










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 no.4 Pretoria Abr. 2008
FORUM
CLINICAL IMAGES
Progressive multifocal leucoencephalopathy - a case report
Mala Modi
Dr Modi is a senior radiologist and senior lecturer in the Department of Radiology, Chris Hani Baragwanath Hospital, Johannesburg. She is author of numerous papers in national and international peer-reviewed journals and is assistant editor of the South African Journal of Radiology.
Progressive multifocal leucoencephalopathy (PML) is a demyelinating disease caused by the human neurotropic JC (John Cunningham) virus, a polyomavirus.1,2
Following on the worldwide HIV/AIDS pandemic there has been a dramatic increase in the incidence of PML. However, cases of PML, an AIDS-defining illness, have rarely been reported from Africa, an area where HIV-1 clade C infection predominates.3-5
Clinical and imaging details
A 27-year-old woman presented to Chris Hani Baragwanath Hospital, Johannesburg, with new-onset seizures. She was heterosexual, did not abuse intravenous drugs, and was retroviral therapy-naïve. On examination in the medical ward she was found to be encephalopathic and pregnant. Further investigations revealed that she was HIV-positive with a very low CD4+ count of 7 cells/µl, and a viral load greater than 750 000 copies/ml. She was referred for imaging, and PML was diagnosed on the basis of computed tomography (CT) and magnetic resonance imaging (MRI) appearances.
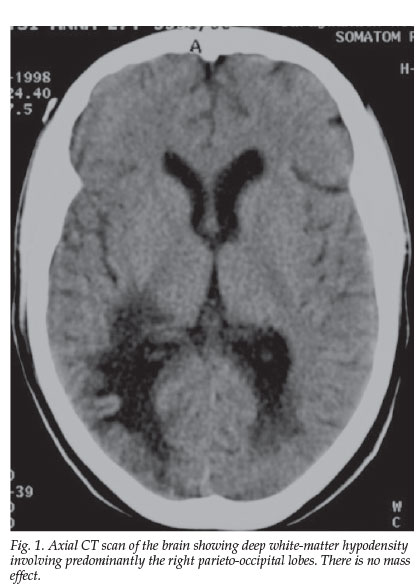
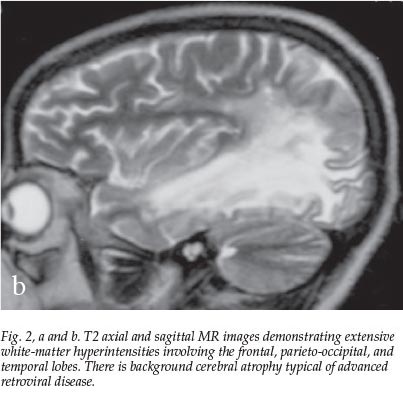
The lesions on CT imaging were typical; they were scalloped in appearance, involved the white matter of the frontal, parietal and occipital lobes, were hypodense, had no mass effect, and were non-enhancing (Fig. 1). On MRI the lesions were hypointense on T1 and hyperintense on T2-weighted MRI scans (Fig. 2, a and b).

The very low CD4+ count of 7 contributed to the diagnosis of PML. The diagnosis was confirmed on polymerase chain reaction (PCR) identification of the JC virus.
The patient died in hospital within a few days, and the diagnosis of PML was confirmed at autopsy.
Discussion
This is a rare case of autopsy-proven PML from a clade C HIV-1 infected area.6 It is pertinent to highlight this demyelinating opportunistic viral infection as access to antiretroviral therapy is currently improving, and the immune reconstitution inflammatory syndrome (IRIS) that occasionally results following the initiation of highly active antiretroviral therapy (HAART) may in rare instances induce a paradoxical clinical deterioration in patients suffering from PML.7 It has been documented that HAART-induced paradoxical aggravation of AIDS-related PML due to IRIS is reversible in most cases with the use of prolonged steroid therapy.7,8
Imaging can be particularly helpful when managing patients with PML and IRIS. PML lesions in patients not on HAART generally do not enhance, while in patients with IRIS contrast enhancement of the lesions may be seen.7
It therefore behoves us to be more vigilant when managing our patients with PML on HAART, as the early diagnosis and timely management of IRIS is critical.8
1. Del Valle L, Pina-Oviedo S. HIV disorders of the brain: pathology and pathogenesis. Front Biosd 2006; 11: 718-732. [ Links ]
2. Berger JR, Levy RM. AIDS and the Nervous System. 2nd ed. Philadelphia: Lippincott-Raven, 1997. [ Links ]
3. Berger JR, Houff S. Progressive multifocal leukoencephalopathy: lessons from AIDS and Natalizumab. Neurol Res 2006; 28: 299-305. [ Links ]
4. Shankar SK, Satishchandra P, Mahadevan A, et al. Low prevalence of progressive multifocal leukoencephalopathy in India and Africa: is there a biological explanation? J Neurovirol 2003; 9: suppl 1, 59-67. [ Links ]
5. Puren AJ. The HIV-1 epidemic in South Africa. Oral Dis 2002; 8: suppl 2, 27-31. [ Links ]
6. Modi G, Hari K, Modi M, Mochan A. The frequency and profile of neurology in black South African HIV infected (clade C) patients - a hospital-based prospective audit. J Neurol Sci 2007; 254(1-2): 60-64. [ Links ]
7. Gray F, Bazille C, Adle-Biassette H, Mikol J, Moulignier A, Scaravilli F.Central nervous system immune reconstitution disease in acquired immunodeficiency syndrome patients receiving highly active antiretroviral treatment. J Neurovirol 2005; 11: suppl 3, 16-22. [ Links ]
8. Nuttall JJ, Wilmshurst JM, Ndondo AP, et al. Progressive multifocal leukoencephalopathy after initiation of highly active antiretroviral therapy in a child with advanced human immunodeficiency virus infection: a case of immune reconstitution inflammatory syndrome. Pediatr Infect Dis J 2004; 23: 683-685. [ Links ]
 Correspondence:
Correspondence:
M Modi
(Mala.Modi@wits.ac.za)

