










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Education
On-line version ISSN 2076-3433
Print version ISSN 0256-0100
S. Afr. j. educ. vol.41 n.1 Pretoria Feb. 2021
http://dx.doi.org/10.15700/saje.v41n1a1830
ARTICLES
Striving for equity: Life orientation resources in South African high schools
Andre van Zyl; Elizabeth M. Webb; Jaqueline E. Wolvaardt
School of Health Systems and Public Health, Faculty of Health Sciences, University of Pretoria, Pretoria, South Africa. liz.wolvaardt@up.ac.za
ABSTRACT
As a school subject, life orientation (LO) aims to improve learner well-being, but a lack of classroom resources may be a barrier. We investigated whether classroom resources were equally available for LO educators in fully funded (no-fee) and partially funded (fee-paying) high schools in Tshwane South, South Africa. In this analytical cross-sectional study, LO representatives completed questionnaires about the availability of resources in their schools. Sixty-seven LO representatives completed the questionnaire. No-fee and fee-paying schools had the same availability of government resources and textbooks, but no-fee schools had less access to audio-visual equipment and printed materials. Representatives from both categories of schools were least satisfied with the availability of resources for the topic: Health. In contrast, they thought that the resources for non-health related topics such as career and skills-development were adequate. Representatives from no-fee schools were less satisfied with physical education resources (U (56) = -2.29, p = 0.02). The government's efforts to redress inequity is evident in the availability of basic resources. However, a lack of health resources is a source of concern in a society that has a quadruple burden of disease.
Keywords: equity; health education; life orientation; resources; school
Introduction
The South African Department of Health has prioritised the strengthening of school health services in the process of re-engineering primary health care (Pillay, Y 2012). School-based health education is effective in reducing risk behaviour, promoting health-related skills, and increasing health-related knowledge (Fonner, Armstrong, Kennedy, O'Reilly & Sweat, 2014). To this end, the South African Department of Basic Education introduced the compulsory subject, LO, aiming to improve the health and well-being of learners (DBE, 2011a, 2011b).
Life orientation is a mandatory subject for all learners from Grade R (reception year before starting school) onwards to grade 12, which generally corresponds to learner ages 6 through 18 years. The subject is a combination of "health education, life skills, career guidance, physical education, human rights education, and religious education" and may contribute to solving social issues such as poverty, abuse, violence, sexually transmitted infections, social breakdown, and unsafe environments (Pillay, J 2012:167). If teachers and schools are adequately and equitably resourced to provide LO education, we believe that LO could serve to realise the third Sustainable Development Goal (SDG) of good health in South Africa (Sachs, 2012).
Literature Review
Life orientation educators follow the South African National Curriculum and Assessment Policy Statement (CAPS), which standardises the LO curriculum (DBE, 2011a, 2011b). The CAPS curriculum outlines LO educational timelines, topics to be covered by educators, assessment guidelines and recommended resources. Historically, resources in the South African schooling system were unequally distributed along racial lines, inequities that have been perpetuated by the decision by some schools to charge fees (DBE, 2017; Organisation for Economic Co-operation and Development [OECD], 2013; Spaull, 2013). To overcome these differences, the government strives to provide equitable basic education for all by providing funding to public schools that are in need (Republic of South Africa [RSA], 1996). The government system classifies public schools according to five quintile rankings based on the community surrounding each school (DBE, 2017). The rankings consider household income, dependency ratio, unemployment level and level of education (OECD, 2013). Quintile 1 to 3 (Q1-3) schools are located in the lowest socio-economic areas and are fully funded by the government. These schools are also referred to as no-fee schools (DBE, 2017). Quintile 4 and 5 (Q4 & 5) schools are partially government-funded, while independent schools are fully funded by parents with no government funding (DBE, RSA, 2015). Independent and Q4 and 5 schools are associated with higher socioeconomic status (SES) areas and are referred to as fee-paying schools.
The resources available in a school may depend on the SES of the school population, with low SES schools expected to have fewer resources (Summersett-Ringgold, Li, Haynie & Iannotti, 2015). In South Africa, no-fee schools serving the most impoverished communities, are not allowed to collect tuition fees, which often results in a shortage of educators, insufficient funds to obtain additional resources, and in poorer educational outcomes (OECD, 2013). Fee-paying schools may collect tuition fees allowing the schools to employ additional staff, have better facilities, have easier access to academic materials, and provide extracurricular activities (OECD, 2013; Summersett-Ringgold et al., 2015). Additionally, parents associated with these schools have the means to provide additional resources to their children due to their own education, access to material resources, and community resources.
The CAPS LO curriculum addresses a broad variety of topics, from physical education to career information, and requires many resources to be implemented successfully (Jacobs & Frantz, 2014). The unequal distribution of resources between no-fee and fee-paying schools may lead to differences in the success of implementing the LO curriculum (Summersett-Ringgold et al., 2015). Previous studies have identified that a shortage of educational resources and continuous professional development (CPD) for LO educators are barriers to the successful implementation of LO (Jacobs & Frantz, 2014; Peu, Napoles, Wenhold, Mostert-Wentzel & Seane, 2010). Due to the lack of resources, learners in under-resourced schools may have less exposure to useful LO information that could improve their quality of life.
Various resources available to parents and LO educators could potentially aid in LO education and school health promotion (Akintola, Lavis & Hoskins, 2015; DBE, 2011a, 2011b; Iudici, 2015; Kazemian, Ghasemi, Movahhed & Kazemian, 2014; Mitu, 2016; Nunes, Daly, Rao, Borntrager, Chambers, Rohner & Shrestha, 2010; Papastergiou, 2009; Peralta, Dudley & Cotton, 2016; Peu et al., 2010). School-based resources include resources for physical education, textbooks, health literature, televisions (TVs), radios, information technology resources, facility resources, printed resources, and CPD for educators. External community resources include religious organisations, health organisations, universities, research projects, and support groups.
Theoretical Framework
Health education theories range from theories that view health education from a deficit perspective such as problem behaviour to those that focus on positive long-term effects. All health education theories share the notion of behavioural change. Problem behaviour theory views negative health-related behaviour as inevitable and, in adolescent health at least, tries to delay the onset, minimize the effect and protect the learner from the consequences of the behaviour (Vadrucci, Vigna-Taglianti, Van der Kreeft, Vassara, Scatigna, Faggiano, Burkhart & The EU-Dap Study Group, 2016). In school health education, social learning theory is popular because educational techniques, such as skills training, are used to translate theory into practice (Parcel, GS 1984). In social learning theory, the social environment is key to learning and plays a role in reinforcing the educational intervention. Other behavioural change theories that highlight the role of the social environment are the "social support and family" theories (Bickerton, Ward, Southgate & Hense, 2014; Feeney & Collins, 2015; Gordon, Almudaihim, Shelnutt, Vilaro, Colby & Mathews, 2017; McCann, Perra, McLaughlin, McCartan & Higgins, 2016; Parcel, TL & Bixby, 2016). While social learning theory includes the role of learning or knowledge creation within the school environment, the social support and family theory focusses on the family unit rather than reinforcing what is learnt at school.
In school health education, the role of attitudes in behavioural change can be explained by two theories, namely the theory of reasoned action (Hackman & Knowlden, 2014) and communication theories (Edgar & Volkman, 2012). The theory of reasoned action is a behavioural intention model that explains that an individual's intention to adopt a certain behaviour is a function of attitude, normative beliefs about what others think he or she should do, weighted by a motivation to comply (Fishbein & Ajzen, 2010). This theory has been particularly useful in promoting positive (e.g. promote attitudes and skills for safer sex), and managing negative health behaviours (e.g. reducing risky sexual behaviours) (Atwood, Kennedy, Shamblen, Tegli, Garber, Fahnbulleh, Korvah, Kolubah, Mulbah-Kamara & Fulton, 2012; Michielsen, Beauclair, Delva, Roelens, Van Rossem & Temmerman, 2012). In health education research, communication theory focusses on persuasion to change people's attitudes and behaviours (Edgar & Volkman, 2012).
The third group of health education theories aspire to change both the short-term and long-term behaviour of learners. These theories focus on the development of the learner to be able to solve problems and analyse their own choices or behaviour. Self-control (Duckworth, Gendler & Gross, 2014; Duckworth & Steinberg, 2015), coping theory (Chua, Milfont & Jose, 2015; Gulliford, Deans, Frydenberg & Liang, 2015) and social-emotional competence (Domitrovich, Durlak, Staley & Weissberg, 2017; Low, Cook, Smolkowski & Buntain-Ricklefs, 2015) are three theories used in school health education. Self-control is a component of other theories such as social learning theory and aims to develop learners' ability to solve problems and understand their own behaviour. Coping theory focusses on the individual's ability to cope with stress and, therefore, indirectly prevents negative health behaviour used to cope with stress, such as smoking, drinking and overeating. Within a school environment, coping theory within health education aims to teach learners how to cope with stress and become more resilient. Social competence theory is similar to both the self-control and coping theories in that the focus is on the long-term development of skills and competencies to deal with complex and unknown challenges. Except for the social support and family theory, all these theories are predicated on building knowledge within the school environment as an element of behavioural change. Irrespective of the health education theory that educators use, building health-related knowledge in a school environment depends on the availability of appropriate resources, including our own perspective of ensuring behavioural change by using social learning theory.
If all schools do not have the same LO resources available, then the inequalities of the past and the substantial burden of disease will remain a constant in the lives of South Africans. The aim of the research reported on here was to describe the current provision of LO resources in the Tshwane South district. The research objectives were to: identify which health education resources are available; determine if there is a difference in the amount of health education resources available; determine the level of satisfaction that LO educators have with the availability of health education resources.
Methods
The theory of social learning, similar to other health education theories, requires resources in the classroom. We used an analytical cross-sectional study design with data obtained through a self-administered questionnaire to determine resource availability. This study design was deemed suitable as our objective was to investigate the current availability of LO resources rather than whether, or how, the resources are used or their effectiveness.
Participants
In the Tshwane South district, there are 120 high schools providing LO tuition for learners from grade 8 to 12 (DBE, RSA, 2015). Among these 103 (85.8%) schools are classified as fee-paying (Q4 & 5) schools, while 17 (14.2%) are classified as no-fee schools (Q1-3). The study sample consisted of LO representatives from both fee-paying and no-fee schools from the Tshwane South district who attended a quarterly cluster meeting. The representatives included LO Head of Departments (HODs), LO educators and other LO representatives.
Instrumentation
We compiled a questionnaire based on the recommended resources suggested by the LO CAPS document.
In this study, we merged all high school (Grades 8-12) LO CAPS topics into eight topics: (1) Development of the self in society, (2) Health, (3) Social responsibility, (4) Environmental responsibility, (5) Constitutional rights and responsibilities, (6) Careers and career choices, (7) Study skills, and (8) Physical education.
We also added questions on additional resources identified in the literature such as community resources, information and communications technologies, and facility resources (DBE, 2011a, 2011b; Iudici, 2015; Kazemian et al., 2014; Mitu, 2016; Nunes et al., 2010; Papastergiou, 2009; Peu et al., 2010). The questionnaire comprised of 47 questions. Of these, 32 questions had yes/no/unsure as options, and eight visual analogue scale questions used to determine participants' level of satisfaction with available resources per LO theme. The visual analogue scale consisted of 10-centimetre lines with sad and happy faces on either side of the scale. The participants indicated their satisfaction by making a cross on the scale. We measured the responses with a ruler to arrive at a score out of 100. We classified satisfaction scores below 50 as "not satisfied" and above 50 as "satisfied." The questionnaire also contained five open-ended questions to which could list formal or informal resources available in their schools, in their communities, health education resources for LO, internet resources, and resources they still required. The questionnaire was pre-tested to determine clarity by researchers and education students.
Procedure
This research was approved by the Research Ethics Committee of the Faculty of Health Sciences at the University of Pretoria (Approval 151/2016) and the Gauteng Department of Education in Tshwane. The questionnaire was distributed at a quarterly LO cluster meeting held on 24 August 2016. The chair of the meeting introduced the study to representatives and invited them to participate. All respondents voluntarily signed informed consent forms.
Data Analysis
The data were stratified according to fee-paying and no-fee schools. Data were analysed with STATA version 13 (StataCorp, 2013). We used descriptive statistics and Chi-square statistics to determine whether the availability of resources differed between the fee-paying and no-fee schools. We used /-tests to determine the differences between schools. A p-value of less than 0.05 was regarded as significant. The listed responses to the open-ended questions were categorised and summarised.
Results
Of the 96 LO representatives who attended the quarterly cluster meeting, 67 completed the survey, resulting in a response rate of 69.8%. Eight respondents (11.9%) did not provide the names of their schools. Since we could not determine these schools' quintiles, we did not use these questionnaires to determine differences between fee-paying and no-fee schools. These questionnaires were included in descriptive statistics.
Most of the LO representatives (71.6%, n = 48) were from fee-paying schools, and 16.4% (n = 11) from no-fee schools (Table 1). More than half (55.2%, n = 37) of respondents were from public schools (all quintiles). Independent schools were represented by 32.8% (n = 22) of the respondents. Most respondents (80.6%, n = 54) were from urban schools. Approximately one-third of respondents (34.3%, n = 23) were HODs from fee-paying schools compared to three (4.5%) from no-fee schools.
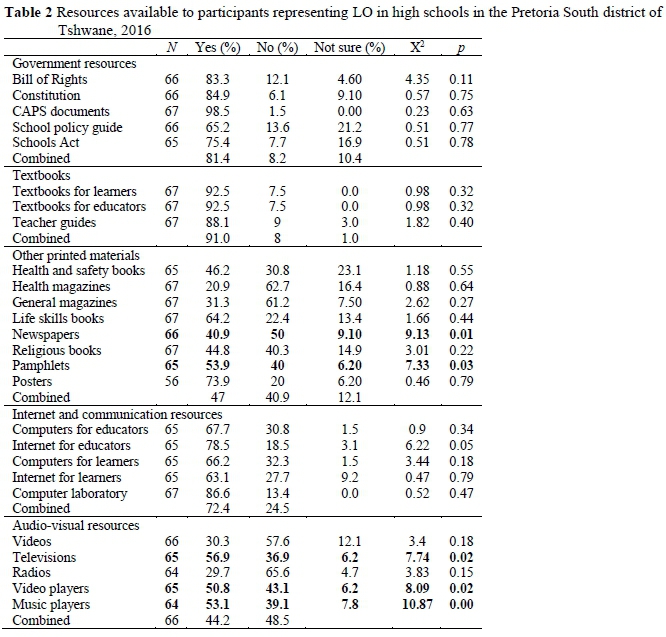
Availability of Government Resources and Textbooks
Fee-paying and non-fee schools had the same availability of government resources (Table 2). Representatives from almost all schools (81%) had access to government resources and 91% had access to textbooks for learners, textbooks for educators, and teacher guides (Table 2).
Availability of Other Printed Materials
Almost half (47%) of all schools had access to other printed materials (Table 2). Most schools had access to posters (73.9%) and only 20.9% of schools had access to health magazines. Significantly more fee-paying schools had access to newspapers (X2(1, N= 58) = 9.1, p = 0.01) and pamphlets (X2(1, N = 57) = 7.3, p = 0.03) compared to non-fee schools.
Availability of Internet, Communication and Audio-Visual Resources
Fee-paying and no-fee schools had the same access to technology resources. Most schools (72%) had access to computers for internet and communication resources (Table 2). Only 44.2% of all schools had access to audio-visual resources including videos, TV, radio, video players, and music players (Table 2). Fee-paying schools had significantly greater access to audio-visual resources, including TVs (X2(1, N = 57) = 7.7, p = 0.02), video players (X2(1, N = 57) = 8.1, p = 0.02) and music players (X2(1, N = 57) = 10.9, p = 0.0) compared to no-fee schools.
Formal and Informal Community Resources Available to Schools
When asked to list community resources, including formal or informal resources in their schools or communities, 48 respondents from fee-paying schools listed 128 responses, while the 11 respondents from no-fee schools listed 28 responses.
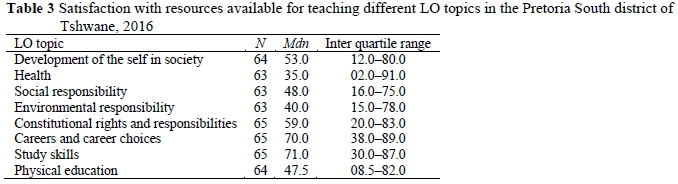
Satisfaction with Available Resources for Each LO Topic
Representatives expressed highest satisfaction (71.0%) with resources available for teaching study skills, while representatives were least satisfied (35%) with the resources available for teaching health (Table 3).
Adequacy of Resources for Health Education
When asked about the adequacy of resources available for teaching health topics, 25.4% (n = 17) of representatives were of the opinion that their schools had adequate resources. The same proportion of representatives from fee-paying and no-fee schools reported inadequate resources X2(1, N = 47) = 0.14, p = 0.7).
The Shapiro-Wilk test indicated that the data from the visual analogue scales were not normally distributed. Therefore, we used the two-sample Wilcoxon rank-sum (U) test, to test whether satisfaction with available resources differed between no-fee and fee-paying schools (Table 4). Representatives from fee-paying and no-fee schools were equally satisfied with resources available for teaching seven of the eight LO topics. Representatives from no-fee schools (Table 4) were significantly less satisfied with the resources available for teaching physical education (U (56) = -2.29, p = 0.02).
Perceptions of Resources Needed for LO
Representatives from fee-paying schools listed 83 resources needed for health education, while representatives from no-fee schools listed 10 resources. Both types of schools required community resources (e.g. community programmes, councillors) as well as primary health care resources (e.g. books, videos). Both types of schools reported needing physical education equipment. Representatives from fee-paying schools listed low-cost items such as balls. In contrast, representatives from no-fee schools listed sports coaches and facilities. Representatives from fee-paying schools listed additional human resources such as mental health care professionals, which were not mentioned by representatives from no-fee schools. Compared to fee-paying schools, representatives from no-fee schools did not list a need for web resources.
Continuous Professional Development Opportunities
Forty-eight (71.6%) representatives had access to CPD opportunities at their schools. Six representatives (9%) were unsure, and two (3%) representatives did not respond. Representatives from fee-paying and no-fee paying schools had equal access to CPD opportunities at their schools (X2(1, N = 67) = 3.5, p = 0.7).
Discussion
The results from the research indicate that high schools in Tshwane South did not have the same access to all resources. Representatives from fee-paying schools had a perceived need for many smaller items, while representatives from no-fee schools had a perceived need for more institutional resources, such as sporting facilities and coaches.
All schools had access to government resources and textbooks. This positive finding reflects the government's commitment to providing the basic resources needed for meeting the objectives of the LO curriculum (Kazemian et al., 2014). Compared to fee-paying schools, no-fee schools did not have access to newspapers and pamphlets that often contain important and current information on health topics (Akintola et al., 2015). The lack of newspapers in these schools may reflect the parents' economic reality while the lack of pamphlets may be explained by LO educators' possible lack of awareness of community resources. While the lack of printed material may be a problem, printed material may also promote unhealthy products (Chapman, Fairchild & Morgan, 2014). Skilful educators should curate printed material from popular media, and educate learners on information promoting unhealthy behaviour and products.
With the increasing access to internet technology, the youth are using technology at progressively younger ages, including searching for health information (Duduciuc, 2016). The large amounts of online health content make finding information about specific health concerns easy (Nunes et al., 2010). Both fee-paying and no-fee schools had the same level of access to information and communication technology (ICT) resources, and representatives did not mention a need for ICT resources in the open-ended questions. It was encouraging that both types of schools listed similar access to ICT resources, which are important for learning digital skills relevant in the current economy, improving access to information and reducing the costs of tuition. In particular, computer and video games could be used to address the most urgent needs such as health education and physical education (Institute of Digital Media and Child Development Working Group on Games for Health, Baranowski, Blumberg, Buday, DeSmet, Fiellin, Green, Kato, Lu, Maloney, Mellecker, Morrill, Peng, Shegog, Simons, Staiano, Thompson & Young, 2016; Papastergiou, 2009). One key example is the use of ICT to promote the mental health of learners (Nunes et al., 2010). In our study, only representatives from fee-paying schools listed a need for additional web-based resources, which could be due to a better awareness of potential external resources. It should be noted that all the schools in this study were located in an urban area.
We observed that fee-paying schools had greater access to TVs, music players, and video players, which were less available in no-fee schools. The difference in availability could be explained by the higher cost of these resources, making them less affordable to no-fee schools. However, these resources were absent in most schools in this study. Current literature does not explore the use of these technologies, but rather focuses on the use of ICT resources for health education. Audio-visual resources for health education might, therefore, be obsolete.
Community resources are able to promote child health but are seldom used (Tweneboa-Kodua, Obeng-Quaidoo & Abu, 1991). This supports our finding that representatives did not list many community resources, including formal or informal resources, in their schools and other resources in their communities. Representatives in fee-paying schools had a greater collective awareness of resources available to teach LO because they mentioned more and a greater variety of community resources. The sparse list of community resources may also indicate educators' lack of awareness of available resources, rather than a lack of available resources in their communities. For example, findings suggest that teachers were not always aware of the warning signs of suicidal behaviour which required mental health interventions (Shilubane, Bos, Ruiter, Van den Borne & Reddy, 2015). The Department of Education should form links within the community to help support teachers. This is especially important for managing mental health, reproductive health and substance abuse in vulnerable teenage populations.
In this study, representatives from fee-paying and no-fee schools were equally satisfied with the availability of resources for most LO topics, including health. Despite the lack of statistical significance, the wide interquartile ranges suggest that the availability of resources differs between individual schools. Representatives from no-fee schools were largely dissatisfied with the availability of physical education resources, a view also expressed in the open-ended questions. We did not explore whether LO educators overcame the lack of resources by using innovative methods or whether learners from fee-paying and no-fee schools had the same level of physical activity. Evidence suggests that access to physical education equipment promotes physical activity (Bevans, Fitzpatrick, Sanchez, Riley & Forrest, 2010). Representatives from no-fee schools expressed a need for expensive physical resources, including sports coaches and facilities. The lack of physical resources could be overcome by using affordable resources like playground markings and physical structures (Escalante, García-Hermoso, Backx & Saavedra, 2014). Walter (2014) suggests low-cost physical activity resources that could be installed with the support of the community.
In general, representatives showed low satisfaction with the availability of resources depending on the LO topic and the school. Representatives showed a high level of satisfaction with the availability of resources to improve career outcomes and study skills. Improved career outcomes could increase learners' future income potential, which could also reduce health inequality (Pickett & Wilkinson, 2015). However, neither careers and career choices nor study skills were health-specific so it is important to ensure that health-specific education resources are available to improve learners' immediate health behaviour (Fonner et al., 2014).
According to Jita and Mokhele, clustering teachers is a relatively new strategy for providing CPD to educators. Educator cluster meetings serve to improve education knowledge and practices aimed at enhancing the educational outcomes of learners (Jita & Mokhele, 2014). Representatives from both fee-paying and no-fee schools had access to CPD meetings, indicating that the local department of education attempted to include all educators from different communities.
Limitations
The cross-sectional study design is limiting as it can only provide a snapshot in time. Our use of a non-validated instrument may have affected the reliability of the data. The questionnaires were self-administered, which could lead to response bias. Few representatives from no-fee participated in the study, which could explain the sparse list of community resources mentioned. Educators may also be unaware of the resources available to them for health education. For example, educators who are not exposed to the internet might be unaware of online teaching resources.
Conclusion
Both fee-paying and no-fee schools had access to basic resources for LO, reflecting the equitable funding system of the Gauteng Department of Education and the provision of the most basic resources. Representatives from fee-paying and no-fee schools were generally dissatisfied with the availability of health-related resources. This lack of resources is a source of concern as the provision of resource material in the classroom is a required component for the social learning theory as well as many of the other health education theories. South Africans are unlikely to be able to reduce the quadruple burden of disease and make progress towards achieving SDG 3 if this learning opportunity is sub-optimal. Education research should determine the best strategies for overcoming shortcomings and assessing the impact of the lack of resources on learners. Further research is required to explore the correlation between resource availability, LO grades and health outcomes.
Acknowledgements
The authors would like to thank all the participants for their participation and the Gauteng Department of Education in Tshwane for their support and assistance.
Authors' Contributions
AvZ planned this research under the guidance of EMW and JEW. AvZ conducted the data collection and all statistical analysis was done by AvZ and EMW. JEW and EMW led the interpretation of the findings. AvZ prepared the first draft of the manuscript, which was edited by EMW and JEW. All authors reviewed the final manuscript.
Notes
i. Published under a Creative Commons Attribution Licence.
ii. DATES: Received: 11 February 2019; Revised: 22 January 2020; Accepted: 11 March 2020; Published: 28 February 2021.
References
Akintola O, Lavis JN & Hoskins R 2015. Print media coverage of primary healthcare and related research evidence in South Africa. Health Research Policy and Systems, 13:68. https://doi.org/10.1186/s12961-015-0051-6 [ Links ]
Atwood KA, Kennedy SB, Shamblen S, Tegli J, Garber S, Fahnbulleh PW, Korvah PM, Kolubah M, ulbah-Kamara C & Fulton S 2012. Impact of chool-based HIV prevention program in post-conflict Liberia. AIDS Education and Prevention, 24(1):68-77. https://doi.org/10.1521/aeap.2012.24.L68 [ Links ]
Bevans KB, Fitzpatrick LA, Sanchez BM, Riley AW & Forrest C 2010. Physical education resources, class management, and student physical activity levels: A structure-process-outcome approach to evaluating physical education effectiveness. Journal of School Health, 80(12):573-580. https://doi.org/10.1111/j.1746-1561.2010.00544.x [ Links ]
Bickerton A, Ward J, Southgate M & Hense T 2014. The afety First Assessment Intervention: A whole family approach for young people with high risk mental health presentations. Australian & New Zealand Journal of Family Therapy, 35(2): 150-8. https://doi.org/10.1002/anzf.1055 [ Links ]
Chapman KJ, Fairchild RM & Morgan MZ 2014. Food references in UK children's magazines - an oral health perspective. British Dental Journal, 217:E20. https://doi.org/10.1038/sj.bdj.2014.1007 [ Links ]
Chua LW, Milfont TL & Jose PE 2015. Coping skills help explain how future-oriented adolescents accrue greater well-being over time. Journal of Youth and Adolescence, 44:2028-2041. https://doi.org/10.1007/s10964-014-0230-8 [ Links ]
Department of Basic Education 2011a. Curriculum and Assessment Policy Statement Grades 7-9: Life Orientation. Pretoria, South Africa: Author. [ Links ]
Department of Basic Education, Republic of South frica 2011b. Curriculum and Assessment Policy Statement Grades 10-12: Life Orientation. Pretoria: Author. Available at https://www.education.gov.za/Portals/0/Documents/Publications/CAPS%20Commnets/FET/LIFE%20ORIENTATION%20GRADES%2010%20-%2012%20EDiTED.PDF?ver=2018-08-29-154752-423. Accessed 9 February 2021. [ Links ]
Department of Basic Education, Republic of South Africa 2015. School masterlist data: Gauteng. Available at https://www.education.gov.za/Programmes/EMIS/EMISDownloads.aspx. Accessed 27 February 017. [ Links ]
Department of Basic Education 2017. South African chools Act (84/1996): Amended National Norms and Standards for School Funding. Government Gazette, 622(40818), April 28. Available at https://www.gov.za/documents/south-african-schools-act-national-norms-and-standards-school-funding-amendment-28-apr. Accessed 4 March 018. [ Links ]
Domitrovich CE, Durlak JA, Staley KC & Weissberg RP 017. Social-emotional competence: An essential factor for promoting positive adjustment and reducing risk in school children. Child Development, 88(2):408-416. https://doi.org/10.1111/cdev.12739 [ Links ]
Duckworth AL, Gendler TS & Gross JJ 2014. Self-cntrol in school-age children. Educational Psychologist, 49(3):199-217. https://doi.org/10.1080/00461520.2014.926225 [ Links ]
Duckworth AL & Steinberg L 2015. Unpacking self-control. Child Development Perspectives, 9(1):32- 37. https://doi.org/10.1111/cdep.12107 [ Links ]
Duduciuc A 2016. Teenagers, risk behaviours and the use of new technologies for health. In V Marinescu & B Mitu (eds). The power of the media in health communication. New York, NY: Routledge. [ Links ]
Edgar T & Volkman JE 2012. Using communication theory for health promotion: Practical guidance on message design and strategy. Health Promotion Practice, 13(5):587-590. https://doi.org/10.1177/1524839912450879 [ Links ]
Escalante Y, García-Hermoso A, Backx K & Saavedra JM 2014. Playground designs to increase physical activity levels during school recess: A systematic review. Health Education & Behavior, 41(2): 138- 144. https://doi.org/10.1177/1090198113490725 [ Links ]
Feeney BC & Collins NL 2015. A new look at social support: A theoretical perspective on thriving through relationships. Personal and Social Psychology Review, 19(2):113-147. https://doi.org/10.1177/1088868314544222 [ Links ]
Fishbein M & Ajzen I 2010. Predicting and changing behavior: The reasoned action approach. New York, NY: Psychology Press. [ Links ]
Fonner VA, Armstrong KS, Kennedy CE, O'Reilly KR & Sweat MD 2014. School based sex education and HIV prevention in low- and middle-income countries: A systematic review and meta-analysis. PLoS One, 9(3):e89692. https://doi.org/10.1371/journal.pone.0089692 [ Links ]
Gordon S, Almudaihim A, Shelnutt K, Vilaro M, Colby S & Mathews A 2017. The impact of family structure on perceived social support for health behaviors of incoming college freshmen. Journal of the Academy of Nutrition and Dietetics, 117(10):A144. https://doi.org/10.1016/jjand.2017.08.095 [ Links ]
Gulliford H, Deans J, Frydenberg E & Liang R 2015. Teaching coping skills in the context of positive parenting within a preschool setting. Australian Psychologist, 50(3):219-231. https://doi.org/10.1111/ap.12121 [ Links ]
Hackman CL & Knowlden AP 2014. Theory of reasoned action and theory of planned behavior-based dietary interventions in adolescents and young adults: A systematic review. Adolescent Health, Medicine and Therapeutics, 5:101-114. https://doi.org/10.2147/AHMT.S56207 [ Links ]
Institute of Digital Media and Child Development Working Group on Games for Health, Baranowski T, Blumberg F, Buday R, DeSmet A, Fiellin LE, Green CS, Kato PM, Lu AS, Maloney AE, Mellecker R, Morrill BA, Peng W, Shegog R, Simons M, Staiano AE, Thompson D & Young K 2016. Games for health for children - current status and needed research. Games for Health Journal, 5(1):1-12. https://doi.org/10.1089/g4h.2015.0026 [ Links ]
Iudici A (ed.) 2015. Health promotion in school: Theory, practice and clinical implications. Hauppauge, NY: Nova Science. [ Links ]
Jacobs H & Frantz JM 2014. Development of a Life Orientation health education programme for high school learners. African Journal for Physical, Health Education, Recreation and Dance, 20(Suppl. 2):69-78. [ Links ]
Jita LC & Mokhele ML 2014. When teacher clusters work: Selected experiences of South African teachers with the cluster approach to professional development. South African Journal of Education, 34(2):Art. # 1790, 15 pages. https://doi.org/10.15700/201412071132 [ Links ]
Kazemian R, Ghasemi H, Movahhed T & Kazemian A 2014. Health education in primary school textbooks in Iran in school year 2010-2011. Journal of Dentistry of Tehran University of Medical Sciences, 11(5):536-544. Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4290773/pdf/jod-11-536.pdf. Accessed 8 February 2021. [ Links ]
Low S, Cook CR, Smolkowski K & Buntain-Ricklefs J 2015. Promoting social-emotional competence: An evaluation of the elementary version of Second Step®. Journal of School Psychology, 53(6):463-477. https://doi.org/10.1016/jjsp.2015.09.002 [ Links ]
McCann M, Perra O, McLaughlin A, McCartan C & Higgins K 2016. Assessing elements of a family approach to reduce adolescent drinking frequency: Parent-adolescent relationship, knowledge management and keeping secrets. Addiction, 111(5):843-853. https://doi.org/10.1111/add.13258 [ Links ]
Michielsen K, Beauclair R, Delva W, Roelens K, Van Rossem R & Temmerman M 2012. Effectiveness of a peer-led HIV prevention intervention in secondary schools in Rwanda: Results from a non-randomized controlled trial. BMC Public Health, 12:729. https://doi.org/10.1186/1471-2458-12-729 [ Links ]
Mitu B 2016. Health in the digital era: Searching health information online. In V Marinescu & B Mitu (eds). The power of the media in health communication. New York, NY: Routledge. [ Links ]
Nunes D, Daly B, Rao K, Borntrager C, Chambers KL, Rohner K & Shrestha S 2010. Technology in child and adolescent and school mental health: A look at today and tomorrow. Advances in School Mental Health Promotion, 3(3):26-35. https://doi.org/10.1080/1754730X.2010.9715684 [ Links ]
Organisation for Economic Co-operation and Development 2013. OECD Economic surveys: South Africa 2013. Paris, France: OECD Publishing. https://doi.org/10.1787/eco_surveys-zaf-2013-en [ Links ]
Papastergiou M 2009. Exploring the potential of computer and video games for health and physical education: A literature review. Computers & Education, 53(3):603-622. https://doi.org/10.1016/j.compedu.2009.04.001 [ Links ]
Parcel GS 1984. Theoretical models for application in school health education research. Journal of School Health, 54(6):39-49. https://doi.org/10.1111/j.1746-1561.1984.tb09735.x [ Links ]
Parcel TL & Bixby MS 2016. The ties that bind: Social capital, families, and children's well-being. Child Development Perspectives, 10(2):87-92. https://doi.org/10.1111/cdep.12165 [ Links ]
Peralta LR, Dudley DA & Cotton WG 2016. Teaching healthy eating to elementary school students: A scoping review of nutrition education resources. Journal of School Health, 86(5):334-345. https://doi.org/10.1111/josh.12382 [ Links ]
Peu MD, Napoles L, Wenhold F, Mostert-Wentzel K & Seane N 2010. Health education training needs of educators at Makapanstad schools in the North West province. Curationis, 33(1):33-41. Available at http://www.scielo.org.za/pdf/cura/v33n1/04.pdf. Accessed 7 February 2021. [ Links ]
Pickett KE & Wilkinson RG 2015. Income inequality and health: A causal review. Social Science & Medicine, 128:316-326. https://doi.org/10.1016Zj.socscimed.2014.12.031 [ Links ]
Pillay J 2012. Keystone Life Orientation (LO) teachers: Implications for educational, social, and cultural contexts. South African Journal of Education, 32(2):167-177. https://doi.org/10.15700/saje.v32n2a497 [ Links ]
Pillay Y 2012. PHC re-engineering in South Africa: Are we making progress? Rosebank, South Africa: Public Health Association of South Africa. Available at https://www.phasa.org.za/wp-content/uploads/2012/02/Pillay_PHC-re-engineering.pdf. Accessed 14 May 2019. [ Links ]
Republic of South Africa 1996. Act No. 84, 1996: South African Schools Act, 1996. Government Gazette, 377(17579), November 15. [ Links ]
Sachs JD 2012. From Millennium Development Goals to Sustainable Development Goals. The Lancet, 379(9832):2206-2211. https://doi.org/10.1016/s0140-6736(12)60685-0 [ Links ]
Shilubane HN, Bos AER, Ruiter RAC, Van den Borne B & Reddy PS 2015. High school suicide in South Africa: Teachers' knowledge, views and training needs. BMC Public Health, 15:245. https://doi.org/10.1186/s12889-015-1599-3 [ Links ]
Spaull N 2013. Poverty and privilege: Primary school inequality in South Africa. International Journal of Educational Development, 33(5):436-447. https://doi.org/10.1016/j.ijedudev.2012.09.009 [ Links ]
StataCorp 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP. [ Links ]
Summersett-Ringgold FC, Li K, Haynie DL & Iannotti RJ 2015. Do school resources influence the relationship between adolescent financial background and their school perceptions? Journal of School Health, 85(7):413-422. https://doi.org/10.1111/josh.12267 [ Links ]
Tweneboa-Kodua A, Obeng-Quaidoo I & Abu K 1991. Ghana social mobilization analysis. Health Education & Behavior, 18(1):125-134. https://doi.org/10.1177/109019819101800112 [ Links ]
Vadrucci S, Vigna-Taglianti FD, Van der Kreeft P, Vassara M, Scatigna M, Faggiano, Burkhart G & The EU-Dap Study Group 2016. The theoretical model of the school-based prevention programme Unplugged. Global Health Promotion, 23(4):49-58. https://doi.org/10.1177/1757975915579800 [ Links ]
Walter CM 2014. Promoting physical activity: A low cost intervention programme for disadvantaged schools in Port Elizabeth, South Africa. African Journal for Physical, Health Education, Recreation & Dance, 20(21):357-371. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}