










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.98 n.2 Pretoria Feb. 2008
ORIGINAL ARTICLES
Incidence of nevirapine-associated hepatitis in an antenatal clinic
V BlackI; H ReesII
IMB BCh, BSc, DTMH, HIV Man Dip; Reproductive Health and HIV Research Unit, Department of Obstetrics and Gynaecology, University of the Witwatersrand, Johannesburg
IIOBE, MB BCh, MA, MRCGP, DCH, DRCOG; Reproductive Health and HIV Research Unit, Department of Obstetrics and Gynaecology, University of the Witwatersrand, Johannesburg
ABSTRACT
OBJECTIVE: To describe the incidence, clinical presentation and management of nevirapine-associated hepatitis among antiretroviral-naïve pregnant women treated with nevirapine-based antiretroviral therapy at a dedicated antenatal antiretroviral clinic.
METHODS: Retrospective analysis of pregnant women initiated on nevirapine-based highly active antiretroviral therapy at a dedicated antenatal antiretroviral clinic between July 2004 and December 2006.
RESULTS: Three hundred and ninety women were included in the analysis. Median age was 29 (interquartile range (IQR) 26 - 32) years and median pre-treatment CD4 cell counts was 157 (IQR 104 - 193) cells/µl. Baseline alanine transaminase (ALT) was elevated in 2.8% of women (11/390). After initiation of nevirapine-based ART 8% (31/390) experienced an ALT elevation. Three of these patients developed clinical hepatitis with jaundice (0.8%, 3/390). The mean and median time to clinical presentation was 5 weeks. Hepatitis resolved following discontinuation of ART. Non-nevirapine regimens were initiated following biochemical and symptomatic improvement; symptoms did not recur.
CONCLUSIONS: Among pregnant women, nevirapine-containing ART has a favourable safety profile, with a low incidence of serious hepatic events.
In April 2004 the South African Department of Health initiated comprehensive care for HIV-infected people that included the use of antiretroviral therapy (ART) in the public health sector. The first-line regimen consists of two nucleoside reverse transcriptase inhibitors, lamivudine and stavudine, together with a non-nucleoside reverse transcriptase inhibitor, either efavirenz or nevirapine.1 As efavirenz is thought to be a teratogen and is classified as a Food and Drug Administration (FDA) category D drug, nevirapine is the preferred agent for use in pregnant women, for women planning a pregnancy and for women at risk of becoming pregnant. Nevirapine is a highly effective antiretroviral (ARV) agent when used in combination with other appropriate ARVs.2 Nevirapine has two principal side-effects that are of particular concern to clinicians, which are Stevens-Johnson syndrome and hepatitis, both of which may be fatal.3,4
In response to the large number of pregnant women requiring ART, a specialised antenatal ARV clinic was established at Johannesburg Hospital in July 2004. We describe the incidence and clinical presentation of nevirapine-associated hepatitis among pregnant women treated with nevirapine at this clinic, and discuss management of this condition.
Methods
Pregnant women who were initiated on nevirapine-containing ART regimens between July 2004 and December 2006 were included in this analysis. Once initiated on ART these women were followed up weekly for the first 4 weeks and then 2 - 4-weekly until delivery. From October 2005 women were followed up to 10 weeks post partum. Alanine transaminase (ALT) levels were measured at baseline, at weeks 1 and 3 of ART treatment, and 2-weekly thereafter until 8 weeks of ART were completed. Demographic and clinical details for women attending the antenatal ARV clinic were entered into an Excel database. Variables collected included age, baseline clinical characteristics, pre-treatment and subsequent ALT levels and CD4 cell count.
Descriptive and summary statistics were performed, with continuous variables expressed as medians and interquartile ranges (IQRs).
Approval for the study was granted by the Human Research Ethics Committee of the University of the Witwatersrand.
Results
Three hundred and ninety women attending the antenatal ARV clinic received a nevirapine-based regimen and were eligible for analysis. The median age was 29 (IQR 26 - 32) years and the median pre-treatment CD4 cell counts were 157 (IQR 104 - 193) cells/µl. Baseline alanine aminotransferase (ALT) was elevated in 2.8% of women (11/390) after initiating ART. One of these women had a further transaminase increase that did not require a change in management.
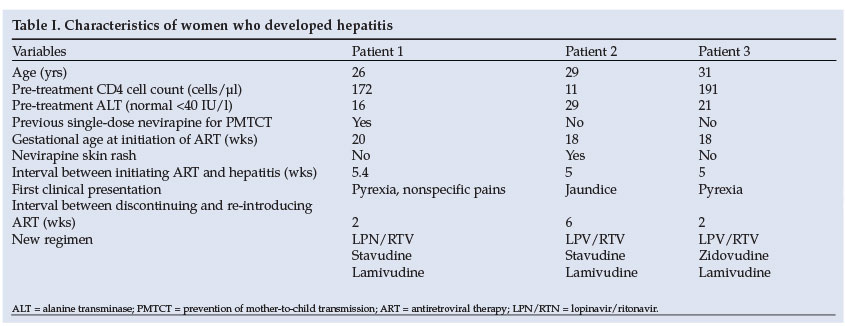
After initiation of nevirapine-based ART, 31 of 390 patients (8%) experienced an ALT elevation. Twenty-eight patients (7.2%) had grade 1 (1.25 - 2.5 x ULN),5 2 patients (0.5%) had grade 2 (2.6 - 5.0 x upper limit of normal (ULN))5 and 1 patient (0.3%) had grade 4 (> 10.0 x ULN)5 elevation in ALT. Of these, 2 patients with grade 1 ALT elevation and the patient with grade 4 elevation developed clinical hepatitis, with jaundice (0.8%, 3/390). Clinical characteristics of these 3 patients are presented in Table I. Serological markers for hepatitis A, B and C were negative and pre-treatment CD4 cell counts were below 200 cells/µl for all 3 patients. Pre-treatment and first monitoring of ALT 1 - 3 weeks after initiating nevirapine were all normal. Two of the 3 patients had insidious onset of nevirapine-associated hepatitis with fever and nonspecific abdominal pain before jaundice. All cases occurred between 5 and 6 weeks. In all 3 cases, hepatitis rapidly resolved following discontinuation of ART. Non-nevirapine regimens, substituting lopinavir/ritonavir for nevirapine, were initiated following biochemical and symptomatic improvement; symptoms did not recur. In 1 patient viral load was not suppressed on the new ART regimen, and after delivery she defaulted from follow-up.
Nineteen women (4.9%) in the cohort were changed from nevirapine to either efavirenz or lopinavir/ritonavir-based ART within 5 weeks of initiating nevirapine-based ART, 5 due to development of a nevirapine rash, 13 due to initiation of TB therapy, and 1 due to suspected auto-immune hepatitis.
Discussion
The Johannesburg Hospital antenatal ARV clinic has a low incidence of nevirapine hepatitis (0.8%). This may be due to a low threshold for nevirapine substitution in patients with a perceived risk of developing hepatitis, especially those on concurrent TB treatment, the low CD4 cell count of most women initiated on nevirapine therapy, the low number with an elevated pre-treatment ALT level and low reported alcohol and drug use among women attending the clinic. Other investigators6 have reported a low incidence of nevirapine toxicity in pregnant women.
Nevirapine-associated hepatotoxicity with elevation of transaminases to more than 5 times the upper limit of normal (ULN) occurred in 10% (range 1.1 - 17%) of HIV-infected nevirapine-treated patients in 17 clinical trials that included patients with high CD4 cell counts.7 In these trials, overall rates of serious hepatic events and death were low (0.06 - 0.13%).7 Clinical symptoms developed in 4.9% (3.2 - 8.9%) of patients.7 One of these studies from South Africa3 reported an incidence of nevirapine hepatitis of 17%, with 2 fatalities due to fulminant hepatitis despite discontinuation of ART. Clinical predictors of nevirapine-associated hepatitis included elevated transaminases >2.5 times the ULN before initiating ART, viral hepatitis B or C infection, and being female with a CD4 cell count greater than 250 cells/µl.8 Development of skin rash following initiation of nevirapine is associated with a >10-fold increased risk of hepatitis.7,9 Only 1 woman who developed hepatitis in this study had a known risk factor for hepatitis, transient rash 2 weeks after initiating nevirapine-based ART.
Nevirapine-associated hepatitis may have an insidious onset. Laboratory monitoring of ALT did not predict hepatitis in any of the 3 patients who developed hepatitis. A high index of suspicion is therefore needed in patients who present with nonspecific clinical symptoms shortly after starting nevirapine. Patients who develop rash following initiation of nevirapine-based ART should be monitored and made aware of symptoms of hepatitis. In cases of nevirapine rash where close monitoring is not possible, nevirapine substitution should be considered. Options include substitution with a protease inhibitor in situations such as co-infection with tuberculosis in the first trimester of pregnancy, a nucleoside reverse transcriptase inhibitor (triple nucleoside regimen), or changing from nevirapine to efavirenz. Efavirenz has been classified as a potential teratogen and should be avoided in early pregnancy.10 Where lopinavir/ritonavir has not been tolerated the authors have used efavirenz in pregnant women beyond the first trimester after risk counselling. No adverse outcomes were observed.
A limitation of this study is that follow-up over time varied, and any late incidence of hepatitis may be under-reported. However, this may have a minimal effect on the study, as hepatic events usually occur within 6 weeks of initiating nevirapine-based therapy.7
It is important to note that severe adverse events following single drug administration of nevirapine to pregnant women as part of prevention of mother-to-child transmission (PMTCT) of HIV has not been reported.11-13 Programmes built around this regimen remain important for preventing HIV infection to newborns where more effective regimens have not yet been implemented.14
Conclusion
Nevirapine-based triple therapy in South Africa's state sector is principally recommended for pregnant women or women at risk of pregnancy who do not have contraindications to nevirapine (background liver disease or a CD4 count >250 cells/µl). Findings of this study suggest that in this study population nevirapine-containing ART has a favourable safety profile, with a low incidence of serious hepatic events. Laboratory monitoring did not predict hepatitis in any of the 3 patients who developed hepatitis.
We would like to thank Andrew Black, Matthew Chersich, David Murdoch and Francois Venter for editing the manuscript; and Jonas Malete, Priya Menon and Adeyemi Adedayo for data retrieval. We thank the President's Emergency Plan for AIDS Relief (PEPFAR) and the Department of Health for their support for this study.
References
1. National Department of Health. National Antiretroviral Treatment Guidelines. 1st ed. Pretoria: Jacana, 2004. [ Links ]
2. van Leth F, Phanuphak P, Ruxrungtham K, et al. Comparison of first-line antiretroviral therapy with regimens including nevirapine, efavirenz, or both drugs, plus stavudine and lamivudine: a randomised open-label trial, the 2NN Study. Lancet 2004; 363:1253-1263. [ Links ]
3. Sanne I, Mommeja-Marin H, Hinkle J, et al. Severe hepatotoxicity associated with nevirapine use in HIV-infected subjects. J Infect Dis 2005; 191: 825-829. [ Links ]
4. Bohringer Ingelheim Roxane Laboratories. Physician Important Drug Warning Letter. November 2000. www.fda.gov/medwatch/safety/2000/virahp.pdf (last accessed August 2006). [ Links ]
5. DAIDS. Division of AIDS table for grading the Severity of adult and pediatric adverse events, December 2004. www3.niaid.nih.gov/research/resources/DAIDSClinRsrch/PDF/Safety/DAIDSAEGradingTable (last accessed December 2007). [ Links ]
6. Douglas D. Nevirapine toxicity uncommon in pregnant women. Am J Obstet Gynecol 2006; 194:199-202. [ Links ]
7. Dieterich DT, Robinson PA, Love J, Stern JO. Drug induced liver injury associated with the use of nonnucleoside reverse-transciptase inhibitors. Clin Infect Dis 2004; 38: Suppl 2, S80-89. [ Links ]
8. Hitti J, Frenkel LM, Stek AM, et al. Maternal toxicity with continuous nevirapine in pregnancy results from PACTG 1022. J Acquir Immune Defic Syndr 2004; 36: 772-776. [ Links ]
9. Moffenson LM. Antiretroviral treatmentduring pregnancy. In: UpToDate 2007: 15.3. www. uptodate.com (last accessed December 2007). [ Links ]
10. Nightingale S. From the FDA. JAMA 1998; 280: 1472. [ Links ]
11. Guay L, Musoke P, Fleming T, et al. Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-child transmission of HIV-1 in Kampala, Uganda: HIVNET 012 randomised trial. Lancet 1999; 354: 795-802. [ Links ]
12. Department of Health. Prevention of Mother-To-Child Transmission of HIV. South African Guidelines, 2002. www.doh.gov.za/docs/factsheets/guidelines/hivcirc041602 (last accessed December 2007). [ Links ]
13. Global stratergies for HIV Prevention. PMTCT-Nevirapine: Important facts on safety/ effectiveness. December 2004. http://www.niaid.nih.gov (last accessed December 2007). [ Links ]
14. World Health Organization. Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Guidelines on care, treatment and support for women living with HIV/AIDS and their children in resource-constrained settings, Geneva: WHO, 2004. www.who.int/hiv/pub/mtct/en/arvdrugswomenguidelinesfinal (last accessed December 2007). [ Links ]
 Correspondence:
Correspondence:
V Black
(v.black@rhru.co.za)
Accepted 26 February 2007.


{kind=link}