










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 n.8 Pretoria Aug. 2008
SCIENTIFIC LETTERS
Oral fluid detection of hepatitis B vaccine-induced antibodies can improve vaccination programmes
Rosemary J BurnettI; Omphile E SimaniII; Guido FrançoisIII; André MeheusIV; Herbert R BasetseV; M Jeffrey MphahleleVI
IMPH; HIV and Hepatitis Research Unit, Department of Virology, University of Limpopo, Medunsa Campus, Pretoria
IIMSc; HIV and Hepatitis Research Unit, Department of Virology, University of Limpopo, Medunsa Campus, Pretoria
IIIMSc, PhD; Department of Epidemiology and Social Medicine, University of Antwerpen, Belgium
IVMD, PhD; Department of Epidemiology and Social Medicine, University of Antwerpen, Belgium
VDTech; National Health Laboratory Service, Dr George Mukhari Tertiary Laboratory, Department of Virology, University of Limpopo, Medunsa Campus
VIMSc, PhD; HIV and Hepatitis Research Unit and National Health Laboratory Service, Dr George Mukhari Tertiary Laboratory, Department of Virology, University of Limpopo, Medunsa Campus
To the Editor: About 387 million people (over 5% of the global population) are chronically infected with the hepatitis B virus (HBV).1 The World Health Organization (WHO) plans to contain the burden of HBV infections by means of universal vaccination programmes for infants and adolescents. The vaccine may be almost universally available to children within the next few years.2 A major drawback of monitoring immunity to the hepatitis B vaccine or HBV infection is the need for a blood specimen to detect hepatitis B surface antibodies (anti-HBs). Collecting blood is by needle, and is often painful and traumatic for babies, children and adults with poor venous access, so non-invasive sampling would be an ideal alternative.
Several oral fluid collection devices exist.3-7 The OraSure (OraSure Technologies Inc., USA), a non-invasive cotton pad impregnated with gelatine, salts (sodium chloride, citric acid, sodium benzoate, potassium sorbate, and sodium hydroxide to give pH 6.5) and deionised water is approved for use in humans by the USA's Food and Drug Administration (FDA) and is licensed for collection of oral mucosal transudate (OMT) for anti-HIV testing.8 As OMT is a serous fluid rich in immunoglubulins (IgG, IgM and IgA), it is possible to test for antibodies induced by infections of public health importance such as hepatitis A virus (HAV), HBV, hepatitis C virus (HCV),7,9,10 human papillomavirus type 1611 and many others.6 Samples can also be used to investigate the presence of hepatitis B surface antigen.12
We aimed to assess the OraSure device for collection of OMT samples; modify a serum-based commercial enzyme-linked immunosorbent assay (ELISA) kit (Murex anti-HBs ELISA, Murex Biotech Limited) for the detection of anti-HBs from OMT specimens; and evaluate the suitability of OMT as an alternative to blood for detecting anti-HBs induced by the hepatitis B vaccine.
Methods
A total of 67 paired serum and OMT specimens were collected from vaccinated health care workers (HCWs) at Dr George Mukhari Hospital, Medunsa complex. In addition, 5 HCWs previously identified as having undetectable anti-HBs despite hepatitis B vaccination were used as negative controls. An OMT sample and <3 ml of blood (using a 5 ml syringe and Vacutainer tubes) were collected after obtaining consent from each HCW. Blood samples were collected, processed and stored as previously described.13 To obtain OMT samples, the OraSure pad was placed for 2 minutes between the lower gum and inner cheek. The osmotic action of the pad draws antibodies from the mucosal tissues. Antibodies move from the capillaries to interstitial fluid and across the mucosa. The collection device is immediately placed into a preservative solution, where it remains stable for up to 21 days when stored at 20 - 37°C, or at room temperature. All serum specimens were tested for anti-HBs with automated AUSAB IMx assay13 and manual Murex anti-HBs ELISA, following manufacturers' instructions. The OMT specimens were tested only with Murex ELISA, after in-house experiments to modify and optimise the assay for detection of antibodies from oral fluid (results not shown).
Results
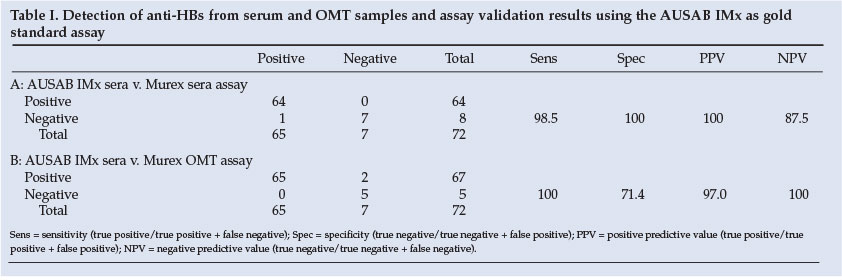
The AUSAB IMx assay (used as the gold standard) accurately determines anti-HBs to approximately 1 mIU/ml. Using this assay, the sera of 65 (97.0%) of 67 hepatitis B-vaccinated HCWs were found to be anti-HBs positive, and 2 (3.0%) were anti-HBs negative (Table I). None of the 5 controls tested positive for anti-HBs with AUSAB IMx assay. Testing with the AUSAB IMx assay therefore identified 65 seropositive for anti-HBs, and 7 negatives. The 65 anti-HBs positives had anti-HBs titres ranging from 1.2 to >1 000 mIU/ml.
The anti-HBs results from the AUSAB IMx assay were compared with those obtained from the serum samples tested with Murex anti-HBs ELISA (Table IA). The Murex assay detected anti-HBs in 64 (98.5%) of the 65 positive sera, and in none of the 7 negative sera, leading to one false negative (the anti-HBs titre of this sample was 1.2 mIU/ml, which was below the cut-off value (>5 mIU/ml) for the Murex assay). The Murex assay therefore yielded a sensitivity of 98.5% (i.e. 64/65) and specificity of 100% (i.e. 7/7).
The anti-HBs results from the AUSAB IMx assay were compared with the Murex ELISA on OMT samples. All 67 OMT specimens from vaccinated HCWs were reactive for anti-HBs using the Murex assay, including the 2 identified as anti-HBs negative by the AUSAB IMx assay. Therefore, the OMT-based testing resulted in 2 false positives (Table IB). However, all 5 OMT specimens from the control group were non-reactive for anti-HBs. The Murex assay on OMT samples showed a sensitivity of 100% and specificity of 71.4%.
Discussion
In keeping with previous reports,5,10 we demonstrated that anti-HBs can be detected from oral fluid. The quality of sampling is not affected by common oral pathologies, recent food intake, cigarette smoke, dentures, drugs causing dry mouth, or HIV status.14 Although different oral fluid collection devices are commercially available,3-6 a limitation is that most assays for detection of antibodies are optimised and licensed for use with blood or serum samples. Further investigations are needed to optimise the sensitivity and specificity of these assays to accurately detect and quantitatively measure antibodies from oral fluid samples. Oral diagnostic testing of antibodies is particularly attractive for epidemiological and surveillance studies in developing countries, and has been used to determine antibody status for rubella in Ethiopian children15,16 and antibodies to diphtheria-tetanus-pertussis (DTP) in British children,6 and can monitor hepatitis B immunisation programmes in babies or adolescents, as most developing countries are now introducing hepatitis B vaccine into their national immunisation programmes. Technologies such as oral diagnostic testing can enable developing countries to introduce new and under-utilised vaccines and monitor their impact with ease.
This study was supported in part by grants from the National Research Foundation and the Poliomyelitis Research Foundation (both local).
References
1. Burnett RJ, Francois G, Kew MC, et al. Hepatitis B virus and human immunodeficiency virus co-infection in sub-Saharan Africa: A call for further investigation. Liver Int 2005; 25: 1-12. [ Links ]
2. Kane MA, Brooks A. New immunization initiatives and progress toward the global control of hepatitis B. Curr Opin Infect Dis 2002; 15: 465-469. [ Links ]
3. Parry JV, Perry KR, Mortimer PP. Sensitive assays for viral antibodies in saliva: an alternative to tests on serum. Lancet 1987; 2: 72-75. [ Links ]
4. Connell JA, Parry VJ, Mortimer PP, Duncan J. Novel assay for the detection of immunoglobulin G antihuman immunodeficiency virus in untreated saliva and urine. J Med Virol 1993; 41: 159-164. [ Links ]
5. Allwright S, Bradley S, Long J, Barry J, Thornton L, Parry JV. Prevalence of antibodies to hepatitis B, hepatitis C, and HIV and risk factors in Irish prisoners: results of a national cross sectional survey. BMJ 2000; 321: 78-82. [ Links ]
6. Vyse AJ, Cohen BJ, Ramsay ME. A comparison of oral fluid collection devices for use in the surveillance of virus diseases in children. Public Health 2001; 115: 201-207. [ Links ]
7. Cameron SO, Carman WF. The use of the OraSure collection device for hepatitis testing in health care settings. J Clin Virol 2005; 34 (Suppl 1): S22-S28. [ Links ]
8. Gallo D, George JR, Fitchen JH, Goldstein AS, Hindahl MS (OraSure HIV Clinical Trials Group). Evaluation of a system using oral mucosal transudate for HIV-1 antibody screening and confirmatory testing. JAMA 1997; 277: 251-258. [ Links ]
9. Sherman KE, Creager RL, O'Brien J, Sargent S, Piacentini S, Thieme T. The use of oral fluid for hepatitis C antibody screening. Am J Gastroenterol 1994; 89: 2025-2027. [ Links ]
10. George JR, Piacentini SC, McGrath BA, Bodin GF, Kenny CA. Diagnosis of HIV, hepatitis B, and hepatitis C in a high risk population using oral fluid. Presented at the 6th Conference on Retroviruses and Opportunistic Infections, Chicago, Illinois, 31 Jan - 4 Feb 1999. [ Links ]
11. Marais DJ, Best JM, Rose RC, et al. Oral antibodies to human papillomavirus type 16 in women with cervical neoplasia. J Med Virol 2001; 65: 149-154. [ Links ]
12. Hutse V, Verhaegen E, De Cock L, et al. Oral fluid as a medium for the detection of hepatitis B surface antigen. J Med Virol 2005; 77: 53-56. [ Links ]
13. Tsebe KV, Burnett RJ, Hlungwani NP, Sibara MM, Venter PA, Mphahlele MJ. The first five years of universal hepatitis B vaccination in South Africa: evidence for elimination of HBsAg carriage in under-5-year-olds. Vaccine 2001; 19(28-29): 3919-3926. [ Links ]
14. Ferri RS. Oral mucosal transudate testing for HIV-1 antibodies: a clinical update. J Assoc Nurses AIDS Care 1998; 9: 68-72. [ Links ]
15. Nokes DJ, Enquselassie F, Vyse A, Nigatu W, Cutts FT, Brown DW. An evaluation of oral-fluid collection devices for the determination of rubella antibody status in a rural Ethiopian community. Trans R Soc Trop Med Hyg 1998; 92: 679-685. [ Links ]
16. Nokes DJ, Enquselassie F, Nigatu W, et al. Has oral fluid the potential to replace serum for the evaluation of population immunity levels? A study of measles, rubella and hepatitis B in rural Ethiopia. Bull World Health Organ 2001; 79: 588-595. [ Links ]
 Correspondence:
Correspondence:
M J Mphahlele
(jmphahlele@medunsa.ac.za)
Accepted 10 April 2008.


{kind=link}