










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 n.3 Pretoria Mar. 2008
ORIGINAL ARTICLES
Predictors of mortality in patients initiating antiretroviral therapy in Durban, South Africa
Bisola O OjikutuI; Hui ZhengII; Rochelle P WalenskyIII; Zhigang LuIV; Elena LosinaV; Janet GiddyVI; Kenneth A FreedbergVII
IMD, MPH. Harvard Center for AIDS Research (CFAR) and Division of AIDS, Harvard Medical School, Boston, MA, USA, and Division of Infectious Disease, Massachusetts General Hospital, Harvard Medical School
IIPhD. CFAR and Division of AIDS, Harvard Medical School
IIIMD, MPH. CFAR and Division of AIDS, Harvard Medical School, and Divisions of General Medicine and Infectious Disease, Massachusetts General Hospital
IVMD. CFAR and Division of AIDS, Harvard Medical School, and Divisions of General Medicine and Infectious Disease, Massachusetts General Hospital
VPhD. Department of Biostatistics, Boston University School of Public Health, Boston
VIMB ChB. McCord Hospital, Durban, South Africa
VIIMD, MSc. CFAR and Division of AIDS, Harvard Medical School, Divisions of General Medicine and Infectious Disease, Massachusetts General Hospital
ABSTRACT
OBJECTIVE: To identify predictors of mortality in patients initiating antiretroviral therapy (ART) in Durban, South Africa.
DESIGN: We conducted a retrospective cohort study analysing data on patients who presented to McCord Hospital, Durban, and started ART between 1 January 1999 and 29 February 2004. We performed univariate and multivariate analysis and constructed Kaplan-Meier curves to assess predictors.
RESULTS: Three hundred and nine patients were included. Forty-nine (16%) had died by the conclusion of the study. In univariate analysis, the strongest predictors of mortality were a CD4 cell count <50/µl (hazard ratio (HR) 3.70, 95% confidence interval (CI) 1.96 - 7.14), a haemoglobin concentration <8 g/dl (HR 1.23, 95% CI 1.08 - 1.40), a history of oral candidiasis (HR 3.17, 95% CI 1.70 - 5.87) and a history of cryptococcal meningitis (HR 2.76, 95% CI 1.80 - 19.2). A CD4 cell count <50/µl (HR 3.08, 95% CI 1.54 - 5.88) and a history of oral candidiasis (HR 2.58, 95% CI 1.37 - 4.88) remained significant in multivariate analysis. A history of tuberculosis was not a significant predictor of mortality.
CONCLUSIONS: Simple clinical and laboratory data independently predict mortality and allow for risk stratification in patients initiating ART in South Africa. Interventions enabling patients to be identified before they develop these clinical markers and earlier initiation of ART will help to ensure maximum benefits of therapy.
In accordance with the World Health Organization call for expanded access to antiretroviral therapy (ART), antiretroviral medications have become more widely available to HIV-infected patients in South Africa who qualify for them (WHO stage IV disease or CD4 count <200 cells/µl). New funding through the President's Emergency Plan for AIDS Relief (PEPFAR) and the South African government has led to a substantial increase in the number of patients who are able to access ART.1 As of April 2007, approximately 300 000 adults and children were receiving ART countrywide.2
The factors that have predicted mortality in studies evaluating patients prior to initiation of ART include a low CD4 cell count, high HIV RNA, mild to severe anaemia, low body mass index, elevated aspartate aminotransferase (AST), a history of opportunistic infections, and depression.3-6 Additional predictors of mortality include older age and advanced disease stage at presentation.7 Our objective was to identify predictors of mortality in patients initiating ART at the Sinikithemba clinic in Durban, South Africa.
McCord Hospital's Sinikithemba ('We Give Hope') Clinic has offered ART to patients at cost since 1999. In 2004 McCord Hospital was awarded PEPFAR funding. Since then, rapid scale-up has occurred and over 2 000 patients are receiving ART at that site. As more patients begin treatment, it is important to identify factors that predict a higher risk of mortality so that they can be more closely monitored.
Methods
We conducted a retrospective cohort study of all patients who started ART at the Sinikithemba Clinic from 1 January 1999 to 29 February 2004. Patients paid for all medications, except for antibiotics for tuberculosis and co-trimoxazole, and for laboratory studies, including CD4 count and HIV RNA. All patients initiating ART at Sinikithemba met WHO criteria for the use of antiretrovirals in resource-limited settings (WHO stage IV or CD4 cell count <200/µl). The ART regimens prescribed at Sinikithemba consisted of three-drug therapy using combinations listed by the WHO as approved first-line regimens. Most patients were prescribed non-nucleoside reverse transcriptase inhibitors (NNRTIs) in combination with two nucleoside reverse transcriptase inhibitors (NRTIs). The analysis also included patients who previously initiated ART at sites other than Sinikithemba. Patients with a history of receiving single-dose nevirapine to prevent mother-to-child transmission were included in the study.
Exclusion criteria were: (i) patients whose charts were missing or for whom substantial clinical data were missing from the file; or (ii) patients who presented to Sinikithemba on ART and did not have a pre-ART CD4 cell count and clinical history available.
Data collection
Data from paper medical records were reviewed using a standardised data collection instrument. Records were reviewed for variables at initial presentation, follow-up and death (if applicable). We collected data in the following domains: demographics, ART history, opportunistic infection history, clinical, and laboratory. For patients who died while taking ART, date of death and time from diagnosis to death were recorded.
A history of opportunistic infections was defined as a history reported by the patient to have occurred prior to presentation as well as any new diagnosis made prior to the initiation of ART. Because of limited diagnostic capability at the clinic, opportunistic infections were noted if there was documented clinical evidence or if they were treated empirically with a clinical response.
All chart reviews were conducted by a physician, a registered nurse with experience in providing HIV care, or a medical student. A random sample of 40 charts was re-reviewed by a second researcher to confirm inter-rater reliability. Inter-rater reliability ranged from 0.9 to 1.00. Data were double-entered, and any errors were corrected.
Statistical analysis
Univariate analysis for association with mortality was performed for each of the following variables: age, gender, WHO stage, CD4 cell count, weight, employment status, haemoglobin concentration and AST as well as history of tuberculosis, Pneumocystis jirovecii pneumonia, cryptococcal meningitis, Kaposi's sarcoma, oral candidiasis, toxoplasmosis and herpes zoster. The multivariate model consisted of six variables: age, gender, employment status, CD4 cell count, history of tuberculosis and history of oral candidiasis. CD4 cell count and history of tuberculosis were added on the basis of prior studies indicating their significance in predicting mortality. Employment status was added as an indicator of socioeconomic status. Oral candidiasis was included on the basis of statistically significant univariate analysis. Hazard ratios (HRs) were derived from univariate and multivariate Cox proportional hazards models. Kaplan-Meier curves were stratified by baseline CD4 cell count. One-year survival estimates by CD4 stratum were also determined. Tests of significance were two-sided with a probability cut-off value of 0.05.
Results
A total of 377 patients over the age of 18 years started ART at Sinikithemba during the study period. Three hundred and nine patients were included in the study. Reasons for exclusion were missing charts or charts where substantial clinical data was missing (49 patients) and a history of ART prior to enrolment at Sinikithemba with no pre-ART clinical data available (19 patients).
Mean age at initial presentation was 38 years (range 24 - 75 years). One hundred and seventy-four patients (56%) were female. Fifty-one patients (17%) had a prior history of ART use and had pre-ART clinical data available. Of these, 32 were on ART at the time of initial presentation. The median CD4 cell count was 65/µl (25th - 75th quartile = 26 - 138/µl) and the mean CD4 cell count 100/µl (standard deviation (SD) 106/µl). Fifty-two patients (17%) had an initial CD4 cell count <20/µl, 76 (26%) a count of 20 - 49/µl, 68 (23%) a count of 50 - 99/µl and 102 (34%) a count of ≥100/µl. The median initial HIV RNA was 5.2 log10 copies/ml (25th - 75th quartile = 4.6 - 5.6 log10 copies/ml) or 158 489 copies/ml, although these results were only available for 103 patients (33%). Sixty per cent of patients were in WHO stage IV at presentation (Table I). Forty-nine patients (16%) had died by the conclusion of the study.

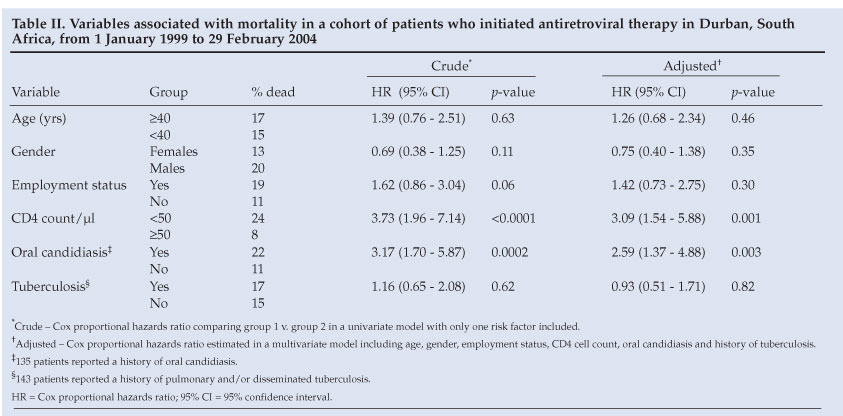
Univariate analysis revealed that a baseline CD4 cell count <50/µl was a significant predictor of mortality (HR 3.70, 95% CI 1.96 - 7.14, p<0.0001) (Table II). Patients who died had a mean pre-ART CD4 cell count of 50/µl compared with 109/µl for those who were alive at the conclusion of the study. A haemoglobin concentration <8 g/dl was also a significant predictor of mortality (HR 1.23, 95% CI 1.08 - 1.40, p=0.0015). Initial haemoglobin levels were available for 216 patients in the cohort (69%). This variable was therefore not included in the multivariate model.
In univariate analysis, a history of oral candidiasis and cryptococcal meningitis also conferred an increased mortality risk (HR 3.17, 95% CI 1.70 - 5.87, p=0.0002 and HR 2.76, 95% CI 1.07 - 7.10, p=0.03). Because there were only 12 cases of cryptococcal meningitis in the database this was also not included in the multivariate model. Patients with a history of tuberculosis (pulmonary or disseminated) were not at a significantly increased risk of death (HR 1.16, 95% CI 0.65 - 2.08, p=0.62) (Table II). A history of herpes zoster and P. jirovecii pneumonia was also not associated with increased mortality (HR 0.73, 95% CI 0.31 - 1.73, p=0.48 and HR 1.11, 95% CI 0.45 - 2.80, p=0.82). Only 2 cases of Kaposi's sarcoma were reported, and no cases of toxoplasmosis were documented.
In multivariate analysis, patients with a CD4 cell count <50/µl had a 3-fold higher risk of mortality (HR 3.08, 95% CI 1.54 - 5.88, p=0.001) and those with a history of oral candidiasis a 2.5-fold increased risk (HR 2.58, 95% CI 1.37 - 4.88, p=0.003) (Table II). Age, gender, employment status and history of pulmonary or disseminated tuberculosis were not predictive of mortality.
The mean duration of follow-up after ART initiation was 257 days. Patient follow-up time was censored due to patient drop-out or study conclusion. If a patient did not return to the clinic beyond that date and within 6 months of the conclusion of the study, they were designated lost to follow-up. In total, 23 patients (7.4%) were designated as such. No difference in age, gender, employment status, CD4 count, haemoglobin concentration, or presence of opportunistic infections was noted between patients who were lost to follow-up and those who were not. Kaplan-Meier curves comparing patients within four different initial CD4 cell count strata (<20/µl, 20 - 49/µl, 50 - 99/µl and ≥100/µl) are shown in Fig. 1. No significant difference was noted in survival between patients with an initial CD4 cell count of <20/µl compared with 20 -49/µl or in patients with an initial CD4 cell count of 50 - 99/µl compared with ≥100/µl. A significant trend was noted when the comparison was made across all CD4 strata (p<0.0001). Patients with a CD4 cell count ≥50/µl had significantly lower mortality than those with CD4 cell count <50/µl (p<0.0001). One-year mortality for patients with a CD4 cell count 20 -49/µl was high (0.40, 95% CI 0.24 - 0.55) but not significantly different from patients with a CD4 cell count <20/µl (0.32, 95% CI 0.16 - 0.42). The lowest 1-year mortality was noted for patients with a baseline CD4 cell count ≥100/µl (0.10, 95% CI 0.02 - 0.18).

Discussion
We sought to determine the factors prior to ART initiation that were most predictive of mortality in HIV-infected patients after they started ART in Durban, South Africa. Two factors were found to be the strongest predictors of mortality in these patients: a CD4 cell count <50/µl and a pre-ART history of oral candidiasis.
Mortality differences based on initial CD4 cell count have been documented in previous studies in sub-Saharan Africa.8 This study was consistent with those findings. Although the survival analysis indicates that there is little difference in mortality between patients who present with extremely low CD4 cell counts (<20/µl) and those who present with counts in a slightly higher range (20 - 50/µl), the significant difference in survival between patients in the <50/µl group and those in the ≥50/µl group indicates that immediate interventions may be better targeted toward patients with CD4 cell counts <50/ul.
Badri et al. in Cape Town noted that oral candidiasis was a significant predictor of mortality in patients who presented for care before ART was widely available.9 It is possible that oral candidiasis serves as a surrogate marker for the presence of undiagnosed opportunistic infection. Nittayananta et al. found a positive association between tuberculosis and the presence of oral candidiasis in a cohort of patients from Thailand.10 Oral candidiasis may also be a marker for more rapid disease progression, as is high HIV RNA. Campo et al. noted that high HIV RNA was significantly associated with oral candidiasis.11 Although viral load testing is not widely available in resource- constrained settings, the presence of oral candidiasis may assist clinicians in their assessment of the rapidity of disease progression if viral load data are not available.
Tuberculosis is currently the most common cause of AIDS-related mortality in developing nations.12 While we did not find that a pre-ART history of TB predicted mortality after starting ART, this study was not specifically powered to detect a mortality difference between patients with and without a history of TB. In addition, the lack of association in this study may be due to the timing of TB diagnosis. A history of pulmonary TB within the last 2 years is designated as a WHO stage III illness in HIV-infected patients.13 TB reported by the patient at the initial visit may have occurred more than 2 years prior to presentation. It is unclear whether or not a more distant history of TB infection will have a bearing on mortality.
This study has several limitations. CD4 cell counts and HIV RNA were not available for all patients because of cost. Past history of opportunistic infections may be limited by recall bias. Diagnostic tests that would confirm the presence of certain opportunistic infections were limited. Patients who started ART at outside clinics may not have met WHO criteria for initiation and may not have been prescribed widely accepted regimens. In addition, follow-up time was relatively short, and the retrospective study design limited our ability to gather data about factors that may increase the risk of mortality, such as lack of social supports and depression.
Over the course of the past year thousands of HIV-infected patients in South Africa who met the criteria of the WHO and the South African government have started ART. Since the conclusion of this study McCord Hospital's Sinikithemba Clinic has been awarded PEPFAR funding and many more patients have enrolled into the clinic's care and treatment programme. The data from this study will provide important baseline parameters against which to measure the expanded treatment taking place through the PEPFAR programme. As more patients present for care, it is critical for health care providers to be aware of those at highest risk of mortality in order to maximise clinical outcomes. This study demonstrates that simple laboratory and clinical data, available to health care providers prior to ART initiation, can predict which patients are at increased risk of death when they start therapy. Interventions enabling more patients to be identified before they develop these clinical markers and earlier initiation of ART will help ensure maximum benefits of therapy.
We would like to acknowledge Helga Holst, Superintendent; Jane Hampton, physician; Erica Dwyer, Fulbright Scholar; and Sophia
Ryberg, RN, all at McCord Hospital, for their assistance. We would also like to thank Sara Sadownik for technical assistance.
This study was supported in part by the National Institute of Allergy and Infectious Diseases (K23 AI01794, K24 AI01794, K25 AI50436, AI 058736 and P30 060354).
References
1. Keeping the promise to support treatment. Office of the US Global AIDS Coordinator, December 2005. www.state.gov/documents/organization/57612.pdf_ (last accessed 15 October 2006). [ Links ]
2. United States President's Emergency Plan for AIDS Relief: 2007 South Africa Country Profile. http://www.pepfar.gov/press/81640.htm (last accessed 15 July 2007). [ Links ]
3. Lieb S, Brooks RG, Hopkins RS, et al. Predicting death from HIV/AIDS: a case-control study from Florida public HIV/AIDS clinics. J Acquir Immune Defic Syndr 2002; 30: 351-358. [ Links ]
4. Egger M, May M, Chêne G, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet 2002; 360: 119-129. [ Links ]
5. Lundgren JD, Mocroft A. Anemia and survival in human immunodeficiency virus. Clin Infect Dis 2003; 37: Suppl 4, S297-303. [ Links ]
6. Farinpour R, Miller EN, Satz P, et al. Psychosocial risk factors of HIV morbidity and mortality: findings from the Multicenter AIDS Cohort Study (MACS). J Clin Exp Neuropsychol 2003; 25: 654-670. [ Links ]
7. Braitstein P, Brinkhof MW, Dabis F, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet 2006; 367: 817-824. [ Links ]
8. Frater AJ, Dunn DT, Beardall AJ, et al. Comparative response of African HIV-1 infected individuals to highly active antiretroviral therapy. AIDS 2002; 16: 1139-1146. [ Links ]
9. Badri M, Maartens G, Wood R. Predictors and prognostic value of oral hairy leukoplakia and oral candidiasis in South African HIV-infected patients. Journal of the South African Dental Association 2001; 56: 592-596. [ Links ]
10. Nittayananta W, Chanowanna N, Winn T, et al. Co-existence between oral lesions and opportunistic systemic diseases among HIV-infected subjects in Thailand. J Oral Pathol Med 2002; 31: 163-168. [ Links ]
11. Campo J, Del Romero J, Castilla J, et al. Oral candidiasis as a clinical marker related to viral load, CD4 lymphocyte count and CD4 lymphocyte percentage in HIV-infected patients. J Oral Pathol Med 2002; 3: 5-10. [ Links ]
12. Murray J, Sonnenberg P, Shearer SC, et al. Human immunodeficiency virus and the outcome of treatment for new and recurrent pulmonary tuberculosis in African patients. Am J Respir Crit Care Med 1999; 159: 733-740. [ Links ]
13. Interim WHO clinical staging of HIV/AIDS case definitions for surveillance. World Health Organization, February 2005. www.who.int/hiv/pub/guidelines/clinicalstaging.pdf (last accessed 6 March 2006). [ Links ]


{kind=link}