










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 no.4 Pretoria Abr. 2008
CORRESPONDENCE
BRIEWE
Is diabetic screening really feasible in South African urban primary care?
J C Rice; K S T Suttle; K A Lecuona
Department of Ophthalmology Groote Schuur Hospital and University of Cape Town James.Rice@uct.ac.za
To the Editor: We congratulate Mash and co-authors on their study on screening for diabetic retinopathy with a mobile fundus camera.1 A readily obtained digital image of the ocular fundus in most patients makes good sense when fundal examination is poorly performed in primary care facilities. Digital fundus photography is accepted as a screening method of choice. They are also to be congratulated on improving quality of care resulting from improving the average rate of retinal screening from 18 to 42%.
Screening for diabetic retinopathy and referral for laser treatment is a form of secondary prevention: treating a disease before it causes permanent loss of function. The high prevalence of diabetic retinopathy raises questions regarding the implementation of the primary prevention of diabetic retinopathy. Careful control of hyperglycaemia, hypertension and hyperlipidaemia delays the onset of diabetic retinopathy and improves established retinopathy.2,3 Retinal laser treatment can preserve vision but is a destructive procedure with many side-effects. The best treatment to prevent visual loss is systemic control of diabetes. If there is no progress in improving primary-level diabetic care, the number of patients referred for further treatment of eye disease will continue to increase.
Secondly, it would be unethical to identify patients requiring treatment if such treatment was not available or accessible. Note that a dedicated laser treatment service was established to manage the cases identified as needing treatment. This was necessary to avoid further referrals to the already overloaded tertiary level hospitals. This study helps to emphasise the severe shortage of infrastructure and human resources necessary to deal with patients with diabetic retinopathy.
Many patients were also identified requiring referral for cataracts and other conditions to secondary level ophthalmic services where capacity to manage them has yet to be developed. The limited secondary eye care services currently available therefore preclude the establishment of such a screening service as a mainstream programme.
Is diabetic screening really feasible in the South African urban primary care environment in the absence of sufficient higher levels of care?
1. Mash B, Powell D, du Plessis F, et al. Screening for diabetic retinopathy in primary care with a mobile fundal camera - evaluation of a South African pilot project. S Afr Med J 2007; 97: 1284-1288.
2. Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications of insulin-dependent diabetes mellitus. N Engl J Med 1993; 329: 977-979.
3. UK Prospective Diabetes Study Group. Intensive blood group with sulphonylurea or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837-853.
Professor B Mash replies: Dr Rice and colleagues question whether the need for secondary prevention of retinopathy can be reduced by better control of diabetes and whether improved quality of care within district health services will increase the demand for preventive treatment at referral centres.
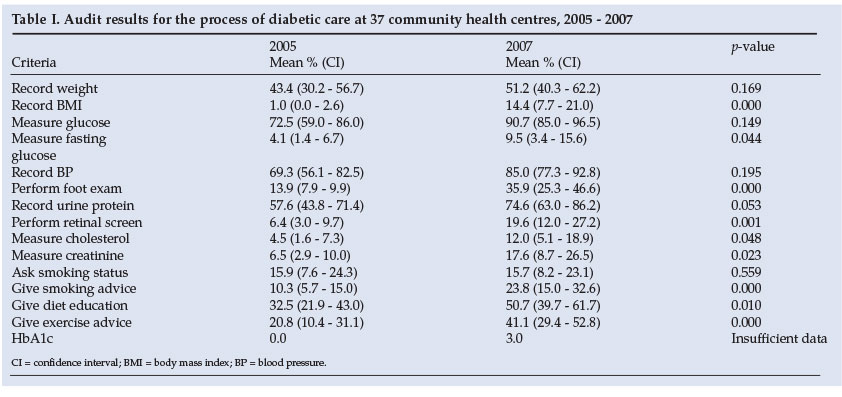
Health outcomes for diabetic patients partly relate to the quality of care offered in the district health services. Improved quality of care can therefore contribute to better outcomes, including lower rates and progression of retinopathy. Retinal screening was part of a broader initiative to improve the quality of care for diabetic patients in the Cape Town metropolitan area.1 Audits of community health centres show a significant improvement in many process indicators (Table I).
Annual assessment for retinopathy is recommended by diabetic guidelines including the 2006 International Diabetes Federation's Type 2 Diabetes Clinical Practice Guidelines for Sub-Saharan Africa. However, it would be unethical to identify patients requiring treatment if this was either unavailable or inaccessible. Cataract surgery is included as a surgical procedure for district hospitals in the national norms and standards, recognising that secondary level support might be required.2 At least one Cape Town district hospital offers high-volume cataract surgery on this basis. Laser treatment is not included and there is no clear policy in this regard. District health services do not see that they should offer laser treatment, which is done by tertiary services, but with limited capacity. It may be possible to train medical officers in laser therapy which does not have to be performed by an ophthalmologist. We are actively negotiating a way forward with all levels of care while the project's own medical officer, seconded from the district health services, continues to provide laser treatment.
Improvement in quality of care for chronic disorders at the district level may not reduce the quantity of referrals to higher levels, but can change the nature of the referrals from urgent treatment of end-stage complications to elective preventive interventions.
1. Mash B, Levitt N, Van Vuuren U, Martell R. Improving the diabetic annual review in primary care: An appreciative inquiry in the Cape Town District Health Services. SA Family Practice (in press). [ Links ]
2. A District Hospital Service Package for South Africa: A Set of Norms and Standards. Pretoria: Department of Health, 2002. [ Links ]


{kind=link}