients who died did so shortly after commencing ART.23 This suggests that immune suppression, immune reconstitution syndromes and possibly acute ART toxicity were responsible for the vast majority of deaths, rather than the more chronic toxicity of mitochondrial damage.
Conclusion
Simple clinical measures, such as detection of symptomatic neuropathy and weight loss, may alert the clinician to impending symptomatic hyperlactataemia, particularly in women and overweight patients. Aggressive clinical investigation of unintentional weight loss is justified in people on ART. Early diagnosis of symptomatic hyperlactataemia allows safe outpatient care and uninterrupted switching of ART regimens in some. Co-treatment with stavudine and didanosine carries a very high risk for this complication, and should not be used.
Ideally, replacing stavudine with an equally potent NRTI in first-line therapy that is easy to use, has a better safety profile and is affordable in South Africa, would decrease mitochondrial toxicity syndromes significantly. Tenofovir is currently under registration review and, along with abacavir, is being considered as an alternative. However, both drugs are significantly more expensive and carry alternative toxicities.
We thank Ms Lucy Nomathansanqa Ndlovu, Ms Busisiwe Ntulini and the staff of the HIV Clinic at Johannesburg Hospital for their assistance, Dr Judy Kirk for assistance in the clinic, the patients on ART who contributed to the study, and the doctors who have shared their experience and expertise with us.
Dr Venter is supported by PEPFAR. There is no conflict of interest regarding any of the authors.
We also wish to dedicate this work to Louisa Mkhabela. Louisa was a vital member of the team that initiated the antiretroviral rollout at Johannesburg Hospital and was one of the first clinicians to treat patients with lactic acidosis. She dedicated herself to patients and their wellbeing, in spite of fighting a brave battle of her own against multiple relapses and remissions for breast cancer. Louisa died on 13 August 2007. She is sorely missed - an inspiration and teacher to patients and staff alike.
References
1. Carr A, Cooper DA. Adverse effects of antiretroviral therapy. Lancet 2000; 356(9239): 14231430. [ Links ]
2. Gazzard B. British HIV Association (BHIVA) guidelines for the treatment of HIV-infected adults with antiretroviral therapy (2005). HIV Med 2005; 6 Suppl 2: 1-61. [ Links ]
3. Gilks CF, Crowley S, Ekpini R, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet 2006; 368: 505-510. [ Links ]
4. Department of Health. National Antiretroviral Treatment Guidelines. Pretoria: Jacana, 2004. [ Links ]
5. Arenas-Pinto A, Grant AD, Edwards S, Weller IV. Lactic acidosis in HIV infected patients: a systematic review of published cases. Sex Transm Infect 2003; 79(4): 340-343. [ Links ]
6. Ogedegbe AE, Thomas DL, Diehl AM. Hyperlactataemia syndromes associated with HIV therapy. Lancet Infect Dis 2003; 3(6): 329-337. [ Links ]
7. Tripuraneni NS, Smith PR, Weedon J, Rosa U, Sepkowitz D. Prognostic factors in lactic acidosis syndrome caused by nucleoside reverse transcriptase inhibitors: report of eight cases and review of the literature. AIDS Patient Care STDS 2004; 18(7): 379-384. [ Links ]
8. Lactic Acidosis International Study Group. Risk factors for lactic acidosis and severe hyperlactataemia in HIV-1-infected adults exposed to antiretroviral therapy. AIDS 2007; 21(18): 2455-2464. [ Links ]
9. Claessens YE, Cariou A, Monchi M, et al. Detecting life-threatening lactic acidosis related to nucleoside-analog treatment of human immunodeficiency virus-infected patients, and treatment with L-carnitine. Crit Care Med 2003; 31(4): 1042-1047. [ Links ]
10. Eshun-Wilson I, Soentjens P, Zeier M, Taljaard J. Symptomatic hyperlactataemia and lactic acidosis in the era of highly active antiretroviral therapy. S Afr Med J 2005; 95(12): 929-930. [ Links ]
11. Geddes R, Knight S, Moosa MY, Reddi A, Uebel K, Sunpath H. A high incidence of nucleoside reverse transcriptase inhibitor (NRTI)-induced lactic acidosis in HIV-infected patients in a South African context. S Afr Med J 2006; 96(8): 722-724. [ Links ]
12. Southern African HIV Clinicians Society. Guidelines for the Prevention, Diagnosis and Management of NRTI-associated Symptomatic Hyperlactataemia and Lactic Acidosis. Southern African Journal of HIV Medicine 2006; 22: 8-15. [ Links ]
13. Forna F, Liechty CA, Solberg P, et al. Clinical toxicity of highly active antiretroviral therapy in a home-based AIDS care program in rural Uganda. J Acquir Immune Defic Syndr 2007; 44(4): 456-462. [ Links ]
14. Coghlan ME, Sommadossi JP, Jhala NC, Many WJ, Saag MS, Johnson VA. Symptomatic lactic acidosis in hospitalized antiretroviral-treated patients with human immunodeficiency virus infection: a report of 12 cases. Clin Infect Dis 2001; 33(11): 1914-1921. [ Links ]
15. Calza L, Manfredi R, Chiodo F. Hyperlactataemia and lactic acidosis in HIV-infected patients receiving antiretroviral therapy. Clin Nutr 2005; 24(1): 5-15. [ Links ]
16. Falco V, Rodriguez D, Ribera E, et al. Severe nucleoside-associated lactic acidosis in human immunodeficiency virus-infected patients: report of 12 cases and review of the literature. Clin Infect Dis 2002; 34(6): 838-846. [ Links ]
17. Boulassel MR, Morales R, Murphy T, Lalonde RG, Klein MB. Gender and long-term metabolic toxicities from antiretroviral therapy in HIV-1 infected persons. J Med Virol 2006; 78(9): 1158-1163. [ Links ]
18. Patel AK, Patel K, Patel J. Lactic acidosis in HIV-I infected patients receiving antiretroviral therapy. J Assoc Physicians India 2004; 52: 666-669. [ Links ]
19. Hudspeth J, Venter W, van Rie A, Wing J, Feldman C. Access to and early outcomes of a public South African adult antiretroviral clinic. Conference on Retroviruses and Opportunistic Infections (CROI), 22-25 February 2005, Boston, Massachusetts. [ Links ]
20. Day L, Shikuma C, Gerschenson M. Mitochondrial injury in the pathogenesis of antiretroviral-induced hepatic steatosis and lactic acidaemia. Mitochondrion 2004; 4: 95-109. [ Links ]
21. Moyle GJ, Datta D, Mandalia S, Morlese J, Asboe D, Gazzard BG. Hyperlactataemia and lactic acidosis during antiretroviral therapy: relevance, reproducibility and possible risk factors. AIDS 2002; 16(10): 1341-1349. [ Links ]
22. Imhof A, Ledergerber B, Gunthard HF, Haupts S, Weber R. Risk factors for and outcome of hyperlactatemia in HIV-infected persons: is there a need for routine lactate monitoring? Clin Infect Dis 2005; 41(5): 721-728. [ Links ]
23. Mqhayi M, Dalal R, Venter W. Causes for defaulting antiretrovirals in an urban clinic. 13th Conference on Retroviruses and Opportunistic Infections (CROI), 5-8 February 2006, Denver, Colorado, USA. [ Links ]
 Correspondence:
Correspondence:
J Fabian
(June.Fabian@wits.ac.za)
Acccepted 8 July 2008.


{kind=link}
{kind=link}