










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 no.10 Pretoria oct. 2008
SCIENTIFIC LETTERS
Imaginary bugs, real distress: Delusional parasitosis
John FreanI; Gillian de JongII; Richard AlbrechtIII
IMB BCh, MMed (Path), DTM&H. National Institute for Communicable Diseases and University of the Witwatersrand, Johannesburg
IIMB BCh, FCPath (Micro), DTM&H. National Institute for Communicable Diseases and University of the Witwatersrand, Johannesburg
IIIMB BCh, DipPEC. PO Box 793, Strubensvalley, 1735
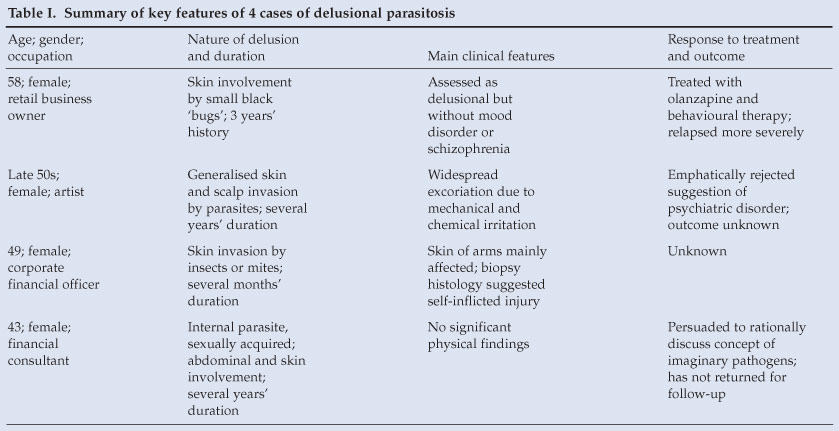
To the Editor: Delusional parasitosis (DP) (Ekbom syndrome, psychogenic parasitosis, chronic tactile hallucinosis) is a false but unshakable conviction of personal infection by 'bugs' of some sort; that is, ecto- or endoparasites or other pathogens. This condition may be increasing in frequency, but the subject is virtually absent from the South African medical literature. Failure to diagnose DP consumes time and financial resources, and prolongs distress and frustration of the doctor and patient. Diagnosis of underlying psychiatric or organic disease can be missed or delayed if DP is not investigated and managed appropriately. We have encountered 4 cases recently (Table I).
Psychiatric aspects
There are three forms of DP:1 primary DP, when the delusion is the only evidence of disease; DP secondary to psychiatric disease; and DP secondary to other medical conditions, intoxication, or substance abuse. Consideration of underlying medical or psychiatric conditions is essential for assessment of DP. Associated psychiatric disorders include schizophrenia, anxiety, depression, obsessive-compulsive disorder, bipolar disorder, phobias, and hypochondriasis. DP may be secondary to many medical conditions, including neurological (head injury, infections, tumours, multiple infarcts), endocrine (thyroid dysfunction, diabetes mellitus), haematological (leukaemia, severe anaemia) and cardiopulmonary (congestive heart failure, asthma) conditions; systemic infections (HIV, tuberculosis, leprosy); malignancies (lymphomas, tumours of breast, lung, colon); nutritional deficiencies (vitamin B12, folate, thiamine); and a miscellaneous category (arthritis, hepatitis, vitiligo). Drugs or toxins that have been implicated include alcohol, amphetamines, cocaine, corticosteroids and ketoconazole.1
Older names (acarophobia, dermatophobia) are misleading because DP is not a phobia: patients are not scared of insects or micro-organisms, and do not recognise their disorder as irrational. Primary DP is a delusional disorder of the somatic type in which the person has a fixed belief in some physical defect or medical condition. This distinguishes it from persecutory or grandiose delusional disorders.1 It is a monosymptomatic hypochondriacal psychosis, where a fixed belief exists without other thought disorders. Patients do not meet the criteria for mood disorder or schizophrenia, although tactile and olfactory hallucinations related to the specific delusion may be present. Depression and anxiety may occur, secondary to the delusional illness. Persons with primary DP have otherwise generally normal mental function and behaviour, and delusions are limited in scope and effect on their lives. The underlying cause is unknown, but in susceptible individuals certain symptoms are amplified and perpetuated by new knowledge, interest or publicity.1 A self-perpetuating cycle of increasing belief in their own 'disease' becomes established, exacerbated by the anxiety this engenders. The pathophysiology may involve abnormal dopamine levels in the brain's corpus striatum.2
Clinical presentation
Typically, patients appear outwardly normal until they elaborate their beliefs (Table I). Most are middle-aged women (the female-to-male ratio is about 2 - 3:1, but 1.4:1 for those aged less than 50 years), and often well educated; social isolation is frequent and may predate the onset of the disorder. Younger patients are more likely to have DP secondary to medical conditions, schizophrenia, or substance abuse.1 The delusion frequently involves skin infestation (cases 1, 2 and 3), or intestinal worms or other internal pathogens (case 4). Body openings and their surrounds are often involved. Patients may describe elaborate, unlikely life cycles and migration of organisms through the body (cases 3 and 4) and in inanimate objects or the environment (case 2). Pets may be blamed as sources of infection and be disposed of (cases 1 and 3). Patients may produce copious notes or diaries documenting their disorder. Frequently, the Internet is consulted (case 3); many websites feed their beliefs. Some propagate conspiracy theories about unseen epidemics of parasites, and naturally reinforce sufferers' delusions.
Physical symptoms may involve sensations of skin penetration or burrowing by parasites, and patients' attempts to extract them can cause skin damage and further irritation. Likewise, application of detergents and chemicals (astringents, bleach, pesticides, paraffin, and others) is damaging (cases 2 and 3). Predominance of skin involvement usually entails consultation with dermatologists, among other specialists. Eyes may be a focus of delusion, resulting in self-inflicted ocular damage. The patient typically describes the infection as persistent and unresponsive to numerous treatments, and frequently perceives medical practitioners to be ignorant and incompetent. Occasionally this anger has resulted in attempted murder (and in one case actual murder) of a doctor.3 Sometimes patients may endanger their own lives, illustrated by a 70-year-old man who set fire to, and subsequently flooded, his accommodation. Suicide may be attempted and sometimes achieved.
There is often a history of numerous consultations with general practitioners, dermatologists, physicians, medical microbiologists, parasitologists, and entomologists. Patients who implicate their pets may repeatedly visit veterinarians.4 Complementary or unconventional medical practitioners may be consulted (case 3). A pathognomonic sign of DP is evidence produced by the patient of the perceived pathogen, usually as small containers holding skin flakes, scabs, fluff, household debris, parts of common insects like ants or gnats, hairs, or other nonspecific material - the well-known 'matchbox' (or 'Ziploc bag') sign.
Sometimes the delusion is shared, usually by a spouse or other close family member ('folie à deux'). It may involve three persons ('folie á trois'), or more ('folie partage'). The 'inducible' nature of DP is exemplified by a report of how yak-wool sweaters, souvenirs from Nepal, triggered DP successively in family members, including relatives living apart from the primary case.5 Shared delusions occur in 5 - 15% of cases of DP; case 3 influenced her sister and work colleagues in this way. Separation from the inducer usually leads to remission.
Management
Doctors unaware of the condition are frustrated by the failure of their usual diagnostic and therapeutic approach. This perpetuates the patients' beliefs in the intractable nature of their condition, and leads to a succession of unsatisfactory consultations. The diagnosis of DP is self-evident to the knowledgeable practitioner. However, bizarre as they may seem, the patient's claims must be investigated for genuine infection or infestation, and to check for underlying disease causing secondary DP. Scabies, infections with animal or bird mites, fleas or lice, contact dermatitis, allergies, other forms of skin irritation, or, in the case of perceived internal parasites, intestinal worms, could be involved. A medical history and examination are necessary. Laboratory investigations might include skin scrapings or biopsies, a full blood count, blood chemistry, thyroid function tests, or vitamin B12 levels. Medical and psychiatric causes of secondary DP must be considered, and referral to specialist physicians, dermatologists or psychiatrists may be necessary.
Some cases of apparent DP are simple misinterpretation of circumstantial evidence. We have seen fly larvae or ants, originating in or around the urinal or toilet bowl, misunderstood as infestation of urine or stool. Undigested or transformed vegetable matter may resemble stool parasites. Specimens produced by the patient should be examined for the presence of pathogens. However, patients with genuine DP are typically not reassured by negative laboratory results, and these paradoxically reinforce their beliefs. Treatment of underlying disease - physical, psychiatric, toxic or other - frequently eliminates or ameliorates secondary DP. Entities to be distinguished from primary DP are factitial dermatitis (self-inflicted for attention-seeking), Munchausen's syndrome, and malingering.
The doctor's attitude is important in managing primary DP. Dissatisfaction and resentment characterise patients' dealings with doctors, and they fiercely reject suggestions of a psychiatric basis to their problem. The medical practitioner is advised to neither support nor contradict the patient's assertions, but strive to form a co-operative bond, understanding that their discomfort is very real to them. Confirmation of the diagnosis requires psychiatric assessment, but patients typically resist referral and often the doctor-patient relationship terminates abruptly at the suggestion. Doctors should be aware of the potential for suicidal ideation and refer urgently if required. Patients may be persuaded to accept antipsychotic medication to reduce stress and anxiety (or a 'chemical imbalance'),1 and to help them live with their condition. Pimozide (Orap) has been the most widely used antipsychotic for DP. Atypical antipsychotics such as risperidone and olanzapine appear to be as effective, and have an improved side-effect profile that promotes compliance.6
Before the advent of neuroleptic medication, DP was regarded as a progressive illness, with a small (10 - 30%) rate of spontaneous remission.1 The success rate of antipsychotic treatment ranges from 50% to 90%, inversely related to duration. Some patients respond well but never achieve full remission; in others, despite treatment, the outcome is sometimes fatal.
References
1. Suh KH, Keystone JS. Delusional parasitosis. In: Guerrant RL, Walker DH, Weller PF, eds. Tropical Infectious Diseases. Philadelphia: Elsevier, 2006: 1700-1707.
2. Huber M, Kirchler E, Karner M, Pycha R. Delusional parasitosis and the dopamine transporter. A new insight of etiology? Med Hypotheses 2007; 68: 1351-1358.
3. Bourgois ML, Duhamel P, Verdoux H. Delusional parasitosis: folie á deux and attempted murder of a family doctor. Br J Psychiatry 1992; 161: 709-711.
4. Nel M, Schoeman JP, Lobetti RG. Delusions of parasitosis in clients presenting pets for veterinary care. J S Afr Vet Assoc 2001; 72: 167-169.
5. Schwartz E, Witztum E, Mumcuoglu KY. Travel as a trigger for shared delusional parasitosis. J Travel Med 2001; 8: 26-28.
6. Wenning MT, Davy LE, Catalano G, Catalano MC. Atypical antipsychotics in the treatment of delusional parasitosis. Ann Clin Psychiatry 2003; 15: 233-239.
Accepted 27 February 2008.
- a desire to have a baby - is not supported by the fact that two-thirds of 15 - 19 and 20 - 24-year-old women who had been pregnant said that their pregnancy was unwanted. Other significant predictors of condom use, including condom self-efficacy, duration of relationship and beliefs about marriage,3 do not show enough age-specific variation to explain the decline.
The probable answer is that a significant proportion of young people succumb to a set of social constraints and expectations that prevail when they leave school. This state of limbo - described by popular rap artist Sista Bettina as living 'in the meantime' - shapes both social and sexual behaviour. To a young woman in an informal settlement, unemployed and insecure, acquiescence to immediate economic pressures and social expectations may seem rational and to be for her own good. Compliance often takes the form of partnership with a man who provides physical and material 'protection' in exchange for unprotected sex.
At some point in the lives of many young people, chronic disappointment and persistent rejection wear down their sense of 'possibility' - of life's potentials. Risky behaviour is not such a big deal, even though they've got the message. That's why young people still have unprotected sex.
A more challenging question is why people in such circumstances should not have unprotected sex. The easy answer - that there's a lot to live for - has long underpinned most approaches to risk reduction. Yet studies consistently show high levels (>90%) of optimism among South African youth - generally defined as a sense of utility in the long term, quite distinct from the pressing concerns of everyday life. Therefore an appeal to their vague sense of future beneficence is hardly compelling. They will only move out of 'the meantime' if their lives gain incremental momentum, starting now.
Interestingly, people living in rural traditional homesteads are relatively protected from HIV, compared with those in urban informal settlements.4 Poverty seems to predispose to infection in the presence of other factors such as social exclusion or family disruption. In cross-country comparisons, income polarisation emerges as a stronger determinant of HIV infection than absolute poverty.5
Most advocates of behaviour change recognise the socioeconomic drivers of HIV infection,6 and have combined local development and communication strategies in their prevention efforts. However, taking on the national burden of poverty and inequality is overwhelming, and could diffuse the focus and place even existing gains at risk.
In South Africa, inroads have been made in reducing HIV infection among teenagers, and stepping up exposure to good sexuality education will take us even further. But the spike of infection in school-leavers suggests that we will not reach the turnaround point without confronting the elephant in the road.
Possibly the most dominant effect of all - the impact of socio-economic polarisation - remains unchallenged.
One point of intervention may be the nexus between social and individual determinants of HIV infection. At some point in the chain, structural factors trigger behavioural effects. A better understanding of the psychological triggers could open new avenues for intervention. Our view is that perception of day-to-day opportunity is a pivotal mediator of structural influence on individual behaviour. Through this cognitive link, the constrained choices and sense of exclusion inherent in polarised societies predispose to higher levels of personal risk. The clincher would be strong independent associations between an individual's sense of immediate possibility, resilience and inclusion, and lower rates of HIV. Unfortunately, there are still yawning gaps in our knowledge, and this is an important area for further research.
We believe, however, that there are enough insights to suggest that changing perceptions of opportunity should be central to behavioural interventions. Some would argue that life-skills programmes do just that. To the extent that they build 'look-for-opportunity', 'get-up-and-go' and 'get-up-again' mindsets, that is true. But we also need to create pathways for young people that link them to opportunity. In this regard, new technologies such as mobile social networks could help by creating immediate and interactive access to information. (Three-quarters of 15 - 24-year-olds in informal settlements have cellphones.)
Perhaps more fundamentally, we should capitalise on the leadership of young people themselves. Too often, they are regarded merely as purveyors of the message. Yet it is these young people, drawn from marginalised communities and self-selected through service, who could create precedents and pathways for others and build solidarity at the same time. A national network of 5 000 entrepreneurial young leaders - linked to opportunities for personal growth - could create a sense of innovation in stagnating communities. It won't drive away the elephant anytime soon, but could get it moving.
References
1. Pettifor A, Rees H, Kleinschmidt I, et al. Young people's sexual health in South Africa: HIV prevalence and sexual behaviours from a nationally representative household survey. AIDS 2005; 19: 1525-1534. [ Links ]
2. Hargreaves J, Morison L, Kim J, et al. The association between school attendance, HIV infection and sexual behaviour in rural South Africa. J Epidemiol Community Health 2008; 62: 113-119. [ Links ]
3. Sayles J, Pettifor A, Wong M, et al. Factors Associated with self-efficacy for condom use and sexual negotiation among South African youth. J Acquir Immune Defic Syndr 2006; 43(2): 226-233. [ Links ]
4. Shisana O, Rehle T, Simbayi L, et al. South African National HIV Prevalence, HIV Incidence, Behaviour and Communication Survey. Cape Town: HSRC Press, 2005. [ Links ]
5. Zanakis S, Alvarez C, Li V. Socio-economic determinants of HIV/AIDS pandemic and nations efficiencies. Eur J Operat Res 2007; 176(3): 1811-1838. [ Links ]
6. Wellings K, Collumbien M, Slaymaker E, Singh S, Patel D, Bajos N. Sexual behaviour in context: a global perspective. Lancet 2006; 368: 1706-1728. [ Links ]
Accepted 13 May 2008.


{kind=link}