










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 no.9 Pretoria sep. 2008
ORIGINAL ARTICLES
Cryptococcus and lymphocytic meningitis in Botswana
Gregory P BissonI; Ramishwari ThakurII; Rob Roy MacGregorIII; John LukesIV; Isaac MtoniV
IMD, MSCE; Infectious Diseases Division, Department of Medicine, University of Pennsylvania School of Medicine, Philadelphia, PA, USA
IIPhD; Infectious Diseases Division, Department of Medicine, University of Pennsylvania School of Medicine, Philadelphia, PA, USA
IIIMD; Infectious Diseases Division, Department of Medicine, University of Pennsylvania School of Medicine, Philadelphia, PA, USA
IVBA; Department of Psychology, University of San Diego, San Diego, CA, USA
VMD; National Health Laboratory, Gaborone, Botswana
ABSTRACT
We retrospectively reviewed microbiological data from a tertiary care hospital in Botswana, and found that Cryptococcus neoformans was cultured from 15% (193/1 307) of all cerebrospinal fluid (CSF) specimens submitted for analysis, making it the most common diagnosed cause of meningitis in this population. Moreover, almost 70% of CSF samples with significant lymphocytosis did not yield a pathogen, suggesting that many causes of lymphocytic meningitis go undiagnosed.
The southern African country of Botswana (population 1.7 million) has one of the highest prevalence rates of HIV infection in Africa (37% of pregnant women 15 - 49 years old).1 Many patients admitted to the 500-bed tertiary care Princess Marina Hospital (PMH) in the capital city of Gaborone carry the presumptive diagnosis of meningitis, and more than 100 per month have CSF submitted for analysis. Since 2001, the Infectious Diseases Division of the University of Pennsylvania School of Medicine has been mentoring in the Botswana National HIV Treatment Programme as well as assisting with in-patient care and teaching at PMH. Because of the frequency of presumptive meningitis, we reviewed results of CSF cultures and cell analyses from all specimens sent to the hospital's microbiology laboratory during calendar year 2003. We report a high burden of disease due to cryptococcal meningitis as well as lymphocytic inflammatory exudates without bacterial or fungal growth.
A total of 1 307 CSF specimens were submitted to the laboratory in 2003. All were cultured for bacteria on sheep blood, MacConkey, and chocolate agar plates, and for fungi on Sabouraud's agar. If requested by the submitting physician, specimens were forwarded to the nearby Centres for Disease Control and Prevention (CDC)-affiliated National Tuberculosis Laboratory for acid-fast bacillus (AFB) smear examination only. Generally, bacterial and fungal cultures were incubated for 2 days; all were examined by Gram staining and by India ink microscopy. Cryptococcal antigen analysis was not available at PMH in 2003. For our retrospective review, we could not retrieve CSF total protein and glucose results to link with culture results. We reviewed and tallied the cellular composition of specimens if they contained >5 cells/ul or if they were culture-positive.
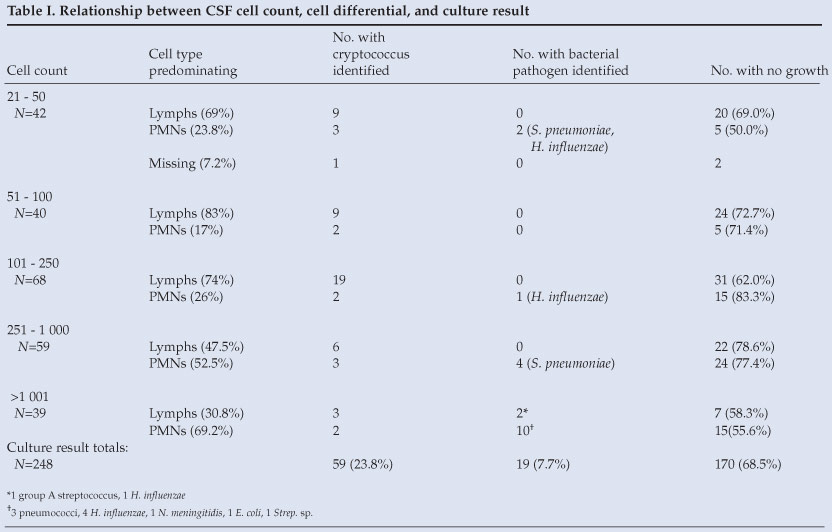
Cryptococcus neoformans was cultured from 15% of all specimens (193/1 307); 183 of 193 (95%) of those were India ink-positive. No leucocytes were present on CSF microscopy in 31% of cryptococcal cases, and an additional 23% had 1 - 10 leucocytes/ul. Therefore, over half of the cryptococcal meningitis cases had 10 or fewer cells in CSF. Conversely, 7.3% of the cryptococcal-positive cases showed >250 cells/ul in CSF and, surprisingly, a third of those (5/14) had predominantly (>50%) polymorphonuclear leucocytes (PMNs) (Table I).
Bacteria were cultured from only 23/1 307 specimens (1.8%), including 11 S. pneumoniae, 6 H. influenzae, 3 gram-negative bacilli, 2 streptococcal species, and 1 N. meningitidis. Four (17%) of the 23 isolates were from paediatric patients. Nineteen of the 23 cases (83%) had white blood cell counts >20/ul, most with a PMN predominance (Table I). It is possible that additional cases were not detected because of antibacterial treatment prior to the lumbar puncture, particularly for the 68% of cases that had >250 PMNs but failed to grow on culture (Table I).
Mycobacterial cultures were not performed on any specimens in 2003. Acid-fast smears were performed on 129 specimens; 2 were positive.
Analysis of the cellular profile of CSF was of interest. Only 27% in the 11 - 20-cell range had differentials performed, so this range was deemed uninterpretable. However, most specimens with >20 cells/ul (248) did have differential counts available (Table I). Sixty per cent of these (150) had lymphocyte-predominant exudates; 31% of these (46) grew cryptococcus; 2 were contaminated; 2 were AFB-smear positive; and the remainder (69%) were culture-negative. Therefore, a major proportion of lymphocytic meningitis in Botswana remains without a specific microbiological diagnosis.
Discussion
Three striking facts emerged from our analysis. Firstly, the burden of cryptococcal meningitis in this high HIV-prevalence country is staggering: 15% of all CSF specimens cultured in 2003 grew cryptococcus and, because cultures were usually discarded after 48 hours' incubation, the true frequency could have been even higher with longer incubation.2 Cryptococcus was found almost 10 times as often as were any bacteria, and accounted for 89% of all of the microbiological diagnoses. This finding underscores the importance of maintaining adequate supplies of amphotericin B and fluconazole in hospitals in southern Africa, where the burden of HIV/AIDS is greatest and resource limitations are severe. Secondly, we confirmed prior reports of low to no CSF inflammatory cells in some AIDS patients with cryptococcal CSF infections.3 A third of the culture-positive cases had <5 leukocytes in the CSF, and 54% had <10 cells; therefore, a very low or negative CSF cell count is no indication that cryptococcal infection is unlikely. Thirdly, almost 70% of CSF specimens with significant lymphocytosis (>20 lymphocytes/ul) did not yield a pathogen. Several reasons for this anomaly seem possible: some of these specimens could have contained cryptococci that required >48 hours to demonstrate growth; recent experience in the laboratory has shown that an additional 12% of cryptococcal isolates will be found only when cultures are incubated for 7 days. Tuberculosis is another likely cause for some of the culture-negative lymphocytic meningitis because tuberculosis is highly prevalent in this AIDS-afflicted population.4 Acid-fast smearswere positive in only 2 out of 129 CSF specimens assessed. Because the AFB smear is an insensitive tool for diagnosing tuberculous meningitis,5 we recently sent 67 CSF specimens away for smear and culture testing; none was smear-positive, and 1 grew M. tuberculosis. The actual incidence of TB meningitis among the remaining lymphocyte-predominant meningitis cases is unknown but appeared to be no more than 50%, based on clinical course. Other possible aetiologies for the remaining lymphocytic meningitis cases include T. pallidum, enteroviruses, mumps, arboviruses, acute HIV, and others.
We are planning a comprehensive prospective study to further research the range of agents causing lymphocytic meningitis in Botswana.
References
1. Botswana Central Statistics Office, National AIDS Coordinating Agency (Botswana). The Botswana AIDS impact survey II, 2004. Gaborone: Central Statistics Office, Department of Print and Publishing Services, 2005. [ Links ]
2. Casadevall A, Perfect JR. Cryptococcus neoformans. Washington, DC: ASM Press, 1998. [ Links ]
3. van der Horst CM, Saag MS, Cloud GA, et al. Treatment of cryptococcal meningitis associated with the acquired immunodeficiency syndrome. NIAID Mycoses Study Group and AIDS Clinical Trials Group. N Engl J Med 1997; 337: 15-21. [ Links ]
4. Nelson LJ, Talbot EA, Mwasekaga MJ, et al. Antituberculosis drug resistance and anonymous HIV surveillance in tuberculosis patients in Botswana, 2002. Lancet 2005; 366: 488-490. [ Links ]
5. Nguyen LN, Kox LF, Pham LD, Kuijper S, Kolk AH. The potential contribution of the polymerase chain reaction to the diagnosis of tuberculous meningitis. Arch Neurol 1996; 53: 771-776. [ Links ]
 Correspondence:
Correspondence:
G Bisson
(bisson@mail.med.upenn.edu)


{kind=link}