










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Education
On-line version ISSN 2076-3433
Print version ISSN 0256-0100
S. Afr. j. educ. vol.43 n.1 Pretoria Feb. 2023
http://dx.doi.org/10.15700/saje.v43n1a2136
ARTICLES
Symptoms of oppositional defiant disorder, conduct disorder and anger in children with ADHD
Ramatladi Meriam Mphahlele; Basil Joseph Pillay; Anneke Meyer
Department of Behavioural Medicine, School of Nursing and Public Health, University of KwaZulu-Natal, Durban, South Africa. merimphl@yahoo.com
ABSTRACT
With the research reported on here we sought to determine whether children with attention-deficit/hyperactivity disorder (ADHD) displayed more symptoms of oppositional defiant disorder (ODD), conduct disorder (CD) and anger, which are categorised as externalising disorders, when contrasted to the control group and, also, whether gender and age impacted these ADHD comorbidities. ADHD is a neurodevelopmental disorder that presents before the age of 12 years according to which an individual displays a recurrent pattern of extreme inattentiveness, overactivity, and impulsiveness that inhibits performance, and is not age-appropriate. ODD is defined as a psychological syndrome characterised by disruptive behaviour, a pattern of anger and irritability, confrontational, and spiteful behaviour. CD is a psychological and behavioural syndrome characterised by difficulties with following rules, recurrent patterns of hostility, destruction, and dishonesty. Anger is a frequent reaction (contrasted to ordinary irritable mood), intense and long-lasting defensive or retaliatory response to perceived provocation or threat, which interferes with normal functioning. Both teacher and parent ratings on the Disruptive Behavior Disorders Scale, and self-report on the Anger Inventory of the Beck Youth Inventories were employed in this investigation. The sample (n = 216) consisted of 216 school children aged 6 to 15 years that were divided into an ADHD group and a matched control group without ADHD (50 boys and 58 girls in each group). The results indicate that children with ADHD displayed notably elevated symptoms of ODD, CD and anger. The externalising disorders are more pronounced in boys with ADHD than in girls. Age had no effect on the results. We recommend that externalising comorbidities should be the target of early interventions. Our findings contribute to the debate about how best to conceptualise ADHD regarding related behavioural and emotional disturbances, and the treatment thereof. Since these symptoms occur during childhood and progress to adolescence, early identification and management may improve the livelihood of those affected.
Keywords: age; anger; attention-deficit/hyperactivity disorder; conduct disorder; gender; oppositional defiant disorder
Introduction and Background to the Study
Attention-deficit/hyperactivity disorder (ADHD) is a prevalent neurocognitive disorder with unknown etiology (Polanczyk, Willcutt, Salum, Kieling & Rohde, 2014) affecting 5% of children worldwide (Polanczyk et al., 2014), 7.47% in African countries (Ayano, Yohannes & Abraha, 2020), 5.5% of primary school children in the Limpopo province, South Africa, (Meyer, Eilertsen, Sundet, Tshifularo & Sagvolden, 2004) and 2.5% of adults worldwide (American Psychiatric Association [APA], 2013; Barkley, 2014). ADHD is more common in boys than in girls (2:1) and 1.6:1 in adults in the general population (APA, 2013). ADHD involves age-inappropriate levels of overactivity/impulsiveness (HI) and inattention that affect social and educational effectiveness or development (APA, 2013). There are three subtypes of ADHD: i) hyperactivity-impulsiveness (HI) characterised by a tendency to act without reflecting on the possible consequences of one's behaviour and difficulty awaiting one's turn, ii) inattention refers to difficulty sustaining attention on tasks at hand, and iii) the combined type characterised by the combination of HI and inattention (APA, 2013; De Milander, Schall, De Bruin & Smuts-Craft, 2020).
Although the etiology of ADHD is not distinctly understood, some studies (Johansen, Killeen, Russell, Tripp, Wickens, Tannock, Williams & Sagvolden, 2009; Sagvolden, Johansen, Aase & Russell, 2005) indicate that ADHD results from an interplay of multifactorial issues that include biological, psychological and social factors. Brain regions and neural pathways have been implicated in ADHD studies, suggesting that ADHD is a disorder of neurobiological origin. Current understanding of the pathophysiology of ADHD is limited, and little information is available on the cellular mechanisms that underlie the disorder (Johansen et al., 2009; Tripp & Wickens, 2008). The hereditarily-constructed functional variances in the corticostriatal-mesolimbic dopamine system are accountable for differences in impulsiveness; the prefrontal cortex is known to facilitate complex decision-making and planning, while the parietal cortex regulates attention (Sagvolden et al., 2005; Sonuga-Barke, Bitsakou & Thompson, 2010).
On the role of psychological and social factors in ADHD, postnatal smoke exposure is associated with higher rates of ADHD symptoms (Arnold, Elliott, Lindsay, Molina, Cornelius, Vitiello, Hechtman, Elliott, Newcorn, Epstein, Wigal, Swanson & Wells, 2005), as is a childhood history of physical and emotional maltreatment (González, Velez-Pastrana, McCrory, Kallis, Aguila, Canino & Bird, 2019). These findings suggest that genetic factors require an enabling environment to aggravate occurrence of symptoms (Azeredo, Moreira & Barbosa, 2018). ADHD often co-occurs with symptoms of oppositional defiant disorder (ODD) and conduct disorder (CD) (Bakare, 2012; Faraone, Asherson, Banaschewski, Biederman, Buitelaar, Ramos-Quiroga, Rohde, Sonuga-Barke, Tannock & Franke, 2015; Lavigne, LeBailly, Hopkins, Gouze & Binns, 2009; Pingali & Sunderajan, 2014), as well as anger (Humphreys, Aguirre & Lee, 2012; King & Waschbusch, 2010; Levy, Hay, Bennett & McStephen, 2005; White, Jarrett & Ollendick, 2013).
ODD involves a persistent pattern of defiance against authority lasting for at least 6 months, which typically appears in early childhood (APA, 2013) and is marked by argumentative or defiant behaviour, loss of temper, and intentional annoyance (Dick, Viken, Kaprio, Pulkkinen & Rose, 2005; Riley, Ahmed & Locke, 2016). Some studies (Bakare, 2012; Biederman, Monuteaux, Mick, Spencer, Wilens, Klein, Price & Faraone, 2006; Cuffe, Visser, Holbrook, Danielson, Geryk, Wolraich & McKeown, 2020; Levy et al., 2005; Pingali & Sunderajan, 2014; Rucklidge, 2010; Skogli, Teicher, Andersen, Hovik & 0ie, 2013) have shown that children with ADHD are inclined to show significantly more symptoms of ODD than a control group. When ADHD and ODD co-occur, symptoms are more severe and impairing (Deault, 2010; Liu, Hsiao, Chou & Yen, 2021).
For instance, Deault (2010) reviewed literature from 2000 to 2008 in order to scrutinise parenting variables associated with the development of externalising and internalising comorbidities, as well as deficiencies in academic as well as social activities in children with ADHD, to show that the co-occurrence of ADHD with ODD and CD worsens children's functional impairment. In relation to children with ADHD only, those with comorbid ADHD and ODD experience more social difficulties (Deault, 2010), behavioural problems, academic impairment (Liu et al., 2021), familial conflict (Deault, 2010) and substance abuse (Shoham, Sonuga-Barke, Yaniv & Pollak, 2021). The effects of this comorbidity are often lifelong and recurrently put such children at an elevated risk for developing further psychiatric conditions (Biederman et al., 2006).
Children with ADHD appear to have impairments in self-regulation and tend to act without considering potential outcomes of their behaviour (Hobson, Scott & Rubia, 2011; Noordermeer, Luman & Oosterlaan, 2016); this behaviour includes arguing with and defying adults' authority, losing their temper, and displaying angry or intentionally annoying behaviour (APA, 2013; Dick et al., 2005). Research reveals that children with ADHD and ODD often experience more social impairments and strained parent-child relationships (Van Lier, Van der Ende, Koot & Verhulst, 2007), and are more often rejected by peers than children with ADHD only (APA, 2013; Dick et al., 2005; Hoza, Mrug, Gerdes, Hinshaw, Bukowski, Gold, Kraemer, Pelham, Wigal & Arnold, 2005).
Social impairments often observed in children with ADHD and ODD may be due to their impulsive defiance and impaired self-regulation (Hobson et al., 2011; Noordermeer et al., 2016) suggesting that these comorbidities pose social challenges at school and home (Hoza et al., 2005), as these children often fail to cope with expectations/demands in these settings (APA, 2013).
The cause of ODD is not clearly understood at present. However, experts agree that an interaction of multiple factors stemming from biological and psycho-social issues may result in oppositional behaviour (Riley et al., 2016). The lifetime prevalence of ODD in the general population of children is 10.2%, with higher rates in boys than in girls, with gender prevalence rates of 11.2% and 9.2%, respectively (Nock, Kazdin, Hiripi & Kessler, 2007). People meeting the diagnostic criteria for ODD before 8 years of age often have poor treatment outcomes (Nock et al., 2007).
CD involves a recurrent and persistent pattern of behaviour such as stealing, cheating, fire-setting, truancy from school, lying, aggression, cruelty to animals and the destruction of property (APA, 2013; Dick et al., 2005). As indicated in some studies (Bakare, 2012; Cuffe et al., 2020; Pingali & Sunderajan, 2014), symptoms of CD are more prevalent among children with ADHD when compared to a control group. This comorbidity is possibly the effect of disinhibition in children with ADHD (Chmielewski, Bluschke, Bodmer, Wolff, Roessner & Beste, 2019; Van Hulst, De Zeeuw, Vlaskamp, Rijks, Zandbelt & Durston, 2018) and difficulty in learning socially acceptable behaviour (Noordermeer et al., 2016) resulting in children who present challenges with self-control, fault monitoring, and socially appropriate behaviour, and they often blame others for their own mistakes (Noordermeer et al., 2016).
Children with ADHD appear to display a low threshold for frustration tolerance, which in turn predisposes them to disruptive behaviour (Puiu, Wudarczyk, Goerlich, Votinov, Herpertz-Dahlmann, Turetsky & Konrad, 2018), hence, they find it difficult to control their urge to act in socially unacceptable ways. Children with ADHD show more rage and abrupt impulsive swings towards undesirable reactions when compared to controls (Banaschewski, Jennen-Steinmetz, Brandeis, Buitelaar, Kuntsi, Poustka, Sergeant, Sonuga-Barke, Frazier-Wood, Albrecht, Chen, Uebel, Schlotz, Van der Meere, Gill, Manor, Miranda, Mulas, Oades, Roeyers, Rothenberger, Steinhausen, Faraone & Asherson, 2012; Sobanski, Banaschewski, Asherson, Buitelaar, Chen, Franke, Holtmann, Krumm, Sergeant, Sonuga-Barke, Stringaris, Taylor, Anney, Ebstein, Gill, Miranda, Mulas, Oades, Roeyers, Rothenbergher, Steinhaussen & Faraone, 2010). Children with CD frequently experience challenges with social relationships and academic and occupational functioning (Sagar, Patra & Patil, 2019).
Children with ADHD often display motivational alterations shown by their preference for smaller immediate rewards as opposed to larger delayed ones in delay aversion activities (Luman, Oosterlaan & Sergeant, 2005; Marco, Miranda, Schlotz, Melia, Mulligan, Müller, Buttler, Christiansen, Gabriels, Medad, Albrecht, Uebel, Asherson, Banaschewski, Gill, Kuntsi, Mulas, Oades, Roeyers, Steinhausen, Rothenberger, Faraone & Sonuga-Barke, 2009; Paloyelis, Asherson & Kuntsi, 2009; Sonuga-Barke, 2002; Tripp & Alsop, 2001). ADHD is associated with increased frustration when executing long and uninteresting activities (Marco et al., 2009) when the administration of reinforcement is delayed (Luman et al., 2005; Plichta, Vasic, Wolf, Lesch, Brummer, Jacob, Fallgatter & Grön, 2009; Sonuga-Barke, 2002). Children with ADHD, irrespective of gender, are inclined to more CD problems than a control group. Children with ADHD and co-occurring CD seem to have significantly deficient decision-making, which is controlled in the amygdala and right striatum in the brain, which in turn predisposes children with ADHD to risky decision-making (Noordermeer et al., 2016). Sagar et al. (2019) note that in the United States, CD is twofold higher in boys (6% to 16%) than in girls (2% to 9%) with the onset of CD in boys at an earlier age compared to girls (i.e. 11 years vs. 15 years, respectively).
ODD and CD often co-occur (Eskander, 2020; Riley et al., 2016). ODD is believed to increase the risk for CD (Ghosh, A, Ray & Basu, 2017). Although ODD appears in 50% of individuals with ADHD, CD occurs in 20% of such cases (McBurnett & Pfiffner, 2009). The early onset of ADHD, ODD, and CD is linked by a common genetic influence (Dick et al., 2005; Tuvblad, Zheng, Raine & Baker, 2009), whereas adolescent onset of comorbid symptoms is linked to non-shared environmental factors such as maternal smoking during pregnancy, which increases vulnerability to ODD and CD (Derks, Dolan, Hudziak, Neale & Boomsma, 2007; Tuvblad et al., 2009).
Winstok (2009) describes anger as a defensive or retaliatory response to perceived provocation or threat which disrupts or impairs the sense of self or normal functioning. Anger reactions in people with anger issues are more frequent, intense and last longer compared to a typical response to provocation (DiGiuseppe & Tafrate, 2003). Children with ADHD often display increased symptoms of anger in relation to those without ADHD (Humphreys et al., 2012; King & Waschbusch, 2010; Singh, 2011; White et al., 2013) and often tend to become hostile and use aggressive solutions to social problems (Noordermeer et al., 2016; Rubia, 2011), which further predisposes them to more anger outbursts. Males with ADHD appear to be at an increased risk for anger compared to their female counterparts (Humphreys et al., 2012; King & Waschbusch, 2010; Levy et al., 2005; Singh, 2011; Tutian & Shechtman, 2015). The gender skew is possibly associated with a male tendency to become physically aggressive, whereas females more often display verbal aggression and cyberbullying (Ohan & Johnston, 2007). Liu et al. (2021) employed a Chinese clinical sample aged 11 to 18 years to show that frustration intolerance is associated with a higher risk of impulsivity, and hostility is linked to traditional (verbal and physical) victimisation, cyberbullying, and perpetration.
Studies suggest an absence of age disparities in the expression of anger symptoms among children with ADHD (Ghanizadeh & Haghighi, 2010), indicating that younger children, just like adolescents, have a genetic predisposition to overtly express anger (Azeredo et al., 2018; Harvey, Breaux & Lugo-Candelas, 2016).
Literature Review
ADHD commonly co-occurs with various psychiatric conditions such as depressive disorders, anxiety disorders, learning/intellectual disabilities, ODD and CD. However, in the context of this study, gender and age differences in three ADHD comorbidities were considered, namely: ODD (Bakare, 2012; Cuffe et al., 2020), CD (Pingali & Sunderajan, 2014) and anger (Tutian & Shechtman, 2015; White et al., 2013). However, the ODD/CD comorbidities appear more common, with higher rates in boys compared to girls (Bakare, 2012; Eskander, 2020; Rucklidge, 2010; Sagar et al., 2019; Skogli et al., 2013). In terms of age, most studies reveal a lack of differences in these comorbidities (Azeredo et al., 2018; Cuffe et al., 2020; Ghanizadeh & Haghighi, 2010; Tuvblad et al., 2009).
ADHD with ODD/CD comorbidity
Some studies show that children with ADHD display heightened symptoms of ODD (Bakare, 2012; Biederman et al., 2006; Cuffe et al., 2020; Pingali & Sunderajan, 2014) and CD (Cuffe et al., 2020; Sagar et al., 2019), often resulting in increased symptom severity and functional impairment when compared to a control group (Eskander, 2020). In a review article focusing on providing an outline of the psychosocial effect of ODD and CD comorbid with ADHD, Eskander (2020) reveals that the co-occurrence exacerbates severity of symptoms and is linked with poor psychosocial functioning, difficulties with friends and at school, and trouble with the police.
Gender differences in ODD/CD among children with ADHD
As noted by Eskander (2020), ODD strongly predicts CD in boys with ADHD. Boys with ADHD seem to present with more ODD symptoms than a control group (Nock et al., 2007). Furthermore, boys with ODD, with or without ADHD, show more symptoms of CD (Van Lier et al., 2007). While Bauermeister, Shrout, Chávez, Rubio-Stipec, Ramírez, Padilla, Anderson, García and Canino (2007) found no gender differences in comorbidity symptoms among children with ADHD, Levy et al. (2005) report more symptoms of ODD and CD in girls with ADHD compared to control groups. Also, ADHD and ODD in girls predisposes them to bullying and poor social skills, compared to females with only ADHD. The latter were again more aggressive than a control group without any of these conditions (Ohan & Johnston, 2007)
Age differences in ODD/CD among children with ADHD
Studies report no age differences in the severity of ODD symptoms in children with ADHD (Cuffe et al., 2020; Skogli et al., 2013). Although symptoms of ADHD, ODD, and CD improve with age (APA, 2013), studies show that ADHD seems to progress to ODD and further to CD, with an overlap of the symptoms of ODD and CD throughout the stages of progression (Ghosh, S & Sinha, 2012). This often results in deficient social skills and academic challenges (APA, 2013; Booster, DuPaul, Eiraldi & Power, 2012), and trouble with the legal system (Mordre, Groholt, Kjelsberg, Sandstad & Myhre, 2011). The existence of an ODD comorbidity in children with ADHD is a significant predictor of adolescent onset of CD (Eskander, 2020). Studies report an insignificant age difference in the expression of symptoms of ODD (Cuffe et al., 2020; Skogli et al., 2013) and CD (Tuvblad et al., 2009) in children with ADHD, however, there is a poorer prognosis in children with earlier onset of symptoms (Nock et al., 2007).
If age differences do occur, they could be linked to late development of the postcentral gyrus (Mizuno, Kagitani-Shimono, Jung, Makita, Takiguchi, Fujisawa, Tachibana, Nakanishi, Mohri, Taniike & Tomoda, 2019), and enlarged activity in the ventral striatum in reaction to incentives (Dir, Hummer, Aalsma & Hulvershorn, 2019). This suggests that children with ADHD require instant reward for their appropriate behaviour in order for them to continue behaving well (Marco et al., 2009). Social impairments may be due to defiance and disobedience that children with ODD display in social relationships with their parents and peers (APA, 2013).
ADHD with anger comorbidity
There is evidence that anger is associated with ADHD in both community and clinical samples. For instance, in a sample of 156 young German offenders aged 14 to 25 years, Barra, Turner, Müller, Hertz, Retz-Junginger, Tüscher, Huss and Retz (2022) found higher rates of self-reported ADHD and anger outbursts. Likewise Harty, Miller, Newcorn and Halperin (2009) used a clinical sample of 85 children aged 7 to 11 years, using cognitive measures, self-report and parent ratings of ADHD, to show that rates of anger are higher in children with ADHD and comorbid ODD/CD, relative to those with ADHD without comorbidity and a control group. Therefore, the comorbidity of ADHD and anger remains higher, irrespective of the sample type (clinical/community).
Gender differences in anger among children with ADHD
Regarding gender disparities in the expression of anger symptoms in children with ADHD, previous investigations report greater levels of comorbidity in boys, compared to girls, on self- and teacher reports (Humphreys et al., 2012; King & Waschbusch, 2010; Singh, 2011; Tutian & Shechtman, 2015).
Age differences in anger among children with ADHD
Some studies report mixed findings with regard to age variations in the expression of anger in children with ADHD. For instance, Ghanizadeh and Haghighi (2010) conducted a study with 197 clinic-and community-referred children and adolescents aged 8 to 14 years, using self-reports, and parent-teacher reports of school anger in children with and without ADHD. These researchers report a lack of age differences in anger expression; however, they further suggest that children with ADHD may express more anger and tend to display elevated anger outbursts as they grow older.
Theoretical Framework
The cause of ADHD is not clearly understood (Steinhausen, 2009). However, genetic factors (Azeredo et al., 2018), which give rise to dysfunctions in brain networks (hypo functioning dopaminergic system), which cause poor cognitive/mental and behavioural functioning (Dirlikov, Rosch, Crocetti, Denckla, Mahone & Mostofsky, 2015; Kofman, Gidley Larson & Mostofsky, 2008) have been implicated. The dynamic developmental theory (DDT) of Sagvolden et al. (2005) proposes that symptoms of ADHD stem from a diminished dopamine signal in the frontal lobe of the brain in expectancy of, or after, a reinforcer/reward. The impulsiveness detected in children with ADHD relative to a control group originates from the tendency of these children to prefer actions that give earlier smaller rewards over those that require waiting longer for bigger rewards (Marco et al., 2009; Paloyelis et al., 2009; Sonuga-Barke, 2002; Yu, Sonuga-Barke & Liu, 2018).
Symptoms of ODD and anger may occur independently of ADHD or co-occur with ADHD (Humphreys et al., 2012; Humphreys & Lee, 2011). However, CD rarely occurs without ADHD (Fairchild, Hawes, Frick, Copeland, Odgers, Franke, Freitag & De Brito, 2019).
Given that ADHD often co-occurs with ODD, CD and anger, some theories attempt to explain the ADHD-ODD-CD-anger link. Firstly, children with ADHD, when compared to the control group, often become frustrated and irritable in situations where it is expected of individuals to control their urge to act impulsively. In such situations, children with these comorbidities often display difficulties in waiting for a longer time which may yield larger rewards (Marco et al., 2009; Mphahlele, Pillay & Meyer, 2021; Paloyelis et al., 2009). Secondly, the early onset of ADHD, ODD, and CD is linked to a shared hereditary influence (Dick et al., 2005; Tuvblad et al., 2009), whereas the adolescent onset of symptoms has been associated with non-shared environmental factors such as maternal smoking during pregnancy (Derks et al., 2007; Tuvblad et al., 2009) and a childhood history of physical and emotional abuse (González et al., 2019). Thirdly, impulsive aggression in ADHD is associated with impaired prefrontal and cingulate activity, which suggests that ADHD and aggression are linked by common neuropsychological deficits (Kuntsi, Wood, Johnson, Andreou, Arias-Vasquez, Buitelaar, Rommelse, Sergeant, Sonuga-Barke, Uebel, Van der Meere, Banaschewski, Gill, Manor, Miranda, Mulas, Oades, Roeyers, Rothenberger, Steinhausen, Faraone & Asherson, 2010; Marco et al., 2009). Deficiencies in these areas often predispose a person to socially unacceptable behaviour and reactions, such as blaming others for their own hostility, and a tendency to implement impulsive and aggressive solutions to social problems (Noordermeer et al., 2016; Rubia, 2011). These findings suggest that genetic factors require an enabling environment in order to initiate the symptoms. Therefore, early identification and treatment of ADHD and its related comorbidities, such as ODD, CD and anger, is important, as the presence of these disorders may put children at risk for educational challenges.
Considered in combination, literature suggests substantial group, gender and age disparities in the expression of symptoms of ODD, CD and anger in children with and without ADHD, but conclusions may be limited due to methodological issues. In addition, the evidence base has been criticised for using either teacher or parent ratings on ADHD and externalising comorbidities. With this study we aimed to address these issues by using parent and teacher ratings and self-reports per construct by investigating the comorbidity of symptoms of ODD, CD and anger in 6 to 15-year-old non-referred children, with or without ADHD, and to establish whether there were gender or age differences in the expression of symptoms of ODD, CD and anger. More specifically, we aimed to answer the following questions: Will children with ADHD display more symptoms of ODD, CD and anger (externalising symptoms) compared to the control group? Are there gender differences in externalising symptoms in children with or without ADHD? Will younger children (6-10 years) express more externalising symptoms when compared to older ones (11-15 years).
Methodology
Research Design
This research was a component of a larger design in which neuropsychological and behavioural aspects of ADHD in various areas of the Limpopo province, South Africa, were investigated. A case-controlled, quantitative research approach was used to randomly select 216 children from 11 schools in the Lepelle-Nkumpi Municipality, in the Capricorn district of the Limpopo province.
Sample
Participants were Sepedi-speaking children aged 6 to 15 years. Based on school records, as well as information extracted from the medical history forms provided by the researchers and completed by parents and teachers, children with severe psychopathology, or auditory or visual impairments were excluded from participation in the study. Children aged 6 to 15 years who were not excluded as above were allowed participation in the study.
The final sample (n = 216) comprised 100 boys and 116 girls. Those who met the criteria for ADHD on the DBD were assigned to the ADHD group (n = 108). The control group (n = 108), matched for gender and age, was established from the cohort of children who did not meet the criteria for ADHD. Furthermore, the sample was divided into two age groups: 6 to 10 years (pre-pubertal): boys = 64; girls = 68 comprising 132 children with the mean age of 8.5 years, and 11 to 15 years (onset of puberty and pubertal): boys = 36; girls = 48, consisting of 84 children with the mean age of 13.2 years; this was to establish age differences in symptom manifestation for both the ADHD and control group.
Measuring Instruments
The Disruptive Behavior Disorder (DBD) Scale has 42 items; based on the Diagnostic and statistical manual of mental disorders (DSM-IV) (APA, 2000) criteria. It assesses the presence and severity of ADHD-related symptoms (viz. inattention, hyperactivity/impulsiveness, and combined types), ODD and CD. The questionnaire has four subscales: ADHD-inattention (9 items), ADHD-hyperactivity/impulsivity (9 items), ODD (8 items), and CD (16 items). Respondents were asked to rate the behaviour of the child on a 4-point Likert-type scale: not at all (0); just a little (1), pretty much (2); and very much (3). Children with scores above the 95th percentile were categorised as the ADHD group, and scores below the 85th percentile were considered for the control group to decrease the risk of false positives in the sample (Barkley, 1997; Barkley & Murphy, 2006). Children with scores > 26 on the hyperactivity/impulsivity and inattention subscales were regarded as the ADHD group. These cut-off points were based on the results of a previous study conducted in the Limpopo province by Meyer et al. (2004). Adequate psychometric properties for the DBD scale have been established (Barkley, 1997; Barkley & Murphy, 2006). Cronbach's α for this population was established at 0.92 for the inattention and 0.90 for the hyperactivity/impulsivity subscales.
One part of the Beck Youth Inventories™ (BYI-II) (Beck, JS, Beck, Jolly & Steer, 2005) was individually administered to the participants. The BYI-II consists of five self-report inventories of which one (anger) measures the presence and severity of anger (Beck, AT, Emery & Greenberg, 2005). The scale contains 20 questions about anger issues experienced by young people. Each of the 20 items is rated on a 4-point Likert-type scale: never (0); sometimes (1), often (2); and always (3), based on the severity of reactions over the past 2 weeks. The total score ranged from 0 to 60. The higher the score, the more severe the symptoms.
Procedure
Both teachers and parents were educated on ADHD symptoms and how to individually rate the children's behaviour on the DBD Scale. After establishing that they understood, the teachers screened children for the presence and severity of ADHD, ODD, and CD symptoms. Parents and/or caregivers submitted completed demographic/ medical history questionnaires and their written consent for each child. The DBD scales were distributed to the parents or caregivers who were requested to rate the children's behaviour as it occurred at home, by completing the DBD questionnaire. Parents could complete either the English or Sepedi version of the DBD scale to confirm the presence and severity of the symptoms at home (Pelham, Gnagy, Greenslade & Milich, 1992; Pillow, Pelham, Hoza, Molina & Stultz, 1998). The Sepedi version was translated and standardised on a sample of over 6,000 Sepedi-speaking primary school children in the Limpopo province of South Africa (Meyer et al., 2004).
The BYI-II anger inventory was administered by the clinical psychologist (researcher), assisted by fieldworkers who held psychology qualifications (Bachelor of Psychology [B Psych] or Bachelor of Arts Honours in Psychology [BA Hons Psych]). The fieldworkers were conversant in Sepedi and trained in the administration of the questionnaire and were monitored and supervised by the researcher. Test instructions were explained to the participants. Each participant indicated the level of their anger reactions in the past 2 weeks on a 4-point Likert scale. Assessment was conducted in a quiet, well-ventilated room during school hours. The assessment lasted about 10 to 15 minutes per child.
Data Analysis
Statistica 10 (StatSoft, Inc., 2011) was used for statistical analysis. MANOVA was used to investigate possible between-group differences. A 2 x 2 x 2 (ADHD group x gender x age) multifactorial ANOVA was employed. Post-hoc analysis (Bonferroni) was conducted in order to determine within-group differences.
Ethical Considerations
Ethical clearance was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal, Durban, South Africa (reference number HSS/1446/015D) and the Department of Education, Limpopo province, South Africa. School principals gave verbal consent for the study to be conducted in their schools. Parents gave written consent for their children to participate in the study. I read the assent form to the children out load in their home language and received assent, after establishing that they understood the content. Autonomy was ensured throughout the investigations by allowing participants to withdraw from the study at any stage without penalty.
Results
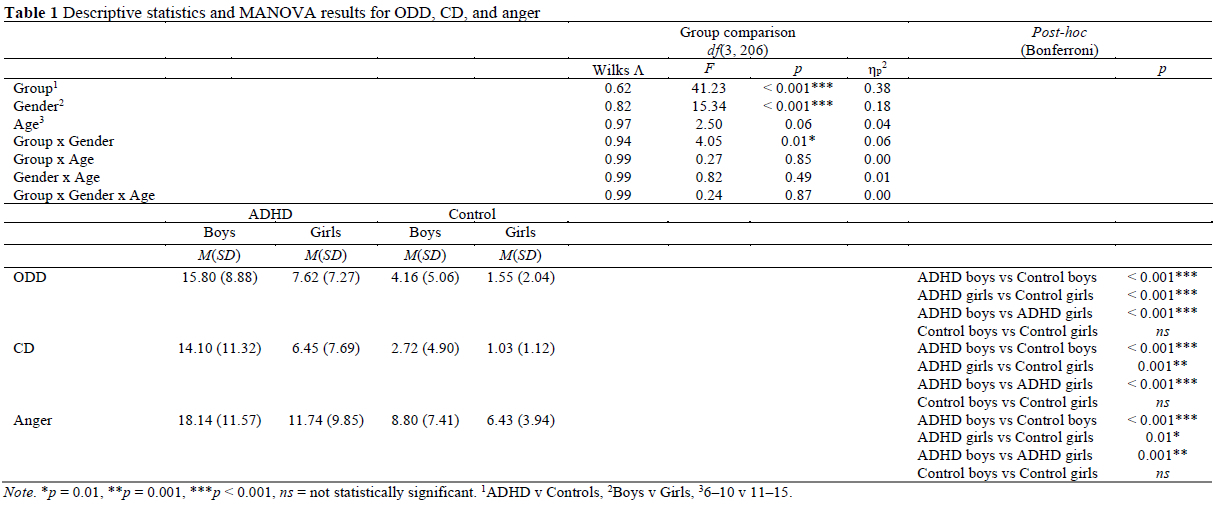
Descriptive statistics, the results of the MANOVA and the post-hoc results for externalising comorbidities (ODD, CD and anger) are displayed in Table 1.
The MANOVA showed a main effect for group (ADHD versus control): Wilks Λ = 0.62, F(3, 206) = 41.23, p < 0.001, ηp2 = 0.38.
There was also a main effect for gender: Wilks Λ = 0.82, F(3, 206) = 15.34, p < 0.001, ηρ2 = 0.18. Group and gender interacted: Wilks Λ = 0.94, F(3, 206) = 4.05, p = 0.01, ηp2 = 0.06. There was no effect for age, neither main nor interacting (Table 1).
Effect sizes (partial eta squared, ηp2) of 0.38 (between ADHD and control) and 0.18 (between genders) can be considered as large (Richardson, 2011).
Post-hoc (Bonferroni) analysis revealed the following:
ODD: ADHD boys scored significantly higher on the ODD scale than control boys (p < 0.001). ADHD girls also scored significantly higher on ODD symptoms than the control girls (p < 0.001). Boys with ADHD obtained higher ODD scores than girls (p < 0.001). However, control boys and girls did not differ significantly. Age did not affect the expression of ODD symptoms in either of the two age categories.
CD: ADHD boys scored significantly higher on the CD scale than the control boys (p < 0.001), as did ADHD girls versus the control (p = 0.001). ADHD boys scored significantly higher on the CD scale than the girls (p < 0.001). CD scale results revealed non-significant gender differences within the controls. A non-significant age effect was observed in the expression of symptoms of CD.
Anger: ADHD boys scored significantly higher on the BYI-II anger inventory than the control boys (p < 0.001), as did the ADHD girls (p = 0.01). When the scores of the ADHD boys were compared with the ADHD girls, the boys scored significantly higher on the BYI-II anger inventory than the girls (p = 0.001). A comparison of anger symptoms between the control boys and girls did not reveal significant differences. Age did not affect the results.
Discussion
In this study we examined gender and age differences in symptoms of ODD, CD and anger in children with ADHD and a matched control group without ADHD using the teacher and parent DBD rating scale for ADHD, ODD, and CD, and the BYI-II self-reported anger inventory. Consistent with our hypotheses and some prior studies (Levy et al., 2005; Ohan & Johnston, 2007; Rucklidge, 2010; Skogli et al., 2013), the results suggest that ADHD is associated with ODD, CD and anger, with increased rates of comorbidity in boys with ADHD compared to girls. There were no gender differences in the expression of symptoms in the control group. The overall results showed no age differences in symptom severity.
ODD Comorbid with ADHD
Consistent with other studies (Bakare, 2012; Biederman et al., 2006; Cuffe et al., 2020; Nock et al., 2007; Pingali & Sunderajan, 2014), we found that children with ADHD displayed more symptoms of ODD than the control group. This could possibly be explained in that children with ADHD may have impaired self-regulation and act without considering the possible outcomes of their behaviour (Hobson et al., 2011; Noordermeer et al., 2016).
Children of both genders with ADHD displayed significantly more ODD symptoms than the control group, which confirms that ODD symptoms are associated with ADHD symptomatology (Cuffe et al., 2020; Skogli et al., 2013); this was also reported by similar studies (Levy et al., 2005; Rucklidge, 2010). In a community sample of 17,230 children from kindergarten to Grade 5 using teacher and parent ratings, Cuffe et al. (2020) show that children with ADHD were at an increased risk of also having a significantly higher rate of ODD compared to the control groups. Similar findings were reported by Skogli et al. (2013) who used parent ratings on the Child Behavior Checklist (CBCL) in a clinical sample of 130 participants aged 8 to 17 years.
Boys are more likely to present with the HI component of ADHD than girls who, in turn, display more inattention symptoms (APA, 2013; Lavigne et al., 2009). In our study, the boys with ADHD showed significantly higher scores than the girls with ADHD on the ODD scale, possibly due to the fact that boys with ADHD, as well as those with externalising comorbidities, remain more likely to be identified, often resulting in higher than expected rates of referral and treatment in boys (Barkley, 2014). Also, the strong public perception that ADHD is a behavioural disorder that primarily affects boys tends to lead to referral bias (Skogli et al., 2013). In this study we did not find significant gender differences among the controls, since both genders showed fewer symptoms.
Consistent with Lavigne et al. (2009), who found that pre-schoolers with ADHD and comorbid ODD were at an increased risk of symptom progression into adolescence and adulthood, we did not find age differences in ODD prevalence among children with ADHD. Our results suggest that ODD symptoms in children with ADHD were already present by the age of 6, which was the age of the youngest participant in this sample.
There is evidence that children with ADHD and ODD/CD are more socially impaired, and more often rejected by their peers than children with ODD/CD but without ADHD (Cuffe et al., 2020). Impulsive defiance (APA, 2013; Dick et al., 2005) and impaired self-regulation (Hobson et al., 2011; Noordermeer et al., 2016) may be causative factors to the ADHD/ODD link. These comorbidities also pose academic challenges (Hoza et al., 2005) as children with ADHD often fail to cope with the expectations and demands in the school setting (APA, 2013).
CD Comorbid with ADHD
The findings that symptoms of CD were more prevalent in children with ADHD when compared to the control group echoes previous studies (Bakare, 2012; Pingali & Sunderajan, 2014). As noted by Bakare (2012) in a meta-analysis of nine studies, CD is one of the common comorbid conditions of ADHD. This comorbidity is possibly due to inhibitory deficits in children with ADHD (Chmielewski et al., 2019; Van Hulst et al., 2018) and the difficulty experienced by children with ADHD in learning socially acceptable behaviour (Noordermeer et al., 2016). In these situations, children show deficiencies in displaying acceptable behaviour and reactions, end up blaming others for their actions, display hostility, and implement aggressive resolutions to social problems (Noordermeer et al., 2016). Furthermore, children with ADHD comorbid with CD have a low threshold for frustration tolerance, which in turn predisposes them for disruptive behaviour (Puiu et al., 2018) meaning that they fail to control the urge to act in a socially unacceptable manner.
Another finding from this study is that the rates of CD were higher in boys with ADHD than in girls with ADHD, which supports other studies (Bakare, 2012; Biederman et al., 2006; Cuffe et al., 2020; Pingali & Sunderajan, 2014; Tuvblad et al., 2009). This suggests that the more prevalent hyperactivity/impulsiveness features of ADHD found in boys predispose them to increased rates of CD (APA, 2013). However, Pingali and Sunderajan (2014) used parent ratings on a behaviour checklist on an outpatient sample of 174 ADHD children (6 to 15 years) attending a psychiatry clinic, and found no gender differences in symptoms of CD. Tuvblad et al. (2009) used parent ratings in a population-based twin study of 1,241 twins aged 9 to 10 years aimed at investigating the genetic and environmental correlation. Tuvblad et al. (2009) found gender differences in the genetic influences, although there was a somewhat lower correlation for CD symptoms in male-female twin pairs, with genetic influences being slightly larger in girls and the shared environment somewhat larger in boys. This suggests some possibility of different genetic influences being important in boys and girls. As our study was conducted on a community sample only, it is possible that we missed more disturbed cases that were taken directly to clinical settings catering for such cases. Further, our results indicate an absence of gender differences in comorbidity among the controls, possibly due to the absence of ADHD symptomatology.
In line with Tuvblad et al. (2009), we found no age differences in the expression of symptoms of CD among children with ADHD. However, contrary to our finding, Van Lier et al. (2007) studied 2,076 participants aged 4 to 18 years, using parent ratings on the CBCL, and showed an adolescent peak in rates of CD among males with ADHD.
Anger Comorbid with ADHD
Consistent with Humphreys et al. (2012), King and Waschbusch (2010), Singh (2011) and White et al. (2013), our results show that children with ADHD display more symptoms of anger than a neurotypical control group. Studies show that emotional lability (Banaschewski et al., 2012), difficulty with waiting (APA, 2013; Tuvblad et al., 2009) for reward (Luman et al., 2005; Marco et al., 2009; Paloyelis et al., 2009; Sonuga-Barke, 2002; Tripp & Alsop, 2001), and subsequent preference for aggressive reactions to social situations (Noordermeer et al., 2016; Rubia, 2011) predispose children with ADHD to more anger outbursts. However, Ghanizadeh and Haghighi (2010) studied 158 children aged 8 to 14 years using self-reported anger within the school context, and reported that children with ADHD did not display more symptoms of anger when compared to the control group. The discrepancy between our findings and those of Ghanizadeh and Haghighi (2010) may be due to differences in methodologies used.
The increased rates of anger in boys with ADHD, when compared to girls with ADHD supports previous studies (Humphreys et al., 2012; King & Waschbusch, 2010; Singh, 2011; Tutian & Shechtman, 2015) which used self- and teacher reports to demonstrate that rates of aggression are heightened in boys with ADHD when compared to matched girls. The gender skew is possibly the result of fewer HI symptoms in girls with ADHD, who tend to show more symptoms of inattention (APA, 2013) and who often display their anger in a socially acceptable manner considered to be consistent with gender (femininity) norms. Both of these affect the probability of girls freely and openly expressing their anger (Rosqvist & Arnell, 2018). Again, we did not find significant gender differences in symptoms of anger in the control group; both genders appeared not to be deficient in self-regulation (as are children with ADHD) (Noordermeer et al., 2016) since they are able to behave in a socially acceptable manner.
The results do not indicate that age affects the feeling and expression of anger among children with ADHD. This finding is divergent from Ghanizadeh and Haghighi (2010), who argue that, although children with ADHD do not show age differences in the expression of anger, this does not rule out the probability that these children may experience more anger and engage in more destructive aggressive expressions as they grow older. In this study, a possible reason for the lack of age differences is that the mean age of the sample was 10 years, with the majority being pre-adolescents, when rates of impulsiveness are known to be more pronounced (Azeredo et al., 2018; Harvey et al., 2016), and brain changes due to hormonal action (Dir et al., 2019) are not yet established.
The results indicate that ADHD is associated with disruptive behaviour symptomatic of ODD, CD and anger, and untreated individuals may be at risk during adolescence and adulthood for substance use (Shoham et al., 2021), risky driving (Pollak, Dekkers, Shoham & Huizenga, 2019) and delinquent behaviour (Mordre et al., 2011; Young, Adamo, Ásgeirsdóttir, Branney, Beckett, Colley, Cubbin, Deeley, Farrag, Gudjonsson, Hill, Hollingdale, Kilic, Lloyd, Mason, Paliokosta, Perecheria, Sedgwick, Skirrow, Tierney, Van Rensburg & Woodhouse, 2020), which negatively impact on academic, occupational and social functioning. Therefore, these comorbidities necessitate early identification and referral for appropriate intervention. These children usually benefit from medical treatment (Jensen, Hinshaw, Kraemer, Lenora, Newcorn, Abikoff, March, Arnold, Cantwell, Conners, Elloitt, Greenhill, Hechtman, Hoza, Pelham, Severe, Swanson, Wells, Wigal & Vitiello, 2001) as well as behavioural interventions (Tutian & Shechtman, 2015) in which teachers, parents and healthcare providers work in collaboration to ensure that children are rewarded for appropriate behaviour to promote recurrence of such behaviour.
It can be concluded that children with ADHD have increased rates of ODD, CD, and anger when compared to a control group and they tend to display more inappropriate behavioural and aggressive responses in social relationships; this might be due to their impulsiveness that further predisposes to a rush for reward (Rubia, 2011). Boys with ADHD showed significantly more symptoms than girls with ADHD. No gender differences in ODD, CD, and anger were found among the control group, who were without ADHD symptoms. No age differences could be established in either the ADHD or control group in the expression of comorbidity symptoms.
Limitations
A community-based sample was used, therefore, findings should be interpreted with caution when generalising to clinical settings. Our sample was relatively homogenous in terms of language and geographical location. In addition, we did not include the adolescent category where the rates of externalising comorbidities are known to peak, and this may have limited the investigation of age differences. Future studies should include late adolescents to investigate the neuro-developmental factors underlying the gender and age differences in the expression of symptoms of ODD, CD and anger among children with and without ADHD.
Acknowledgements
We acknowledge the Limpopo Department of Education for their approval of the study. We are grateful to the principals, teachers, parents, and the learners who took part in our investigation, and to the fieldworkers who assisted with the data collection as well as the College of Health Sciences Research Office of the University of KwaZulu-Natal for funding the study.
Authors' Contributions
RMM conducted data collection, concept and design, drafting of the article and finalising the version to be published; BJP was the supervisor for the Doctor of Philosophy (PhD) study of which this manuscript forms part, and was responsible for editing and final approval of the version to be published; AM was co-supervisor for the PhD study and conducted the data analysis, constructed the tables and revised the article.
Notes
i. Published under a Creative Commons Attribution Licence.
References
American Psychiatric Association 2000. Diagnostic and statistical manual of mental disorders: DSM-IV-TR (4th ed). Washington, DC: Author. [ Links ]
American Psychiatric Association 2013. Diagnostic and statistical manual of mental disorders: DSM-5™(5th ed). Arlington, VA: Author. https://doi.org/10.1176/appi.books.9780890425596 [ Links ]
Arnold LE, Elliott M, Lindsay RL, Molina B, Cornelius MD, Vitiello B, Hechtman L, Elliott GR, Newcorn J, Epstein JN, Wigal T, Swanson JM & Wells K 2005. Gestational and postnatal tobacco smoke exposure as predictor of ADHD, comorbid ODD/CD, and treatment response in the MTA. Clinical Neuroscience Research, 5(5-6):295-306. https://doi.org/10.1016/j.cnr.2005.09.009 [ Links ]
Ayano G, Yohannes K & Abraha M 2020. Epidemiology of attention-deficit/hyperactivity disorder (ADHD) in children and adolescents in Africa: A systematic review and meta-analysis. Annals of General Psychiatry, 19:21. https://doi.org/10.1186/s12991-020-00271-w [ Links ]
Azeredo A, Moreira D & Barbosa F 2018. ADHD, CD, and ODD: Systematic review of genetic and environmental risk factors. Research in Developmental Disabilities, 82:10-19. https://doi.org/10.1016/j.ridd.2017.12.010 [ Links ]
Bakare MO 2012. Attention deficit hyperactivity symptoms and disorder (ADHD) among African children: A review of epidemiology and comorbidities. African Journal of Psychiatry, 15(5):358-361. https://doi.org/10.4314/ajpsy.v15i5.45 [ Links ]
Banaschewski T, Jennen-Steinmetz C, Brandeis D, Buitelaar JK, Kuntsi J, Poustka L, Sergeant JA, Sonuga-Barke EJ, Frazier-Wood AC, Albrecht B, Chen W, Uebel H, Schlotz W, Van der Meere JJ, Gill M, Manor I, Miranda A, Mulas F, Oades RD, Roeyers H, Rothenberger A, Steinhausen HC, Faraone SV & Asherson P 2012. Neuropsychological correlates of emotional lability in children with ADHD [Special issue]. The Journal of Child Psychology and Psychiatry, 53(11):1139-1148. https://doi.org/10.1111/j.1469-7610.2012.02596.x [ Links ]
Barkley RA 1997. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin, 121(1):65-94. [ Links ]
Barkley RA 2014. Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York, NY: Guilford Publications. [ Links ]
Barkley RA & Murphy KR 2006. Attention-deficit hyperactivity disorder: A clinical workbook (3rd ed). New York, NY: Guilford Press. [ Links ]
Barra S, Turner D, Müller M, Hertz PG, Retz-Junginger P, Tüscher O, Huss M & Retz W 2022. ADHD symptom profiles, intermittent explosive disorder, adverse childhood experiences, and internalizing/externalizing problems in young offenders. European Archives of Psychiatry and Clinical Neuroscience, 272:257-269. https://doi.org/10.1007/s00406-020-01181-4 [ Links ]
Bauermeister JJ, Shrout PE, Chávez L, Rubio-Stipec M, Ramírez R, Padilla L, Anderson A, García P & Canino G 2007. ADHD and gender: Are risks and sequela of ADHD the same for boys and girls? The Journal of Child Psychology and Psychiatry, 48(8):831-839. https://doi.org/10.1111/j.1469-7610.2007.01750.x [ Links ]
Beck AT, Emery G & Greenberg RL 2005. Anxiety disorders and phobias: A cognitive perspective. New York, NY: Basic Books. [ Links ]
Beck JS, Beck AT, Jolly JB & Steer RA 2005. Manual for the Beck youth inventories of emotional and social impairment (2nd ed). San Antonio, TX: Psychological Corporation. [ Links ]
Biederman J, Monuteaux MC, Mick E, Spencer T, Wilens TE, Klein KL, Price JE & Faraone SV 2006. Psychopathology in females with attention-deficit/hyperactivity disorder: A controlled, five-year prospective study. Biological Psychiatry, 60(10):1098-1105. https://doi.org/10.1016/j.biopsych.2006.02.031 [ Links ]
Booster GD, DuPaul GJ, Eiraldi R & Power TJ 2012. Functional impairments in children with ADHD: Unique effects of age and comorbid status. Journal of Attention Disorders, 16(3):179-189. https://doi.org/10.1177/1087054710383239 [ Links ]
Chmielewski W, Bluschke A, Bodmer B, Wolff N, Roessner V & Beste C 2019. Evidence for an altered architecture and a hierarchical modulation of inhibitory control processes in ADHD. Developmental Cognitive Neuroscience, 36:100623. https://doi.org/10.1016/j.dcn.2019.100623 [ Links ]
Cuffe SP, Visser SN, Holbrook JR, Danielson ML, Geryk LL, Wolraich ML & McKeown RE 2020. ADHD and psychiatric comorbidity: Functional outcomes in a school-based sample of children. Journal of Attention Disorders, 24(9): 1345-1354. https://doi.org/10.1177/1087054715613437 [ Links ]
Deault LC 2010. A systematic review of parenting in relation to the development of comorbidities and functional impairments in children with Attention-Deficit/Hyperactivity Disorder (ADHD). Child Psychiatry & Human Development, 41(2):168-192. https://doi.org/10.1007/s10578-009-0159-4 [ Links ]
De Milander M, Schall R, De Bruin E & Smuts-Craft M 2020. Prevalence of ADHD symptoms and their association with learning-related skills in Grade 1 children in South Africa. South African Journal of Education, 40(3):Art. #1732, 7 pages. https://doi.org/10.15700/saje.v40n3a1732 [ Links ]
Derks EM, Dolan CV, Hudziak JJ, Neale MC & Boomsma DI 2007. Assessment and etiology of attention deficit hyperactivity disorder and oppositional defiant disorder in boys and girls. Behavior Genetics, 37(4):559-566. https://doi.org/10.1007/s10519-007-9153-4 [ Links ]
Dick DM, Viken RJ, Kaprio J, Pulkkinen L & Rose RJ 2005. Understanding the covariation among childhood externalizing symptoms: Genetic and environmental influences on conduct disorder, attention deficit hyperactivity disorder, and oppositional defiant disorder symptoms. Journal of Abnormal Child Psychology, 33(2):219-229. https://doi.org/10.1007/s10802-005-1829-8 [ Links ]
DiGiuseppe R & Tafrate RC 2003. Anger treatment for adults: A meta-analytic review. Clinical Psychology: Science and Practice, 10(1):70-84. https://doi.org/10.1093/clipsy.10.1.70 [ Links ]
Dir AL, Hummer TA, Aalsma MC & Hulvershorn LA 2019. Pubertal influences on neural activation during risky decision-making in youth with ADHD and disruptive behaviour disorders. Developmental Cognitive Neuroscience, 36:100634. https://doi.org/10.1016/j.dcn.2019.100634 [ Links ]
Dirlikov B, Rosch KS, Crocetti D, Denckla MB, Mahone EM & Mostofsky SH 2015. Distinct frontal lobe morphology in girls and boys with ADHD. NeuroImage: Clinical, 7:222-229. https://doi.org/10.1016/j.nicl.2014.12.010 [ Links ]
Eskander N 2020. The psychosocial outcome of conduct and oppositional defiant disorder in children with attention deficit hyperactivity disorder. Cureus, 12(8):e9521. https://doi.org/10.7759/cureus.9521 [ Links ]
Fairchild G, Hawes DJ, Frick PJ, Copeland WE, Odgers CL, Franke B, Freitag CM & De Brito SA 2019. Conduct disorder. Nature Reviews Disease Primers, 5:43. https://doi.org/10.1038/s41572-019-0095-y [ Links ]
Faraone S, Asherson P, Banaschewski T, Biederman J, Buitelaar JK, Ramos-Quiroga JA, Rohde LA, Sonuga-Barke EJS, Tannock R & Franke B 2015. Attention-deficit/hyperactivity disorder. Nature Reviews: Disease Primers, 1(1):15020. https://doi.org/10.1038/nrdp.2015.20 [ Links ]
Ghanizadeh A & Haghighi HB 2010. How do ADHD children perceive their cognitive, affective, and behavioral aspects of anger expression in school setting? Child and Adolescent Psychiatry and Mental Health, 4(1):4. https://doi.org/10.1186/1753-2000-4-4 [ Links ]
Ghosh A, Ray A & Basu A 2017. Oppositional defiant disorder: Current insight. Psychology Research and Behavior Management, 10:353-367. [ Links ]
Ghosh S & Sinha M 2012. ADHD, ODD, and CD: Do they belong to a common psychopathological spectrum? A case series. Case Reports in Psychiatry, 2012:520689 https://doi.org/10.1155/2012/520689 [ Links ]
González RA, Vélez-Pastrana MC, McCrory E, Kallis C, Aguila J, Canino G & Bird H 2019. Evidence of concurrent and prospective associations between early maltreatment and ADHD through childhood and adolescence. Social Psychiatry and Psychiatric Epidemiology, 54:671-682. https://doi.org/10.1007/s00127-019-01659-0 [ Links ]
Harty SC, Miller CJ, Newcorn JH & Halperin JM 2009. Adolescents with childhood ADHD and comorbid disruptive behavior disorders: Aggression, anger, and hostility. Child Psychiatry & Human Development, 40(1):85-97. https://doi.org/10.1007/s10578-008-0110-0 [ Links ]
Harvey EA, Breaux RP & Lugo-Candelas CI 2016. Early development of comorbidity between symptoms of attention-deficit/hyperactivity disorder (ADHD) and oppositional defiant disorder (ODD). Journal of Abnormal Psychology, 125(2): 154-167. https://doi.org/10.1037/abn0000090 [ Links ]
Hobson CW, Scott S & Rubia K 2011. Investigation of cool and hot executive function in ODD/CD independently of ADHD. The Journal of Child Psychology and Psychiatry, 52(10):1035-1043. https://doi.org/10.1111/j.1469-7610.2011.02454.x [ Links ]
Hoza B, Mrug S, Gerdes AC, Hinshaw SP, Bukowski WM, Gold JA, Kraemer HC, Pelham WE, Jr, Wigal T & Arnold LE 2005. What aspects of peer relationships are impaired in children with attention-deficit/hyperactivity disorder? Journal of Consulting and Clinical Psychology, 73(3):411-423. https://doi.org/10.1037/0022-006X.73.3.411 [ Links ]
Humphreys KL, Aguirre VP & Lee SS 2012. Association of anxiety and ODD/CD in children with and without ADHD. Journal of Clinical Child & Adolescent Psychology, 41(3):370-377. https://doi.org/10.1080/15374416.2012.656557 [ Links ]
Humphreys KL & & Lee SS 2011. Risk taking and sensitivity to punishment in children with ADHD, ODD, ADHD+ODD, and controls. Journal of Psychopathology and Behavioral Assessment, 33:299-307. https://doi.org/10.1007/s10862-011-9237-6 [ Links ]
Jensen PS, Hinshaw SP, Kraemer HC, Lenora N, Newcorn JH, Abikoff HB, March JS, Arnold LE, Cantwell DP, Conners CK, Elloitt GR, Greenhill LL, Hechtman L, Hoza B, Pelham WE, Severe JB, Swanson JM, Wells KC, Wigal T & Vitiello B 2001. ADHD comorbidity findings from the MTA study: Comparing comorbid subgroups. Journal of the American Academy of Child & Adolescent Psychiatry, 40(2): 147-158. https://doi.org/10.1097/00004583-200102000-00009 [ Links ]
Johansen EB, Killeen PR, Russell VA, Tripp G, Wickens JR, Tannock R, Williams J & Sagvolden T 2009. Origins of altered reinforcement effects in ADHD. Behavioral and Brain Functions, 5:7. https://doi.org/10.1186/1744-9081-5-7 [ Links ]
King S & Waschbusch DA 2010. Aggression in children with attention-deficit/hyperactivity disorder. Expert Review of Neurotherapeutics, 10(10): 1581-1594. https://doi.org/10.1586/ern.10.146 [ Links ]
Kofman O, Gidley Larson J & Mostofsky SH 2008. A novel task for examining strategic planning: Evidence for impairment in children with ADHD. Journal of Clinical and Experimental Neuropsychology, 30(3):261-271. https://doi.org/10.1080/13803390701380583 [ Links ]
Kuntsi J, Wood AC, Johnson KA, Andreou P, Arias-Vasquez A, Buitelaar JK, Rommelse NNJ, Sergeant JA, Sonuga-Barke EJ, Uebel H, Van der Meere JJ, Banaschewski T, Gill M, Manor I, Miranda A, Mulas F, Oades RD, Roeyers H, Rothenberger A, Steinhausen HC, Faraone SV & Asherson P 2010. Separation of cognitive impairments in attention-deficit/hyperactivity disorder into 2 familial factors. Archives of General Psychiatry, 67(11):1159-1166. https://doi.org/10.1001/archgenpsychiatry.2010.139 [ Links ]
Lavigne JV, LeBailly SA, Hopkins J, Gouze KR & Binns HJ 2009. The prevalence of ADHD, ODD, depression, and anxiety in a community sample of 4-year-olds. Journal of Clinical Child & Adolescent Psychology, 38(3):315-328. https://doi.org/10.1080/15374410902851382 [ Links ]
Levy F, Hay DA, Bennett KS & McStephen M 2005. Gender differences in ADHD subtype comorbidity. Journal of the American Academy of Child & Adolescent Psychiatry, 44(4):368-376. https://doi.org/10.1097/01.chi.0000153232.64968.c1 [ Links ]
Liu TL, Hsiao RC, Chou WJ & Yen CF 2021. Perpetration of and victimization in cyberbullying and traditional bullying in adolescents with attention-deficit/hyperactivity disorder: Roles of impulsivity, frustration intolerance, and hostility. International Journal of Environmental Research and Public Health, 18(13):6872. https://doi.org/10.3390/ijerph18136872 [ Links ]
Luman M, Oosterlaan J & Sergeant JA 2005. The impact of reinforcement contingencies on AD/HD: A review and theoretical appraisal. Clinical Psychology Review, 25(2):183-213. https://doi.org/10.1016/jxpr.2004.11.001 [ Links ]
Marco R, Miranda A, Schlotz W, Melia A, Mulligan A, Müller U, Buttler L, Christiansen H, Gabriels I, Medad S, Albrecht B, Uebel H, Asherson P, Banaschewski T, Gill M, Kuntsi J, Mulas F, Oades R, Roeyers H, Steinhausen HC, Rothenberger A, Faraone SV & Sonuga-Barke EJS 2009. Delay and reward choice in ADHD: An experimental test of the role of delay aversion. Neuropsychology, 23(3):367-380. https://doi.org/10.1037/a0014914 [ Links ]
McBurnett K & Pfiffner LJ 2009. Treatment of aggressive ADHD in children and adolescents: Conceptualization and treatment of comorbid behavior disorders. Postgraduate Medicine, 121(6):158-165. https://doi.org/10.3810/pgm.2009.11.2084 [ Links ]
Meyer A, Eilertsen DE, Sundet JM, Tshifularo J & Sagvolden T 2004. Cross-cultural similarities in ADHD-like behaviour amongst South African primary school children. South African Journal of Psychology, 34(1):122-138. https://doi.org/10.1177/008124630403400108 [ Links ]
Mizuno Y, Kagitani-Shimono K, Jung M, Makita K, Takiguchi S, Fujisawa TX, Tachibana M, Nakanishi M, Mohri I, Taniike M & Tomoda A 2019. Structural brain abnormalities in children and adolescents with comorbid autism spectrum disorder and attention-deficit/hyperactivity disorder. TranslationalPsychiatry, 9:332. https://doi.org/10.1038/s41398-019-0679-z [ Links ]
Mordre M, Groholt B, Kjelsberg E, Sandstad B & Myhre AM 2011. The impact of ADHD and conduct disorder in childhood on adult delinquency: A 30 years follow-up study using official crime records. BMC Psychiatry, 11(1):57. https://doi.org/10.1186/1471-244X-11-57 [ Links ]
Mphahlele RM, Pillay BJ & Meyer A 2021. Delay aversion in school-aged children with attention-deficit hyperctivity disorder. South Arican Journal of Psychology, 51(4):496-506. https://doi.org/10.1177/0081246320964350 [ Links ]
Nock MK, Kazdin AE, Hiripi E & Kessler RC 2007. Lifetime prevalence, correlates, and persistence of oppositional defiant disorder: Results from the National Comorbidity Survey Replication. The Journal of Child Psychology and Psychiatry, 48(7):703-713. https://doi.org/10.1111/j.1469-7610.2007.01733.x [ Links ]
Noordermeer SDS, Luman M & Oosterlaan J 2016. A systematic review and meta-analysis of neuroimaging in oppositional defiant disorder (ODD) and conduct disorder (CD) taking attention-deficit hyperactivity disorder (ADHD) into account. Neuropsychology Review, 26(1):44-72. https://doi.org/10.1007/s11065-015-9315-8 [ Links ]
Ohan JL & Johnston C 2007. What is the social impact of ADHD in girls? A multi-method assessment. Journal of Abnormal Child Psychology, 35(2):239-250. https://doi.org/10.1007/s10802-006-9076-1 [ Links ]
Paloyelis Y, Asherson P & Kuntsi J 2009. Are ADHD symptoms associated with delay aversion or choice impulsivity? A general population study. Journal of the American Academy of Child & Adolescent Psychiatry, 48(8):837-846. https://doi.org/10.1097/CHI.0b013e3181ab8c97 [ Links ]
Pelham WE, Jr, Gnagy EM, Greenslade KE & Milich R 1992. Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 31(2):210-218. https://doi.org/10.1097/00004583-199203000-00006 [ Links ]
Pillow DR, Pelham WE, Jr, Hoza B, Molina BSG & Stultz CH 1998. Confirmatory factor analyses examining attention deficit hyperactivity disorder symptoms and other childhood disruptive behaviours. Journal of Abnomal Child Psychology, 26(4):293-309. https://doi.org/10.1023/A:1022658618368 [ Links ]
Pingali S & Sunderajan J 2014. A study of comorbidities in attention deficit hyperactivity disorder: A retrospective analysis of case records. Andhra Pradesh Journal of Psychological Medicine, 15(2):206-210. [ Links ]
Plichta MM, Vasic N, Wolf RC, Lesch KP, Brummer D, Jacob C, Fallgatter AJ & Grön G 2009. Neural hyporesponsiveness and hyperresponsiveness during immediate and delayed reward processing in adult attention-deficit/hyperactivity disorder. Biological Psychiatry, 65(1):7-14. https://doi.org/10.1016/j.biopsych.2008.07.008 [ Links ]
Polanczyk GV, Willcutt EG, Salum GA, Kieling C & Rohde LA 2014. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2):434-442. https://doi.org/10.1093/ije/dyt261 [ Links ]
Pollak Y, Dekkers TJ, Shoham R & Huizenga HM 2019. Risk-taking behavior in attention deficit/hyperactivity disorder (ADHD): A review of potential underlying mechanisms and of interventions. Current Psychiatry Reports, 21(5):33. https://doi.org/10.1007/s11920-019-1019-y [ Links ]
Puiu AA, Wudarczyk O, Goerlich KS, Votinov M, Herpertz-Dahlmann B, Turetsky B & Konrad K 2018. Impulsive aggression and response inhibition in attention-deficit/hyperactivity disorder and disruptive behavioral disorders: Findings from a systematic review. Neuroscience & Biobehavioral Reviews, 90:231-246. https://doi.org/10.1016/j.neubiorev.2018.04.016 [ Links ]
Richardson JTE 2011. Eta squared and partial eta squared as measures of effect size in educational research. Educational Research Review, 6(2):135-147. https://doi.org/10.1016/j.edurev.2010.12.001 [ Links ]
Riley M, Ahmed S & Locke A 2016. Common questions about oppositional defiant disorder. American Academy of Family Physicians. 93(7):586-591. [ Links ] Rosqvist HB & Arnell L 2018. Being a responsible violent girl? Exploring female violence, self-management, and ADHD. Girlhood Studies, 11(2):111 -126. https://doi.org/10.3167/ghs.2018.110209 [ Links ]
Rubia K 2011. "Cool" inferior frontostriatal dysfunction in attention-deficit/hyperactivity disorder versus "hot" ventromedial orbitofrontal-limbic dysfunction in conduct disorder: A review. Biological Psychiatry, 69(12):e69-e87. https://doi.org/10.1016/j.biopsych.2010.09.023 [ Links ]
Rucklidge JJ 2010. Gender differences in attention-deficit/hyperactivity disorder. Psychiatric Clinics, 33(2):357-373. https://doi.org/10.1016/j.psc.2010.01.006 [ Links ]
Sagar R, Patra BN & Patil V 2019. Clinical practice guidelines for the management of conduct disorder. Indian Journal of Psychiatry, 61(Suppl. 2):270-276. https://doi.org/10.4103/psychiatry.IndianJPsychiatry_539_18 [ Links ]
Sagvolden T, Johansen EB, Aase H & Russell VA 2005. A dynamic developmental theory of attention-deficit/hyperactivity disorder (ADHD) predominantly hyperactive/impulsive and combined subtypes. Behavioral and Brain Sciences, 28(3):397-468. [ Links ]
Shoham R, Sonuga-Barke E, Yaniv I & Pollak Y 2021. ADHD is associated with a widespread pattern of risky behaviour across activity domains. Journal of Attention Disorders, 25(7):989-1000. https://doi.org/10.1177/1087054719875786 [ Links ]
Singh I 2011. A disorder of anger and aggression: Children's perspectives on attention deficit/hyperactivity disorder in the UK. Social Science & Medicine, 73(6):889-896. https://doi.org/10.1016/j.socscimed.2011.03.049 [ Links ]
Skogli EW, Teicher MH, Andersen PN, Hovik KT & 0ie M 2013. ADHD in girls and boys - gender differences in co-existing symptoms and executive function measures. BMC Psychiatry, 13:298. https://doi.org/10.1186/1471-244X-13-298 [ Links ]
Sobanski E, Banaschewski T, Asherson P, Buitelaar J, Chen W, Franke B, Holtmann M, Krumm B, Sergeant J, Sonuga-Barke E, Stringaris M, Taylor E, Anney R, Ebstein RP, Gill M, Miranda A, Mulas F, Oades RD, Roeyers H, Rothenbergher A, Steinhaussen HC & Faraone SV 2010. Emotional lability in children and adolescents with attention deficit/hyperactivity disorder (ADHD): Clinical correlates and familial prevalence. The Journal of Child Psychology and Psychiatry, 51(8):915-923. https://doi.org/10.1111/j.1469-7610.2010.02217.x [ Links ]
Sonuga-Barke EJ, Bitsakou P & Thompson M 2010. Beyond the dual pathway model: Evidence for the dissociation of timing, inhibitory, and delay-related impairments in attention-deficit/hyperactivity disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 49(4):345-355. https://doi.org/10.1016/j.jaac.2009.12.018 [ Links ]
Sonuga-Barke EJS 2002. Psychological heterogeneity in AD/HD-a dual pathway model of behaviour and cognition. Behavioural Brain Research, 130(1-2):29-36. https://doi.org/10.1016/S0166-4328(01)00432-6 [ Links ]
StatSoft, Inc. 2011. STATISTICA (Version 10). Tulsa, OK: Author. [ Links ]
Steinhausen HC 2009. The heterogeneity of causes and courses of attention-deficit/hyperactivity disorder [Special issue]. Acta Psychiatrica Scandinavica, 120(5):392-399. https://doi.org/10.1111/j.1600-0447.2009.01446.x [ Links ]
Tripp G & Alsop B 2001. Sensitivity to reward delay in children with attention deficit hyperactivity disorder (ADHD). The Journal of Child Psychology and Psychiatry, 42(5):691-698. https://doi.org/10.1111/1469-7610.00764 [ Links ]
Tripp G & Wickens JR 2008. Research review: Dopamine transfer deficit: A neurobiological theory of altered reinforcement mechanisms in ADHD. The Journal of Child Psychology and Psychiatry, 49(7): 691-704. https://doi.org/10.1111/j.1469-7610.2007.01851.x [ Links ]
Tutian R & Shechtman Z 2015. Aggressive children with and without ADD/ADHD: A comparison of outcomes. Journal of Education and Human Development, 4(1):233-243. https://doi.org/10.15640/jehd.v4n1a21 [ Links ]
Tuvblad C, Zheng M, Raine A & Baker LA 2009. A common genetic factor explains the covariation among ADHD ODD and CD symptoms in 9-10 year old boys and girls. Journal of Abnormal Child Psychology, 37(2):153-167. https://doi.org/10.1007/s10802-008-9278-9 [ Links ]
Van Hulst BM, De Zeeuw P, Vlaskamp C, Rijks Y, Zandbelt BB & Durston S 2018. Children with ADHD symptoms show deficits in reactive but not proactive inhibition, irrespective of their formal diagnosis. Psychological Medicine, 48(15):2515-2521. https://doi.org/10.1017/S0033291718000107 [ Links ]
Van Lier PAC, Van der Ende J, Koot HM & Verhulst FC 2007. Which better predicts conduct problems? The relationship of trajectories of conduct problems with ODD and ADHD symptoms from childhood into adolescence. The Journal of Child Psychology and Psychiatry, 48(6):601-608. https://doi.org/10.1111/j.1469-7610.2006.01724.x [ Links ]
White BA, Jarrett MA & Ollendick TH 2013. Self-regulation deficits explain the link between reactive aggression and internalizing and externalizing behavior problems in children. Journal of Psychopathology and Behavioral Assessment, 35(1):1-9. https://doi.org/10.1007/s10862-012-9310-9 [ Links ]
Winstok Z 2009. From self-control capabilities and the need to control others to proactive and reactive aggression among adolescents. Journal of Adolescence, 32(3):455-466. https://doi.org/10.1016/j.adolescence.2008.08.006 [ Links ]
Young S, Adamo N, Ásgeirsdóttir BB, Branney P, Beckett M, Colley W, Cubbin, S, Deeley Q, Farrag E, Gudjonsson G, Hill P, Hollingdale J, Kilic O, Lloyd T, Mason P, Paliokosta E, Perecheria S, Sedgwick J, Skirrow C, Tierney K, Van Rensburg K & Woodhouse E 2020. Females with ADHD: An expert consensus statement taking a lifespan approach providing guidance for the identification and treatment of attention-deficit/hyperactivity disorder in girls and women. BMC Psychiatry, 20(1):404. https://doi.org/10.1186/s12888-020-02707-9 [ Links ]
Yu X, Sonuga-Barke E & Liu X 2018. Preference for smaller sooner over larger later rewards in ADHD: Contribution of delay duration and paradigm type. Journal of Attention Disorders, 22(10):984-993. https://doi.org/10.1177/1087054715570390 [ Links ]
Received: 10 November 2020
Revised: 15 October 2021
Accepted: 12 May 2022
Published: 28 February 2023


{kind=link}