










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 n.5 Pretoria May. 2008
ORIGINAL ARTICLES
Association of tooth loss with hypertension
Olalekan A Ayo-YusufI; Imade J Ayo-YusufII
IBDS, MSc, MPH; Department of Community Dentistry, School of Dentistry, University of Pretoria
IIBDS, MSc; Department of Community Dentistry, School of Dentistry, University of Pretoria
ABSTRACT
OBJECTIVE: Hypertension may result from changes in dietary quality and nutrient intake. We therefore sought to determine the epidemiological association between tooth loss and hypertension in South African adults.
METHODS: This is a secondary data analysis of a cross-sectional survey of a nationally representative sample of adults aged 25 - 70 years who participated in the South African Demographic and Health Survey during 1998 (N=9 098). The primary data were collected using a validated questionnaire, which included information on past experience of tooth loss (partial or complete), use of dental services, tobacco use and other known risk factors for hypertension. Hypertension was defined as having a measured average blood pressure (BP) >160/95 mmHg and/or taking antihypertensive medication.
RESULTS: The prevalences of hypertension, any tooth loss and complete edentulousness were 18.1%, 72.2% and 9.4% respectively. Tooth loss was more common among overweight/obese respondents than among those with a normal body mass index (76.7% v. 66.7%; p<0.01). Compared with the fully dentate respondents, the completely edentulous respondents had mean systolic and diastolic BPs that were respectively 12 mmHg and 5 mmHg higher. After adjusting for known risk factors for hypertension in a multiple logistic regression model, being completely edentulous remained significantly associated with hypertension (odds ratio 1.35, 95% confidence interval 1.02 - 1.78). The estimated population-attributable fraction of hypertension resulting from complete edentulousness was 10%.
CONCLUSIONS: The findings suggest that complete edentulousness is a risk indicator for hypertension in South Africa and highlights the importance of primary care practitioner involvement in oral health promotion.
Vascular disease is a leading cause of death in developed countries and an increasingly important cause of morbidity and mortality in developing countries, including South Africa.1,2 Risk factors for vascular diseases in developing countries include smoking, diabetes mellitus, obesity, dyslipidaemia and hypertension.3,4 Studies in developed countries have suggested an association between tooth loss - an end-stage of dental and periodontal disease - and an increased risk of coronary heart disease and cerebrovascular disease.5,6 Others have failed to demonstrate any significant independent association.7
The link between tooth loss and risk of vascular disease is based on the premise that local chronic bacterial infection in the oral cavity that precedes tooth loss may influence systemic levels of inflammatory mediators. This may contribute to endothelial dysfunction, carotid artery plaque formation8 or deterioration of the anti-atherogenic potency of high-density lipoproteins.9 Another mechanism postulated is that tooth loss may affect dietary quality and nutrient intake, leading to an increased risk of vascular diseases.10 Others have suggested that the relationship between tooth loss and vascular diseases can mainly be explained by confounding factors, particularly those relating to personal health behaviour and practices.7
Studies to date have been in developed countries, and except for one,11 no earlier studies have explored the link with hypertension. The only study demonstrating an association between tooth loss and hypertension was restricted to postmenopausal women.11 Given that tooth loss may lead to dietary pattern change that may be associated with hypertension, especially among black subjects,12 hypertension might be an important risk factor linking tooth loss and vascular diseases in South Africa. We therefore sought to determine the association between tooth loss and hypertension, using a nationally representative adult sample of South Africans.
Methods
Data source and study design
The data were obtained from individuals aged 25 - 70 years who participated in the first South African Demographic and Health Survey (SADHS), a nationally representative, cross-sectional household survey conducted between February and September 1998. The 1998 SADHS used a stratified, two-staged, probability sample design. The methods used to ensure standardised data collection and interviews and consent procedures have been published.13
Cardiovascular disease risk factor assessment and definitions
The questionnaire was administered by trained and standardised fieldworkers. It included questions on the respondents' personal and family medical history, and their use of chronic medications. Interviewers listed medication containers. Other information on lifestyle and habits that was recorded included the respondents' history of tobacco and/or alcohol use and an estimation of discretionary salt usage. The respondents' smoking status and intensity were stratified according to the reported average number of cigarettes smoked per day. Fieldworkers assessed anthropometric measurements and blood pressure (BP) using methods previously detailed.13 Wealth index - a measure of socio-economic status - was derived from a composite score of a list of household items (working refrigerator, television, car, washing machine, electricity) owned by the respondents. The reliability of the scale derived was considered very satisfactory as reflected by a high internal consistency of response to scale items (Cronbach α = 0.83). The index scores were then ranked to classify the respondents into three socio-economic categories.
Hypertension was defined using the then South African hypertension guidelines (a cut-off point of 160/95 mmHg and/ or being on antihypertensive medication were used).13 This is higher than the usual cut-off point of 140/90 mmHg, but it was used in the risk estimation in this study in order to avoid over-diagnosis and misclassification of hypertensive respondents, given that all the triplicate BP measurements were taken on one occasion. This cut-off also provided some understanding of policy implications for the findings, locally. 'Dyslipidaemia' was defined as having a past history of diagnoses of high cholesterol or being on current medication for high cholesterol. Similarly, diabetes mellitus was defined as having a past history of diagnoses by health professionals of diabetes or blood sugar problems.
Dental status assessment
A person with tooth loss was defined as someone who responded in the affirmative to the question 'Have you lost any of your natural teeth?' If the respondent answered in the negative, he/she was classified as fully dentate. Partially edentulous participants were those who had lost natural teeth, but also responded in the affirmative to the question 'Do you have any of your natural teeth?'; otherwise the respondent was classified as completely edentulous. Participants were asked what they usually did to look after their teeth. Those indicating that they would visit the dentist were categorised as making preventive dental visits. Those answering 'Yes' to the question 'Do you usually brush/clean your mouth every day?' were categorised as brushing daily. The latter two responses were applied in data analysis as variables of preventive health behaviour and oral hygiene practice respectively.
Statistical analysis
Statistical analyses were done using STATA release 8 (Stata Corp., Texas, USA), with appropriate weights and design effects to produce unbiased standard errors (SE). Group differences were assessed using chi-square statistics and t-test or ANOVA for categorical and continuous variables respectively. Statistical comparisons were done between fully dentate and partially or completely edentulous respondents with regard to known vascular disease risk factors and oral hygiene behaviour (daily brushing/cleaning and preventive dental visits). Multiple logistic regression models were constructed to determine any independent association between different categories of dental status with hypertension, while adjusting for the influence of the covariates that have been identified in the literature as risk factors for hypertension and/or tooth loss. All models controlled for the age and gender of the participants regardless of the level of significance obtained in the bivariate analysis. Odd ratios (OR) with a 95% confidence interval (CI) were used in estimating the effect sizes. The level of statistical significance was set at 5%.
To illustrate the potential public health impact of tooth loss as a modifiable risk factor, population-attributable fraction or risk was calculated based on the assumptions that the associations are causal and that the prevalence odds ratios in the adjusted models approximate the true relative risks.14
Results
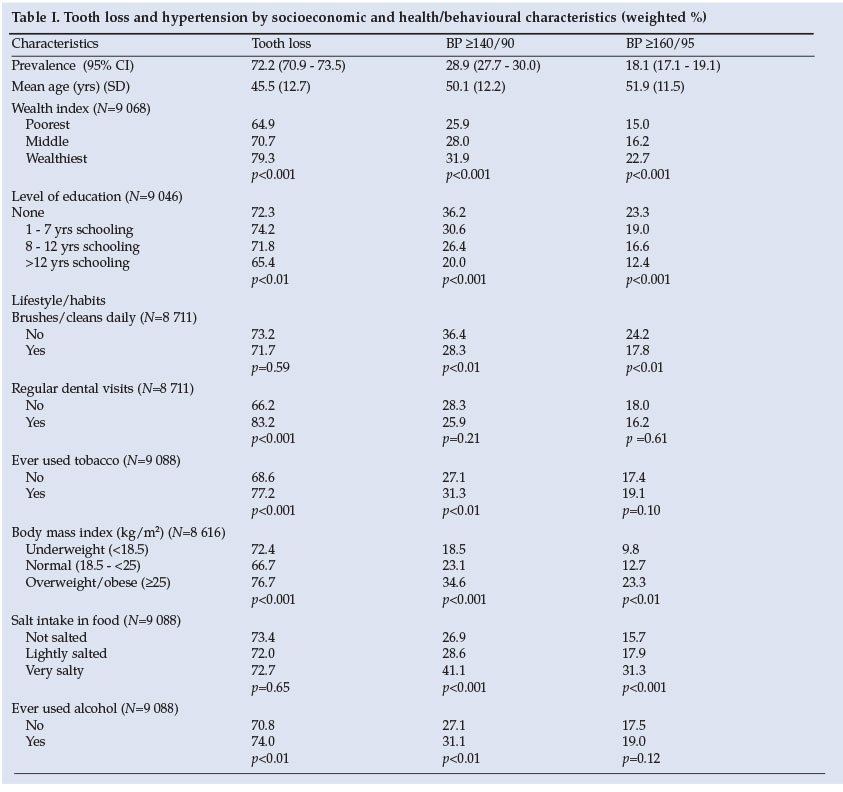
A total of 9 098 records matched the age selection criteria. Of the respondents 60.6% (N=5 470) were female and 75% (N=6 824) identified themselves as black Africans, 72.1% (N=6 560) reported that they had lost at least one tooth, and 9.4% (N=851) had experienced total tooth loss (were completely edentulous). Using the cut-off point of 160/95 mmHg, 18.1% of the respondents could be classified as hypertensive.
Respondents who were overweight/obese were more likely to be hypertensive and were also significantly more likely to have lost at least one tooth (Table I). Alcohol and tobacco use were associated with tooth loss and hypertension, albeit not at a significant level when the measure of hypertension was at the cut-off point of 160/95 mmHg. Irrespective of the measure of hypertension, affluent respondents were the most likely to be hypertensive and to have lost at least one tooth, but were less likely to be completely edentulous.
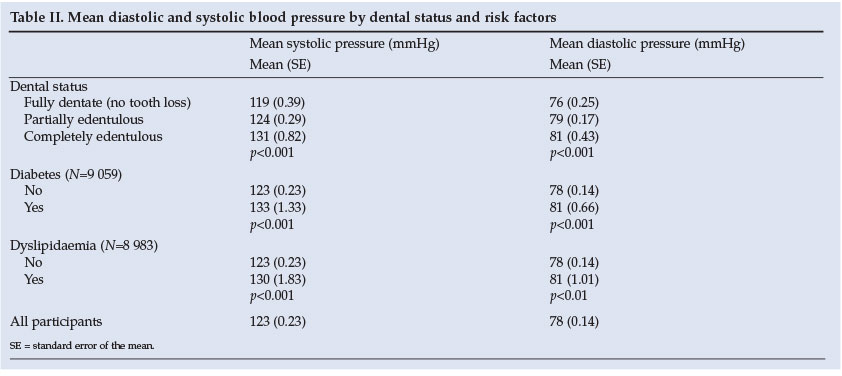
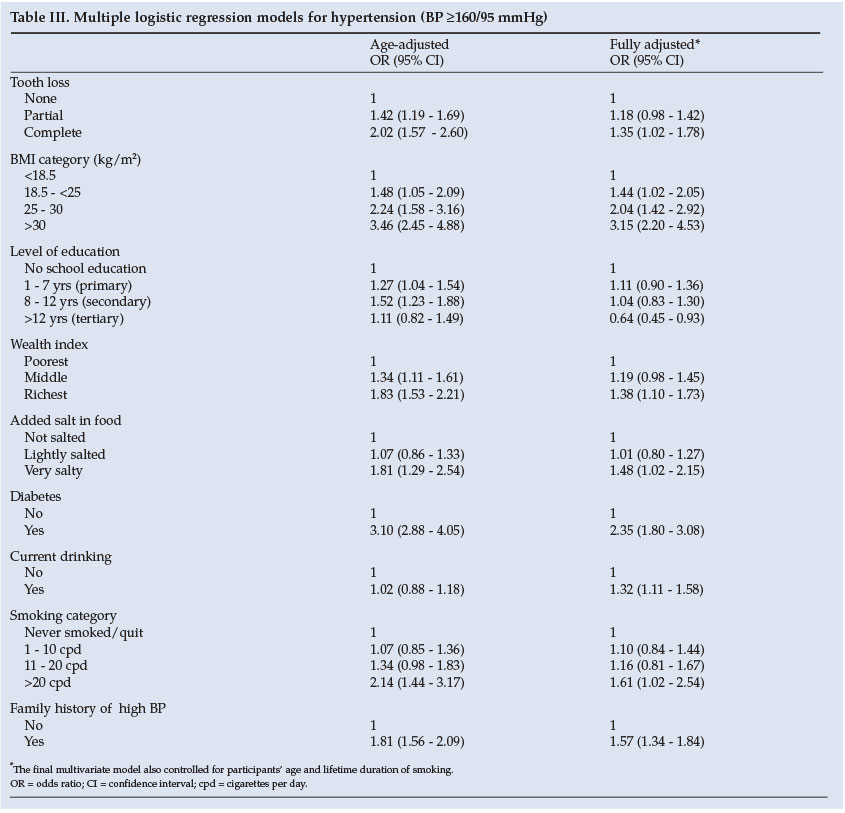
The mean diastolic BP increased with an increasing level of tooth loss. Compared with the fully dentate respondents, the completely edentulous respondents presented with mean systolic and diastolic BPs that were 12 mmHg and 5 mmHg higher respectively (Table II). After controlling for potential confounders and known risk factors, complete edentulousness but not partial edentulousness remained significantly associated with hypertension (Table III).
The estimated population-attributable fraction of hypertension resulting from complete edentulousness was 10%.
Discussion
As far as we could ascertain, this study is the first to demonstrate an association between hypertension and tooth loss in a general population. It has shown that total tooth loss or complete edentulousness, but not partial edentulousness, is a risk factor for developing hypertension. This finding may be attributable to dietary changes that could be associated with being completely edentulous,15 which may result in an increased risk of vascular disease. An association between vitamin C and folate levels and cardiovascular disease has been shown.10 The apparently graded response observed between the dental status and mean BP of the respondents in our study supports the view that nutrition or dietary pattern changes could account for the association observed between tooth loss and hypertension. Conceivably, completely edentulous subjects may not be able to consume foods as nutritious as that consumed by dentate or partially dentate subjects.
This study has confirmed the key reported traditional lifestyle factors associated with high BP in Africa.3 It confirmed the potential benefit that could be derived from dietary approaches to hypertension reduction, such as salt restriction, at a population level.12 A significant association between traditional risk factors for vascular disease, such as smoking, and an increased risk of tooth loss, was consistent with the literature.7 Being overweight or obese was associated with an increased risk of tooth loss. Given that periodontal disease is a leading cause of tooth loss in developing countries, the findings are consistent with a study that found increased upper body weight to be associated with an increased risk of periodontal disease.16 It is hypothesised that this association results from possible diminished blood flow in the periodontal blood vessels and compromise of the local host immune response in the presence of visceral fat.16 The observed relationship between body mass index and tooth loss may partly account for the observed gross attenuation of the association between hypertension and tooth loss after adjustment for several traditional risk factors. Therefore, the findings support views that the association between tooth loss and cardiovascular disease may be related to shared risk or confounding factors.7
However, the fact that total tooth loss remained significantly associated with hypertension after controlling for confounding factors supports the view that the link between tooth loss and heart disease may be related to an increased risk of hypertension. This is further supported in that total tooth loss was associated with a significant increase of 5 mmHg in mean diastolic blood pressure (DBP). A prolonged lower DBP of 5 mmHg has been associated with an at least 34% lower risk of a stroke and at least 21% lower risk of coronary heart disease.17 These figures are consistent with findings from a study of periodontal disease and tooth loss as risk factors for strokes.5
The major design limitations of this study were its cross-sectional approach and its reliance on self-reporting. Although the cross-sectional nature did not allow for the establishment of the temporal order of events, considering that the mean age of those who reported tooth loss was 5 years less than that of the respondents who reported hypertension, it is likely that tooth loss preceded hypertension in the current cohort. Furthermore, given that this was a cross-sectional study, edentulousness can only be considered a risk indicator. Consequently, edentulousness needs to be confirmed as a true risk factor in longitudinal studies that take into account the temporal order of events. Another limitation was that the level of partial tooth loss was not graded, so the 'partially edentulous' category may have lost significance as it represented too wide a range of subjects. Lastly, it may be possible that residual confounders not measured, so not adjusted for in the current model, may explain the relationship observed. Despite these limitations, this study provides, for the first time in a large national representative sample, useful information on tooth loss as a risk indicator for hypertension, while controlling for multiple risk factors.
In conclusion, this study illustrates that total tooth loss is a risk indicator for established hypertension and confirms that some traditional risk factors associated with an increase in blood pressure are also associated with the increased likelihood of tooth loss. Since the study findings suggest that 1 in 10 South African hypertensive adults could be hypertension-free if total tooth loss were eliminated, priority should be given to public health interventions to reduce tooth loss. For instance, at a primary health care level, preventive messages directed at reducing hypertension should also include how to reduce factors that may increase the risk of tooth loss, such as excessive drinking, smoking and poor oral hygiene. The importance of these factors should be emphasised in oral health promotion programmes.
Data for this study were obtained with permission from the National Department of Health through the South African Data Archives (SADA) housed at the South African National Research Foundation (NRF). The SADHS was funded by the South African National Department of Health under the co-ordination of the Medical Research Council, South Africa.
References
1. Murray CJL, Lopez AD. Mortality by cause for eight regions of the world: Global burden of disease study. Lancet 1997; 349: 1269-1276. [ Links ]
2. Bradshaw D, Schneider M, Dorrington R, Bourne DE, Laubscher R. South African cause-of-death profile in transition - 1996 and future trends. S Afr Med J 2002; 92: 618-623. [ Links ]
3. Kaufman J, Barkey N. Hypertension in Africa: an overview of prevalence rates and causal risk factors. Ethn Dis 1993; 3: suppl, S83-101. [ Links ]
4. Connor M, Rheeder P, Bryer A, et al. The South African stroke risk in general practice study S Afr Med J 2005; 95: 334-338. [ Links ]
5. Joshipura KJ, Hisn-Chia Hung, Rimm EB, Willett C, Ascherio A. Periodontal disease, tooth loss, and incidence of ischemic stroke. Stroke 2003; 34: 47-52. [ Links ]
6. Okoro CA, Balluz LS, Eke PI, et al. Tooth loss and heart disease. Am J Prev Med 2005; 29 (5S1): 50-56. [ Links ]
7. Hujoel PP, Drangsholt M, Spiekerman C, DeRouen TA. Periodontitis-systemic disease associations in the presence of smoking - causal or coincidental? Periodontology 2002; 30:51-60. [ Links ]
8. Desvarieux M, Demmer RT, Rundek T, et al. Relationship between periondontal disease, tooth loss, and carotid artery plaque: the oral infections and vascular disease epidemiology study (INVEST). Stroke 2003; 34: 2120-2125. [ Links ]
9. Pussinen PJ, Jauhiainen M, Vilkuna-Rautiainen T, et al. Periodontitis decreases the antiatherogenic potency of high density lipoprotein. J Lipid Res 2004; 45: 139-147. [ Links ]
10. Lowe G, Woodward M, Rumley A, Morrison C, Tunstall-Pedoe H, Stephen K. Total tooth loss and prevalent cardiovascular disease in men and women: possible roles of citrus fruit consumption, Vitamin C, and inflammatory and thrombotic variables. J Clin Epidemiol 2003: 56: 694-700. [ Links ]
11. Taguchi A, Mitsuhiro S, Suei Y, ef al. Tooth loss is associated with an increased risk of hypertension in postmenopausal women. Hyperfension 2004; 43:1297-1300. [ Links ]
12. Svetkey LP, Simons-Morton D, Vollmer WM, Appel LJ, Conlin PR, Ryan DH. Effects of dietary patterns on blood pressure subgroup analysis of the dietary approaches to stop hypertension (DASH) randomized clinical trial. Arch Infern Med 1999; 159: 285-293. [ Links ]
13. Steyn K, Gaziano TA, Bradshaw D, Laubscher R, Fourie J. Hypertension in South African Adults: results from the demographic and health survey, 1998. J Hyperfens 2001; 19: 1717-1725. [ Links ]
14. Kabn HA, Sempos CT. Sfafisfical Mefhods in Epidemiology. New York: Oxford University Press, 1989: 1-292. [ Links ]
15. Nowjack-Raymer RE, Sheiham A. Association of edentulism and diet and nutrition in US adults. J Denf Res 2003; 82: 123-126. [ Links ]
16. Saito T, Shimazaki Y, Koga T, Tsuzuki M, Ohshima A. relationship between upper body obesity and periodontitis. J Denf Res 2001; 80: 1631-1636. [ Links ]
17. MacMahon S, Peto R, Cutler J, ef al. Blood pressure, stroke, and coronary heart disease. Part 1: Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. lancef 1990; 335: 765 -774. [ Links ]
 Correspondence:
Correspondence:
O A Ayo-Yusuf
(lekan.ayoyusuf@up.ac.za)
Accepted 24 July 2007.


{kind=link}
{kind=link}
{kind=link}