










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 no.9 Pretoria sep. 2008
ORIGINAL ARTICLES
Otosclerosis and TGF-β1 gene in black South Africans
M TshifularoI; C A JosephII
IMB BCh, MMed (ORL), FCS (ORL); ENT Department, University of Pretoria
IIMB ChB, MMed, FRCS, FCS; ENT Department, University of Limpopo (Medunsa campus), Pretoria
ABSTRACT
Limited literature is available on the epidemiology and genetics of otosclerosis in South African blacks, among whom it is extremely rare. We undertook this study because we had documented and surgically confirmed cases of clinical oval window otosclerosis in this population.
Otosclerosis is a spongifying disease of the labyrinthine capsule of unknown aetiology that occurs only in humans.1,2 It affects the temporal bone, a focus of bone resorption and reactive bone formation developing into otospongiotic weak bone.1,2 The prevalence of clinical otosclerosis is 0.3 - 0.4% in adult Caucasians2 and is low among Japanese, Chinese, Indonesians and American Indians,3 while the condition is extremely rare in blacks.1,3,4 It is one of the most common causes of progressive conductive hearing loss among adult Caucasians.4 Theories about the aetiology of otosclerosis have been postulated but, despite extensive research, its origin remains unclear.1
Genetically, otosclerosis is considered to be a multifactorial and complex disease.1,2,5 During the embryonic formation of the otic capsule, is considered to be a regulatory molecule that is important in the epithelial-mesenchymal interactions and epithelial induction of the chondrogenesis.5,6 It is expressed in otosclerosis specimens of adult human bone consisting of stapedial footplate, suggestive of its role in bone turnover and remodelling in otosclerosis.6-8
Given the rarity of otosclerosis among blacks, we aimed to define its clinical presentation, diagnosis and genetics in black South Africans. We hypothesised that the clinical presentation would be similar to that in other races and that the TGF-|31 protective gene might play a role in its low incidence among blacks.
Patients and methods
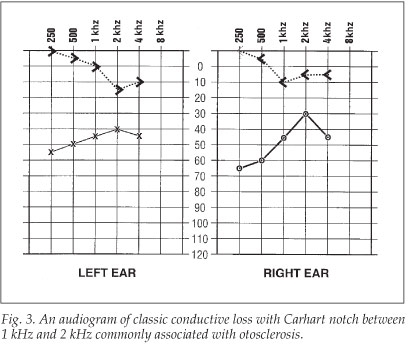
Cases from January 1993 to December 2006 were compiled from the clinical records of ENT departments at three South African universities and academic hospitals. All patients fulfilling the inclusion criteria of being indigenous black South Africans with progressive painless conductive hearing loss without infection or trauma, normal tympanic membrane and the presence of a Carhart notch on the audiogram, were included. Clinical information was obtained from the patients' charts and any clinical communication available. Information regarding clinical presentation, demography, family history, audiometric data, operation reports and laboratory results was recorded. Audiograms were analysed based on age and sex-dependent audiometric curves according to International Organization for Standardization (ISO) standard 7029. Surgical and histological reports for all patients considered to be affected clinically were checked for confirmation.
Genomic study
The genetic analysis was done on 116 DNA specimens obtained from black South Africans. In 10 patients with clinical otosclerosis and 106 controls, DNA was extracted from whole blood. The single nucleotide polymorph (SNP) primers were designed from intronic sequences flanking exons 1, 5 and 6 of TGF-P1 (rs1800472). Direct sequencing of the polymerase chain reaction (PCR) products was performed.
Results
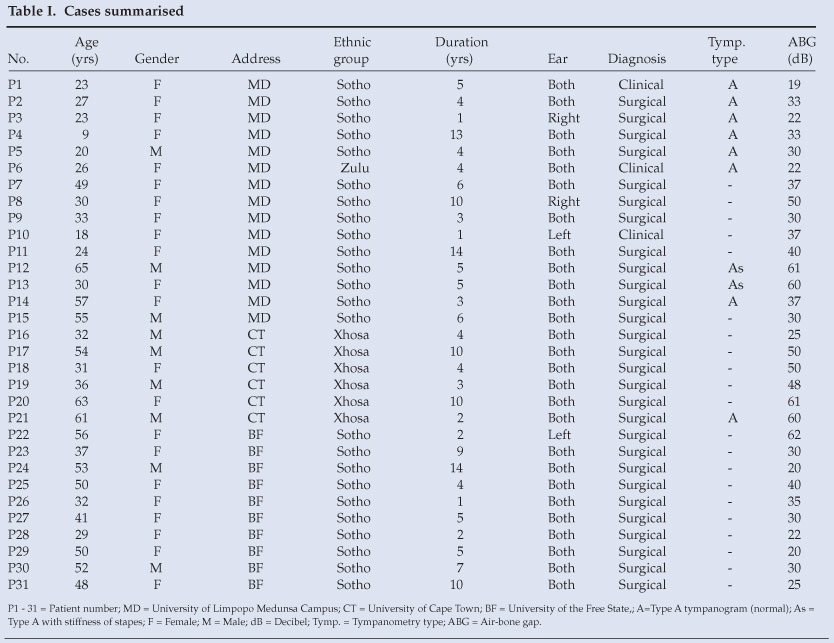
Our study included a total of 31 patients with clinical otosclerosis (Table I). Ages ranged from 9 to 65 years; there were 22 (71%) females and 9 (29%) males - a ratio of approximately 2:1 (Fig. 1). The mean age of onset was 41 years (females 36 years; males 45 years). They comprised several South African ethnic groups (Fig. 2): 24 (77%) Sotho, 7 Nguni, 6 Xhosa and 1 Zulu. Ten female patients had been pregnant (average of 1.2 pregnancies), and all of them indicated that pregnancy and the first symptom and presentation of otosclerosis were concurrent. The average duration of illness before presentation ranged from 1 to 14 years, with a mean of 6 years. No patients had a family history of clinical otosclerosis.

Presentation was bilateral in 27 (87%) and unilateral in 4 (12%) patients. The average air-bone gap on presentation ranged from 19 to 62 dB with a mean of 40.3 dB (Fig. 3). Most patients presented with moderate hearing loss. Tympanometric findings, recorded in 10 patients, showed type A compliance in 8 patients and type As in 2.
Clinical otosclerosis on history and presence of a Carhart notch had a 100% surgical correlation of oval window ankylosis (stapes footplate fixation) in 28 (90.3%) patients. Histological evaluation of stapes specimens confirmed otosclerosis as a cause of ankylosis (Fig. 4). Information on operative complications was not available. Patients fitted with prostheses after stapedectomy or stapedotomy were satisfied with the outcome and hearing benefit. One patient used a hearing aid because she was reluctant to have surgery. Two patients (6.5%) were satisfied with their hearing levels and opted for no treatment. No patients were on medical treatment with fluoride.

A genetic study of 116 DNA specimens was undertaken. Sequencing of the SNPs (1+2), (4+5) and (6) on 10 patients and controls was done, looking for polymorphism or mutations on T263I gene associated with TGF-P1. We found that the protective haplotype SNP4-rs1800472, T263I found in European (Belgian-Dutch and French) populations as a protective gene and SNP6-rs8179181 were not polymorphs in the South African black population. However, a rare coding polymorphism on control ZAP-C 100:892 C-T at Exon6 was changing the codon CTG into TTG, coding for the amino acid leucine on position 298. This SNP is a polymorph in the South African black population but very rare in the European population. There were two SNPs at SNP2-rs1982073 at Exon1 and SNP3-rs1800471 at Exon1 which were also polymorphs in the South African black population but very rare in the European population.
Discussion
There is a relationship between race and the incidence of otosclerosis,1,3,4,6,8-10 which has been estimated to be about 7 times less common among African-American blacks than among Caucasians in the USA, and to be extremely rare or non-existent among South African blacks.3,5,6,8 Our study of 31 South African black patients confirms that otosclerosis exists, although it is extremely rare;5 its incidence is not yet known. Ethnic groups affected were 24 (77.4%) Sotho, 6 (19.4%) Xhosa, 1 (3.2%) Zulu and no others. Whether ethnic differences contribute to the causation of otosclerosis in this population or is an incidental finding needs to be clarified. The ages of presentation are in keeping with other studies.1,3,4,9,10 Otosclerosis usually presents at around 15 - 45 years of age but can present earlier. The female:male ratio of about 2:1 is in keeping with other reports.7,11,12 Females present earlier than males. The average duration of illness before presentation ranged from to 1 - 14 years, with a mean duration of 6 years. In keeping with the literature of a negative family history in 50% and variable penetrance of 40%, all patients had a negative family history of otosclerosis. Cases among blacks seem to be sporadic.1,6,10
Of our patients, 27 (87%) had bilateral and 4 (12%) unilateral disease (p<0.05). In other reports, more than 85% of patients had bilateral disease.1,3,4,7,12 There was no significant statistical difference in severity between the left (16 - 51.6%) and the right ears (14 - 48.4%). The average air-bone gap on presentation ranged from 19 dB to 62 dB with a mean of 40.3 dB, in keeping with other studies.1,3,4 Most patients presented with conductive hearing loss. The compliance in matured otosclerosis is type As.1,9,10 Of the 31 patients with a clinical diagnosis of otosclerosis, 28 (90.3%) had a 100% correlation of oval window ankylosis (stapes footplate fixation) on exploratory tympanotomy. Patients were satisfied with the outcome and hearing benefits of stapedectomy or stapedotomy which, in experienced hands and appropriate patient selection, is safe and effective, with a success rate of more than 90%.1,3,7,11,12 The finding in this genetic study of polymorphisms associated with TGF-P1 among South African blacks but which are different to the European population may be because otosclerosis is a complex functional gene condition.5
Otosclerosis can be considered as a complex disease with relatively common monogenic forms. Knowledge of these genes could lead to substantial improvements in our ability to diagnose, and possibly even prevent or treat, this type of hearing loss.2,5,8,13
We thank the patients, families and participants; the ENT departments of the University of Limpopo (Medunsa), University of Cape Town (Dr M Young), University of the Free State (Prof. A Claassen and Dr K Seedat) and University of the Witwatersrand (National Health Laboratory Service) (Prof. M Ramsy and the team) for DNA extraction; collaborators Prof. Guy van Camp and Ms M Thys from Antwerp University, Belgium, for genetic studies; and GlaxoSmithKline and the European Union (EU) for funding.
References
1. Tshifularo MI, Joseph CA. Otosclerosis among South African indigenous blacks. East Afr Med J 2005; 82(5): 223-225. [ Links ]
2. Moumoulidis I, Axon P, Baguley D, Reid E. A review on the genetics of otosclerosis. Clin Otolaryngol 2007; 32(4): 239-247. [ Links ]
3. Altman F, Glasgold A, McDuh JP. The incidence of otosclerosis as related to race and sex. Ann Otol Rhinol Laryngol 1967; 76: 377-392. [ Links ]
4. Guild SR. Histological otosclerosis. Ann Otol Rhinol Laryngol 1944; 53: 246-266. [ Links ]
5. Thys M, Schrauwen I, Vanderstraeten K, et al. The coding polymorphism T263I in TGF-/Ï1 is associated with otosclerosis in two independent populations. Hum Mol Genet 2007; 17: 2021-2030. [ Links ]
6. Tshifularo MI. Clinical case presentation on otosclerosis in SA blacks. Geneeskunde 1998; 42: 2-5. [ Links ]
7. Tato JM, Tato JM Jr. Otosclerosis and races. Ann Otol Rhinol Laryngol 1967; 76: 1018-1025. [ Links ]
8. Van Den Bogaert K, Govaerts PJ, Schattenman I. A second gene for otosclerosis, OTSC 2, maps to chromosome 7q34-36. Am Hum Genet 2001; 68: 495-500. [ Links ]
9. Morrison AW. Genetic factors in otosclerosis. Ann R Coll Surg Engl 1976; 41: 202-237. [ Links ]
10. Arnold W, Friedmann J. Otosclerosis: An inflammatory disease of the otic capsule of viral etiology. J Laryngol Otol 1988; 102: 861-865. [ Links ]
11. Brobby GW. Two cases of otosclerosis in Kumasi, Ghana, case report. Trop Geogr Med 1986; 38: 292-295. [ Links ]
12. Gordon MA. The genetics of otosclerosis: a review. Am J Otolaryngol 1989; 10 (6): 426-438. [ Links ]
13. Van Den Bogaert K, De Leenheer EMR, Chen W, et al. A fifth locus for otosclerosis, OTSC5, maps to chromosome 3q22-24. J Med Genet 2004; 41: 450-453. [ Links ]
 Correspondence:
Correspondence:
M Tshifularo
(tshifularom@surgeon.co.za)
Accepted 15 February 2008


{kind=link}