










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 n.8 Pretoria Aug. 2008
FORUM
ISSUES IN PUBLIC HEALTH
Emergence of extensive drug resistance (XDR) among Gram-negative bacilli in South Africa looms nearer
Adrian Brink; Charles Feldman; Guy Richards; Johan Moolman; Marthinus Senekal
Department of Clinical Microbiology, Ampath National Laboratory Services, Milpark Hospital, Johannesburg; the Division of Pulmonology, Department of Medicine, Johannesburg Hospital and University of the Witwatersrand, Johannesburg; the Department of Intensive Care, Johannesburg Hospital and University of the Witwatersrand, Johannesburg; Lancet Laboratories, Pretoria; and Pathcare, Cape Town
Until recently, the term 'extensive drug resistance' (XDR) was held to be applicable to Mycobacterium tuberculosis only. It is now clear that Gram-negative bacilli are moving a step closer towards acquiring similar resistance. The emergence of multi-(MDR) and pan-drug resistant (PDR) Gram-negative health care-associated pathogens has been confined to non-fermenters such as Pseudomonas aeruginosa and Acinetobacter baumannii. However, increasing reports of infections due to XDR fermentative Enterobacteriaceae such as Klebsiella pneumoniae, Escherichia coli, Enterobacter spp. and even Salmonella spp. support the notion that '... MDR, XDR and PDR Gram-negative fermenters might become our worst nightmare'.1-5
The proposed definitions are as follows:
MDR: resistance to 3 or more of the following 8 classes:
- anti-pseudomonal cephalosporins (ceftazidime and cefepime)
- carbapenems (ertapenem, imipenem and meropenem)
- beta-lactam/β-lactamase inhibitor combination (piperacillin/tazobactam)
- fluoroquinolones (ciprofloxacin or levofloxacin)
- aminoglycosides (amikacin, gentamicin and tobramycin)
- aztreonam
- polymyxin E
- tigecycline (Wyeth, filed for registration in South Africa).
XDR: susceptibility to 2 or less classes.
PDR: diminished susceptibility to all classes (no options for treatment).
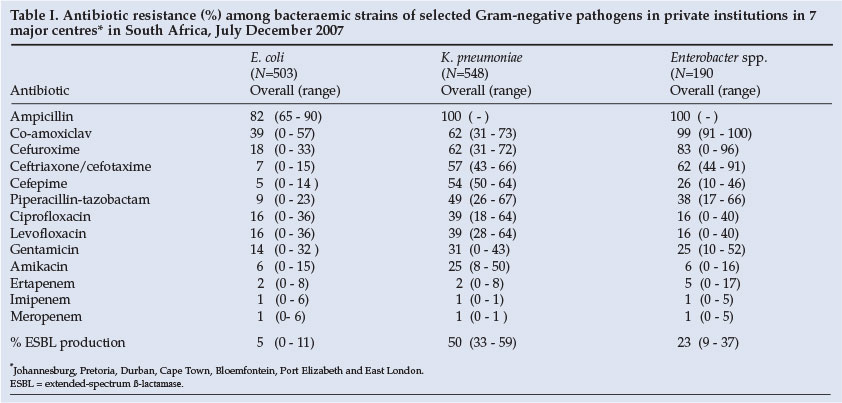
The National Antibiotic Surveillance Forum (NASF) has previously reported extremely high rates of antibiotic resistance among selected pathogens isolated from blood cultures in private institutions in South Africa.6 This report documents these new developments, particularly with regard to susceptibilities of invasive strains of the fermentative Gram-negatives, K. pneumoniae, E. coli and Enterobacter species, isolated from patients in all private institutions in seven major centres in South Africa.
Methods and results
The methods employed were similar to those described previously.6 The study was conducted from 1 July 2007 to 31 December 2007. Over this period, a total of 1 241 blood culture isolates were tested; E. coli (N=503), K. pneumoniae (N=548) and Enterobacter spp. (N=190). The resistance profiles of these strains are depicted in Table I.
Discussion
The study highlights the following:
- The high levels of resistance to key 'workhorse' Gram-negative antibiotics used in the hospitals studied
- The significant prevalence of broad-spectrum antibiotic-inactivating enzymes, in particular extended-spectrum β-lactamases (ESBLs) in some centres, and other resistance mechanisms affecting fluoroquinolones and aminoglycosides in strains of invasive Enterobacteriaceae
- The considerable differences in the prevalence of resistance and ESBL production between the various centres. This emphasises the need for routine antimicrobial surveillance at least at regional level, and preferably at each hospital or even each unit. The concept of 'know your bugs' has never been as crucial to guiding and optimising empirical treatment for bacteraemic infections as it is now.
Extensive drug resistance among these species can be conferred by several resistance mechanisms:
- Carbapenemases (KPC) are β-lactamase enzymes that inactivate the carbapenems (ertapenem, imipenem and meropenem). Those that were recently described during outbreaks in New York were resistant to all β-lactams including piperacillin-tazobactam, and most were resistant to aminoglycosides and fluoroquinolones.3
- Zinc-containing enzymes called metallo-β-lactamases (MBLs) were initially thought to be specific to P. aeruginosa and found only in Japan. However, the emergence of this enzyme among fermentative Gram-negatives in Europe (in 1997 in Italy and 1998 in Portugal) has dispelled this theory. Once such strains emerge in an intensive care unit, ward or hospital, endemicity is inevitable. This was evident from an ongoing hospital outbreak in Madrid of MBL-producing XDR Enterobacteriaceae involving 4 species: K. pneumoniae, E. cloacae, E. coli and K. oxytoca.7 A recent publication from Greece has also reported an ongoing epidemic of MBL-producing K. pneumoniae in several hospitals, involving more than 50% of blood culture isolates, effectively prohibiting the use of carbapenems.8 There are no commercially available MBL inhibitors.
- In vivo development of ertapenem resistance in an XDR strain of K. pneumoniae, due to both ESBL production and porin deficiency (which elevated imipenem and meropenem minimum inhibitory concentrations (MICs) 4 - 7-fold, respectively) in a private hospital in Cape Town, was recently described.1 Two subsequent case reports by Segal et al. described a similar phenomenon at Groote Schuur Hospital (also in Cape Town), in which imipenem and meropenem MICs increased 4- and 8-fold respectively, during meropenem therapy.2 Six other clinical strains from private hospitals in Cape Town have confirmed that hyper-production of an ESBL in association with porin deficiency is one mechanism by which these pathogens may become XDR (Pathcare, unpublished data).
- Several XDR strains of K. pneumoniae have now also been isolated from patients in two private hospitals in Johannesburg (Ampath, unpublished data). The underlying mechanism(s) of resistance is under investigation.
Attributable morbidity and mortality of increasingly resistant organisms is often difficult to quantify. However, apart from the considerable impact on financial resources, clinical outcome in bacteraemic infections caused by ESBL-producing K. pneumoniae appears to be worse than that of patients with non-ESBL-producing isolates.9 Tumbarello et al. documented the 21-day mortality rate in an ESBL group to be 52% (25/48), whereas that in the non-ESBL group was 29% (29/99) (p<0.007, odds ratio (OR) 2.62).10 These results have been confirmed in a recent meta-analysis of bacteraemia caused by ESBL-producing Enterobacteriaceae by Schwaber et al. which also demonstrated an increased risk for delay in effective therapy (pooled risk ratio (RR) 5.36; 95% confidence interval (CI) 2.73 - 10.53).11 In the Spanish outbreak mentioned above, the overall mortality rate among patients infected with an MBL-harbouring organism was also very high (45%), and it was estimated that 67% of these deaths were attributable to the presence of the resistant organism.7 Reasons for the increased mortality include the increased likelihood that initial therapy would be inappropriate and that, whereas MBL- and KPC-producing organisms may appear to be susceptible to carbapenems, clinical response may be poor.12
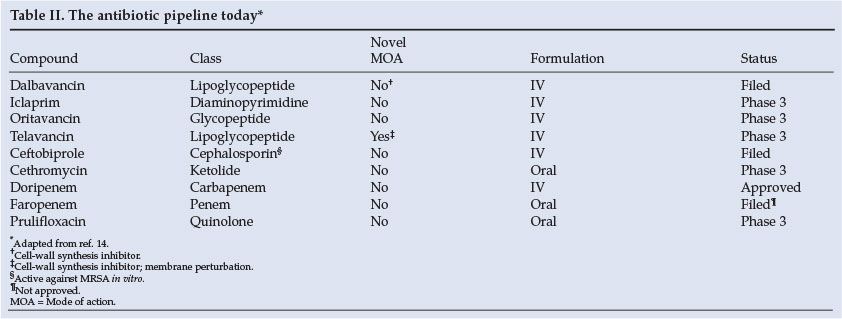
These reports are extremely disturbing; the occurrence of all such cases or outbreaks must be monitored closely. Whether salvage therapy with polymyxin E (colistin sulphate - an antibiotic emanating from the 1950s) will be an effective therapeutic option for such XDR infections, and for how long this may be so, remains to be determined. As such, not all strains of Proteus spp., Serratia spp., Morganella morganii and Providentia spp. are uniformly susceptible to polymyxin. In contrast to the relative abundance of therapeutic options for resistant Gram-positive infections (such as those caused by methicillin-resistant Staphylococcus aureus), there are no new antibiotics in development other than tigecycline for these Gram-negative infections (Table II).13,14
As recommended before,15,16 limitation of the development and spread of resistant pathogens in our institutions requires a multi-disciplinary approach, preferably involving a hospital committee to dictate:
- rigorous infection control practices
- infectious disease and clinical microbiology consultation
- active surveillance and application of molecular methods to detect epidemiological trends in mechanisms of resistance and clonal spread of such bacteria
- adequate source control
- meticulous attention to the appropriate use of antibiotics, including choice, dosage and duration of therapy
- de-escalation to narrower-spectrum antibiotics according to susceptibility.
The fact that overall antibiotic management (including prolonged duration, utilisation of multiple inappropriate or unnecessary agents, and a virtual absence of de-escalation) is suboptimal in clinical practice is evident from the nationwide results of a recent survey in academic, public and private institutions (S Bhagwanjee, personal communication) in which all of these practices were rife. In previous studies, prior exposure to antibiotics had been a common risk factor for ESBL-producing bacteria and, in this regard, the role of cephalosporins and fluoroquinolones is widely recognised (often referred to as 'collateral damage'). However, recent evidence suggests that prior use of carbapenems may also be a significant risk factor for ESBL-producing Gram-negatives in patients with bacteraemia.17 Ironically, in the NASF surveillance presented here, the carbapenems were the most active antibiotics in the majority of centres. Therefore, a formal strategic programme of sustained reduction in antibiotic consumption of all classes over the long term in hospitals nationwide, such as occurs in Sweden, is urgently warranted.18
Conclusion
As private institutions in South Africa do not employ the doctors who provide services in their hospitals, they are not able to influence prescribing habits. The fact that the antibiotic-prescribing fraternity has not yet accepted stewardship of the emerging problem of XDR Gram-negative bacilli has given rise to an ethical dilemma both in South Africa and internationally.19 To delay the imminent end of the antibiotic era, it may well be time now to challenge the right of doctors to prescribe whichever antibiotic they wish, including the dosage and duration.
Although restriction of established prescribing habits is a controversial matter, it is certain that this practice would reduce resistance levels in the community and hospitals. Similarly, punitive measures should also be instituted in an attempt to install and ingrain basic infection control practices such as hand disinfection in health care workers. Finally, ongoing training of pre- and postgraduate doctors (and nursing staff) in appropriate aspects of clinical microbiology, infection control and the principles of anti-infective use, must be mandatory.
'The die', as Julius Caesar said on crossing the Rubicon, 'is cast'. However, such is the desperate nature of the present situation that every attempt should be made to at least delay the onset of this modern plague.
Conflict of interests declaration: AB has received recent research funding from Merck and Sanofi-Aventis, served on the advisory board of MSD and Pfizer and on speakers' bureaux for AstraZeneca, Abbott Laboratories, Bayer, GlaxoSmithKline, Merck, Pfizer, Sanofi-Aventis and Wyeth pharmaceuticals. CF has received research funding from Abbott Laboratories and Sanofi-Aventis, acted on the advisory board of MSD, Abbott Laboratories and Pfizer, served as a speaker for MSD, Bayer, Abbott Laboratories, GlaxoSmithKline, AstraZeneca and Sanofi-Aventis and received funding for congress travel from Abbott Laboratories and Sanofi-Aventis. GR has served on advisory boards of MSD, Pfizer, Abbott Laboratories, Fresenius Kabi and Roche. He has received research funding from Bristol-Myers Squibb, and has served on speakers' bureaux for Merck, Sanofi-Aventis, Roche, AstraZeneca, Pfizer, Bayer, GlaxoSmithKline, Wyeth, Boehringer and Fresenius Kabi. JM served as a speaker Bayer and GlaxoSmithKline. MS has served on advisory boards of MSD, Roche and Sanofi-Aventis. He has served on speakers' bureaux for MSD, Sanofi-Aventis, Roche, AstraZeneca, Pfizer, Bayer-Schering, GlaxoSmithKline, Wyeth and Bristol-Myers Squibb.
The contributions of the following NASF members from private pathology practices are acknowledged: L Badenhorst, F Botha, M Botha, S Breuning, S Budavari, J Coetzee, M Cruz da Silva, G Elliott, M Henning, N Janse van Rensburg, S Kahn, R Loxton, L Marcus, M Mennen, N Miller, A K Peer, X Poswa, K Pillay, B Prinsloo, P Schoeman, M Senekal, J Smit, P Smith, W Swart, J van Greune, G van Greunen, C van Rensburg, M van Rensburg, O van Rensburg, J van Wyk, G Weldhagen and I Zietsman.
The NASF is supported by an unrestricted educational grant from Aspen Pharmacare, Abbott Laboratories, AstraZeneca, Bayer, Bristol-Myers Squibb, GlaxoSmithKline, MSD, Pfizer, Roche, Sanofi-Aventis and Wyeth.
1. Elliott E, Brink A, van Greune J, et al. In-vivo development of ertapenem resistance in a patient with pneumonia caused by Klebsiella pneumoniae with extended-spectrum β-lactamase. Clin Infect Dis 2006; 42: e95-98.
2. Segal H, Elisha BG. Resistance to p-lactams, and reduced susceptibility to carbapenems, in clinical isolates of Klebsiella pneumoniae due to interplay between CTX-M 15 and altered outer membrane permeability. S Afr J Epidemiol Infect 2006; 21: 41-44. [ Links ]
3. Bratu S, Brooks S, Burney S, et al. Detection and spread of Escherichia coli possessing the plasmid-borne carbapenemases KPC-2 in Brooklyn, New York. Clin Infect Dis 2007; 44: 972-975. [ Links ]
4. Miriagou V, Tzouvelekis LS, Rossiter S, et al. Imipenem resistance in a Salmonella clinical strain due to plasmid-mediated class A carbapenemase KPC-2. Antimicrob Agents Chemother 2003; 47: 1297-1300. [ Links ]
5. Hossain A, Ferraro MJ, Pino RM, et al. Plasmid-mediated carbapenem-hydrolyzing enzyme KPC-2 in an Enterobacter sp. Antimicrob Agents Chemother 2004; 48: 4438-4440. [ Links ]
6. Brink AJ, Moolman J, Cruz da Silva M, et al. Antimicrobial susceptibility profile of selected bacteraemic pathogens from private institutions in South Africa. S Afr Med J 2006; 97: 30-36. [ Links ]
7. Tato M, Coque TM, Ruiz-Garbajoza P, et al. Complex clonal and plasmid epidemiology in the first outbreak of Enterobacteriaceae infection involving VIM-1 metallo-β-lactamase in Spain: Towards endemicity. Clin Infect Dis 2007; 45: 1171-1178.
8. Psichogiou M, Tassios PT, Avlamis A, et al. Ongoing epidemic of blaViM-1_positive Klebsiella pneumoniae in Athens, Greece: a prospective survey. J Antimicrob Chemother 2008; 61: 59-63. [ Links ]
9. Giske CG, Monnet DL, Cars O, et al. Minireview: Clinical and economic impact of common multidrug-resistant Gram-negative bacilli. Antimicrob Agents Chemother 2008; 52: 813-821. [ Links ]
10. Tumbarello M, Spanu T, Sanguinetti M, et al. Bloodstream infections caused by extended-spectrum -lactamase-producing Klebsiella pneumoniae: Risk factors, molecular epidemiology, and clinical outcome. Antimicrob Agents Chemother 2006; 50: 498 - 504. [ Links ]
11. Schwaber MJ, Carmeli Y. Mortality and delay in effective therapy associated with extended-spectrum Ê-lactamase (ESBL)-production in Enterobacteriaceae bacteraemia: a systematic review and meta-analysis. J Antimicrob Chemother 2007; 60: 913-920. [ Links ]
12. Cornaglia G, Akova M, Amicosante G, et al. Metallo-p-lactamases as emerging resistance determinants in Gram-negative pathogens: open issues. Int J Antimicrob Agents 2007; 29: 380-388. [ Links ]
13. Chopra I, Schofield C, Everett M, et al. Treatment of health-care-associated infections caused by Gram-negative bacteria: a consensus statement. Lancet Infect Dis 2008; 8: 133-139. [ Links ]
14. Talbot GH, Bradley J, Gilbert D, et al. Bad bugs need drugs: An update on the development pipeline from the antimicrobial availability task force of the Infectious Diseases Society of America. Clin Infect Dis 2006; 42: 657-668. [ Links ]
15. Brink AJ. Multidrug-resistant (MDR) Gram-negative fermentors: 'Our worst nightmare?' Editorial. S Afr J Epidemiol Infect 2007; 22: 2-4. [ Links ]
16. Richards GA. The therapeutic challenge of Gram-negative sepsis: Prolonging the lifespan of a scarce resource. Clin Microbiol Infect 2005; 11(S6): 18-25. [ Links ]
17. Martinez JA, Aguilar J, Almela M, et al. Prior use of carbapenems may be a significant risk factor for extended-spectrum p-lactamase producing Escherichia coli or Klebsiella pneumoniae in patients with bacteraemia. J Antimicrob Chemother 2006; 58: 1082-1085. [ Links ]
18. Molstad S, Erntell M, Melander E, et al. Sustained reduction of antibiotic use and low bacterial resistance: 10-year follow-up of the Swedish Strama programme. Lancet Infect Dis 2008; 8: 125-132. [ Links ]
19. Delitt TH, Owens RC, McGowen JE, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 2007; 44: 159-176. [ Links ]
 Correspondence:
Correspondence:
A Brink
(brinka@ampath.co.za)


{kind=link}
{kind=link}