










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Education
versão On-line ISSN 2076-3433
versão impressa ISSN 0256-0100
S. Afr. j. educ. vol.39 no.3 Pretoria Ago. 2019
http://dx.doi.org/10.15700/saje.v39n3a1697
ARTICLES
The prevalence, nature, and functions of non-suicidal self-injury (NSSI) in a South African student sample
Sarojini Naidoo
Discipline of Psychology, School of Applied Human Sciences, University of KwaZulu-Natal, Durban, South Africa. naidoos7@ukzn.ac.za
ABSTRACT
Non-suicidal self-injury (NSSI) has become an increasingly worrying phenomenon among adolescents and young adults. This study sought to address the paucity of data about the prevalence, nature, and functions of NSSI in the South African context. The Inventory of Statements about Self-harm and the Beck Depression Inventory-II were administered to 623 high school and university students recruited for the study. The results indicate an NSSI prevalence rate of 56.2% of the sample, with interfering with wounds, pulling hair, banging heads and cutting being the most common NSSI behaviour. The behaviour appeared to be associated more with intrapersonal functions like affect regulation and self-punishment than with interpersonal functions like communicating distress and maintaining boundaries. The implications of the findings for interventions and future research are discussed.
Keywords: nature; non-suicidal self-injury; prevalence; South Africa; students
Introduction
Youth is the developmental stage at which the first signs of psychological disorders often present. The prevalence of mental health concerns like self-harm and suicidal behaviour have increased dramatically in recent years, with suicide being the leading cause of death among younger individuals in emerging economies such as China (Law & Liu, 2008), India (Pillai, Andrews & Patel, 2009), and South Africa (South African Depression and Anxiety Group [SADAG], 2014). Research has shown that countries undergoing rapid socio-political and economic transition have recorded associations between these changes and self-harm behaviour (Mäkinen, 2000; Rancans, Salander Renberg & Jacobsson, 2001). In these contexts, self-harm is often associated with psychological strain in the form of economic deprivation and unrealised aspirations (Zhang, Wieczorek, Conwell & Tu, 2011), and violence and feelings of hopelessness (SADAG, 2014; Shilubane, Ruiter, Van den Borne, Sewpaul, James & Reddy, 2013).
Although not a new phenomenon, non-suicidal self-injury (NSSI) has recently become the focus of increased clinical and research attention. Previously considered to be a symptom of other psychiatric diagnoses, including borderline personality disorder (BPD), anxiety, and depression (Klonsky & Glenn 2009; Nock, Joiner, Gordon, Lloyd-Richardson, Mitchell & Prinstein, 2006; Whitlock & Knox, 2007), NSSI is now regarded as distinct enough in nomenclature and amenability to classification to warrant a separate diagnosis. It has therefore been included in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) of the American Psychiatric Association ([APA], 2013) as a condition that requires further investigation into a standalone diagnosis in future editions of the DSM. The importance of this possible inclusion lies not only in the potential for NSSI to be studied as a phenomenon, but for the mechanisms underlying this behaviour to be more fully explored. Although an abundance of literature on the nature and prevalence of NSSI behaviour in other countries exists, little data is available for the South African context. The present study sought to explore the prevalence, nature, and functions of NSSI in a sample of South African high school and first-year university students.i
Literature Review
Nock (2009) defines NSSI as direct, self-inflicted damage to one's body (excluding socially sanctioned behaviours such as body piercing) without the intention to die. It includes cutting or carving with a razor or knife, burning, pinching, and scratching of body parts, and banging one's head (Klonsky & Glenn, 2009). The behaviour appears to be equally prevalent across socio-economic statuses and ethnicities (Nock, 2009). The self-injury in NSSI is usually of low lethality, although studies have shown that it often becomes serious enough to warrant clinical intervention (e.g., Makowska, Kropiwinicki & Gmitrowicz, 2016).
Empirical studies suggest that the behaviour is common among young people, with studies reporting prevalence rates of between 9 and 46% in community samples (Lippi, 2014; Lloyd-Richardson, Perrine, Dierker & Kelley, 2007; Ross & Heath, 2002; Whitlock, Eckenrode & Silverman, 2006; Zetterqvist, 2015; Zetterqvist, Lundh, Dahlström & Svedin, 2013). It is unclear whether these widely differing prevalence rates reflect an accurate variation in rates of NSSI, as research findings have been affected by definition and measurement issues (Lloyd-Richardson et al., 2007; Zetterqvist, 2015). Multiple terms have been used to describe NSSI, including deliberate self-harm, parasuicide, self-injurious behaviour, and self-mutilation (Hoff & Muehlenkamp, 2009). As some of these terms are associated with both NSSI and injury with suicidal intent (Mangnall & Yurkovich, 2008), this affects the confidence with which study findings can be meaningfully interpreted.
NSSI typically begins around 14 years of age and reaches a peak at 20 to 29 years of age before declining (APA, 2013). Studies on gender differences in prevalence rates have produced inconsistent findings with some reporting higher rates among females (Yates, Tracy & Luthar, 2008; Zetterqvist et al., 2013) and others indicating no gender effect (Gratz, 2001; Lippi, 2014). International studies have produced inconsistent findings in NSSI rates regarding race differences (Andover, Primack, Gibb & Pepper, 2010; Gratz, 2001; Muehlenkamp & Gutierrez, 2007), while research in South Africa (Joe, Stein, Seedat, Herman & Williams, 2008; Lippi, 2014) indicates that Asian and Coloured individuals are more likely to engage in self-harm than their Black and White counterparts.
The APA (2013) states that NSSI serves to (a) obtain emotional relief from an affective or cognitive state, (b) resolve an interpersonal difficulty, and c) induce a positive feeling state. It appears that NSSI also serves to relieve anxiety, to provide distraction from painful emotions, to punish the self, to reduce dissociative symptoms, to block painful memories, and to communicate and/or relieve intrapersonal and interpersonal distress (Bheamadu, Fritz & Pillay, 2012; Briere & Gil, 1998).
Theoretical Framework
Nock and Prinstein (2004) suggest a four-factor model that elucidates the functions that NSSI behaviour serves. The functions are divided into two dichotomous dimensions: contingencies that are automatic versus social, and reinforcement that is negative or positive. Automatic-negative reinforcement refers to an individual's use of self-harm to achieve a reduction in other negative affective states (e.g., "to stop bad or negative feelings"). Individuals who engage in automatic-positive reinforcement seek to create a positive physiological or psychological state (e.g., "I feel dead inside", "I just want to feel something"). Automatic reinforcement, both positive and negative, appears to be commonly cited in NSSI literature (APA, 2013, Bheamadu et al., 2012). Social positive reinforcement functions refer to the use of NSSI to regulate or influence one's social and interpersonal environment (e.g., "to get a reaction out of others", "to make them take me seriously"), while social negative reinforcement refers to an individual's use of NSSI to avoid negative social or interpersonal situations (e.g., "to avoid punishment from others", "to avoid doing something unpleasant"). Klonsky and Glenn (2009) posit that the automatic and social functions respectively map directly onto their theorised intrapersonal and interpersonal constructs. This study employs Nock and Prinstein's (2004) framework for understanding the mechanisms of NSSI behaviour in our context. Using a cross-sectional survey design, the study sought to explore the prevalence, nature, and functions of NSSI among high school and university students.
Methodology
Sampling
Using a convenience sampling method, students from 10 schools in the Durban metropolitan area and from a first-year psychology class at the University of KwaZulu-Natal were invited to participate in the research. Of the 10 schools, six elected to participate on condition that their anonymity was maintained in the dissemination of findings. In both university and school settings, students who volunteered their participation were recruited into the study.
Participants
Six hundred and twenty-three participants aged 13 to 24 years (M = 17.81, SD = 2.42) were recruited into the study. The sample included 460 females and 163 males, with participants' level of education ranging from Grade 8 to first-year university studies. Four hundred and twenty-seven (68.5%) participants self-reported being Black, 137 (22%) Indian, 26 (4.2%) White, and 33 (5.3%) of mixed race.
Instruments
Inventory of statements about self-harm
The Inventory of Statements about Self-Harm (ISAS), developed by Klonsky and Glenn (2009), measures the prevalence, nature, and functions of self-harm behaviour. The ISAS consists of two sections, the first of which requires participants to endorse NSSI behaviours they have engaged in, and the number of times they have engaged in that behaviour during their lifetime. Items include cutting, scratching, biting, carving, interfering with wounds, pinching, swallowing dangerous substances, burning, and pulling hair. An additional five questions assess descriptive and contextual factors like age of onset, the experience of pain during NSSI, and whether NSSI is performed alone or around others. Participants who endorse one or more NSSI behaviours are requested to complete the second section of the ISAS, which assesses 13 potential functions of NSSI in a Likert-based format. These 13 functions are then summed to produce an Interpersonal function (including autonomy, interpersonal boundaries, interpersonal influence, peer-bonding, revenge, self-care, sensation-seeking, and toughness) and an Intrapersonal function (including affect regulation, anti-dissociation, anti-suicide, marking distress, and self-punishment).
In validation studies using community samples of youth, the ISAS has been found to have high levels of internal consistency for both the Interpersonal and the Intrapersonal functions (Klonsky & Glenn, 2009) and good test-retest reliability over a one-year period (Glenn & Klonsky, 2011). In the present study, Cronbach alpha values of α = .92 were recorded for the Interpersonal scale and α = .91 for the Intrapersonal scale.
Beck Depression Inventory-II
The Beck Depression Inventory-II (BDI-II), developed by Beck, Steer and Brown (1996), is an extensively used 21-item instrument designed for the measurement of depressive symptomatology. Scores range from 0 to 3 for each item, with higher scores indicating more severe depressive symptoms. The scale was used as a measure of concurrent validity in the present study. Validation studies using community samples have indicated good internal consistency of the instrument (Segal, Coolidge, Cahill & O'Riley, 2008; Whisman, Perez & Ramel, 2000). In the present study, a Cronbach alpha value of α = .92 was recorded for the BDI.
Procedure
Assistance with the research was sought from school principals and the registrar of the university with which participants were affiliated. For the school sample, parental consent was sought for those students who indicated that they wished to participate in the research. University students (all over the age of 18 years) were invited to participate at the end of psychology tutorials. Upon written consent being provided by university participants, and assent by school participants, the research questionnaire was administered by postgraduate psychology students. All questionnaires were completed in a single sitting in groups of 20 to 30 students.
Ethical Considerations
Ethical clearance for the research was obtained from the Biomedical Research Ethics Committee at the University of KwaZulu-Natal, Durban (BE138/14). To deal with the possibility that participation in the research might induce distress, participants were advised that debriefing would be provided by school counsellors or the author (a registered psychologist) if they required same. None of the participants availed themselves of this offer.
Data Analyses
The data was analysed using the Statistical Package for the Social Sciences (SPSS) (version 25). In addition to descriptive statistics, frequency and chi square analyses were used to explore the prevalence and nature of NSSI and BDI levels in the sample. An independent samples t-test was used to explore gender differences in scores on the BDI while a paired sample t-test was used to compare endorsement of NSSI functions. To compare race, age, and gender differences on intrapersonal and interpersonal functions, two three-way analyses of variance (ANOVAS) were performed. Finally, a bivariate correlation analysis was used to explore the relationship between NSSI functions and BDI scores.
Results
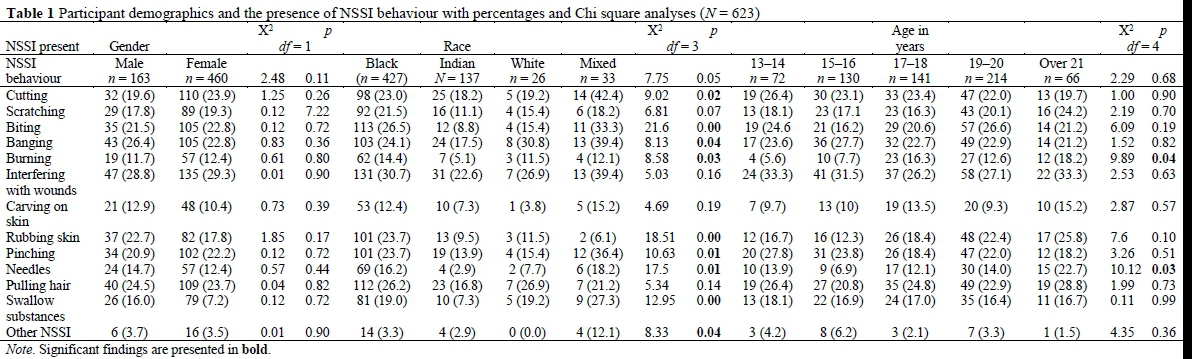
Frequency analyses indicated that, of the total sample (N = 623), 350 participants (56.2%) had engaged in some form of NSSI behaviour (range = 0-6218, M = 107.97, SD = 412.22). Chi square analyses indicated no significant race, age, or gender associations in the overall endorsement of NSSI behaviour; however, there were significant race and age differences in individual NSSI behaviours.
As can be seen in Table 1, interfering with wounds, pulling hair, head banging, and cutting were the most commonly endorsed NSSI acts in the sample. In terms of gender, interfering with wounds was the most commonly endorsed behaviour for both males and females (28.8% and 29.3% respectively), followed by banging or hitting self for males (26.4%), and cutting for females (23.9%). With respect to race, the mixed‑race group showed significantly higher endorsements of several NSSI behaviours with cutting, burning and swallowing dangerous substances being among these. Of those who endorsed NSSI behaviour, 279 participants (79.7%) had engaged in at least two forms of self-injury.
Of those who provided the age at which they initially self-harmed (n = 327), the majority (61.9%) reported being 13 years and under at the time of first harm, while 30.9% were between the ages of 14 and 16 years (M = 12.8 years, SD = 2.70).
One hundred and twenty-nine participants (36.9%) reported experiencing pain during the act, while 120 (34.3%) reported no pain, and 101 (28.9%) sometimes experienced pain. Of the 337 participants who answered the question "are you alone when you self-harm?," 217 (64.4%) indicated that they were, while 83 (24.6%) indicated that they were sometimes alone, and 37 (11.0%) indicated that they were not alone at the time. Of those who indicated the amount of time that elapses between experiencing the urge to self-harm and engaging in the behaviour (n = 321), 51.4% indicated that < 1 hour elapsed, followed by 1 to 3 hours (20.2%), 3 to 6 hours (5.3%), 12 to 24 hours (1.9%) and > one day (18.7%). Of those who answered the item "do you want to stop?" (n = 314), the majority (62; 83.4%) indicated that they would like to stop while 52 participants (16.6%) indicated that they had no wish to stop hurting themselves. Finally, of those who indicated when last they had self-harmed (n = 302), the majority (56.3%) indicated that they had done so in the last year, with 24.2% indicating that their last engagement in self-harm was in the last month. Thirty percent of participants had last self-harmed more than two years prior to participation in the study.
To compare BDI levels, scores were categorised as: 0 to 19 (normal), 14 to 19 (mild), 20 to 28 (moderate) and 29 to 63 (severe) (Beck et al., 1996). Frequency analyses indicated that 32.4% of the sample reported mild depressive symptoms, while 38.4% reported moderate to severe symptoms. An independent samples t-test indicated that females (M = 17.55, SD = 12.82) had significantly higher mean scores than males (M = 12.92, SD = 11.01), [t(62) = -4.10, p < .001, d = 0.20]. No significant race or age differences in BDI scores were recorded. Chi square analyses (Table 2) indicate significant gender differences; more females endorsed mild, moderate, and severe depressive symptoms compared to males. Significant race differences in BDI levels are indicated: more White participants endorsed mild depressive symptoms than the other race groups, while more Black and mixed-race participants endorsed moderate levels of BDI symptoms. Mixed-race participants also reported a higher rate of severe depressive symptoms compared to the other race groups. Although there were no significant age differences in BDI levels, the 15 to 16 year age group had a higher percentage of participants (46.2%) with moderate to severe BDI scores compared to the other age groups.
Descriptive properties were examined for the ISAS and the BDI. Descriptive statistics for the ISAS functions were: Interpersonal: range = 0-40, M = 7.10, SD = 9.70, skewness (statistic = 1.206, SE = .098, z = 12.30), and kurtosis (statistic = -.204, SE = .195, z = 1.04); comparative statistics for the Intrapersonal scale were: range = 0-28, M = 6.31, SD = 7.68, skewness (statistic = .879, SE = .098), and kurtosis (statistic = .515, SE = .195). The distribution of scores for both subscales differed significantly from what would be expected under the normal curve. Consequently, scores for both subscales were subjected to a square root transformation. Estimates of skewness for the transformed Interpersonal subscale (statistic = .573, SE = .098, z = 2.40) and kurtosis (statistic = ‑1.2085, SE = .195; z = 3.23), and the transformed Intrapersonal subscale (statistic = .338, SE = .098, z = 3.44) and kurtosis (statistic = -1.540, SE = .195, z = -7.29) indicated that the distribution of transformed scores did not differ significantly from what would be expected under the normal curve (Kim, HY 2013). Transformed scores for the ISAS were consequently used in all subsequent analyses.
Descriptive statistics for the BDI were: range = 0-57, M = 16.34, SD = 12.54, skewness (statistic = .745, SE = .098, z = 7.60), and kurtosis (statistic = .135, SE = .195, z = .69). Taken together, these statistics indicate that the BDI total scores differed significantly from what would be expected under the normal curve. Consequently, scores for the BDI were subjected to a square root transformation. Estimates of skewness for the transformed variable (statistic = -.400, SE = .098, z = -.408) and kurtosis (statistic = -.410, SE = .195; z = -2.10) indicate that the distribution of transformed scores do not differ significantly from what would be expected under the normal curve (Kim, HY 2013). Transformed scores for the BDI were consequently used in all further analyses.
To compare endorsement of interpersonal and intrapersonal functions of NSSI (prorated by dividing scale scores by the number of subscales, eight for the Interpersonal scale and five for the Intrapersonal scale), a paired sample t-test was used. The results indicate that intrapersonal functions (prorated M = 1.42, SD = 1.94) were significantly more endorsed than interpersonal functions (prorated M = 0.88, SD = 1.21), [t(.622) = -18.26, p < .001, d = 0.73].
To compare race, age, and gender differences on intrapersonal and interpersonal functions, two three-way ANOVAS were performed on the functions (multi-collinearity of the scales did not permit a MANOVA). Given the large sample size, a more stringent significance level of 0.01 was set for these analyses to reduce the possibility of Type II errors, (Kim, J 2015). The ANOVA for interpersonal functions indicated that there was no significant interaction effect of race, age, and gender on interpersonal functions, F (8,587) = .55, p = 0.82. There was a significant main effect for race, F (3,587) = 4.71, p < 0.01; however, the effect size was small (partial eta squared = 0.02). Post hoc comparisons using the Tukey test indicated that transformed mean Interpersonal scores for Blacks (M = 1.92, SD = 2.07) were significantly higher than those for Indians (M = 1.30, SD = 1.77). The main effects for age F (4,587) = 3.25, p = 0.02 and gender F (1,587) = 1.79, p = 0.18 did not reach statistical significance.
The three-way ANOVA for intrapersonal functions indicated that there was no significant interaction effect of race, age, and gender on intrapersonal functions, F (8,587) = .71, p = 0.68. There was a significant main effect of age, F (4,587) = 3.71, p < 0.01; however, the effect size was small (partial eta squared = 0.03). Post hoc comparisons using the Tukey test indicated that transformed mean Intrapersonal scores for the 15 to 16 year age group (M = 2.20, SD = 1.20) were significantly higher than those of the 17 to 18 year age group (M = 1.60, SD = 1.80) and the 19 to 20 year age group (M = 1.53, SD = 1.75). The main effects for race F (3,587) = 3.27, p = 0.02 and gender F (1,587) = .05, p = 0.82 did not reach statistical significance.
Finally, the relationship between ISAS functions and BDI scores was examined using Pearson product-moment correlation coefficient. There was a strong positive correlation between the Intrapersonal and Interpersonal scales, r = .86, p < 0.001; a moderate correlation between the Intrapersonal scale and BDI scores, r = .40, p < 0.001 and a weak correlation between the Interpersonal scale and BDI scores, r = .28, p < 0.001.
Discussion
The findings suggest that the high prevalence rate of NSSI behaviour in this sample is similar to that of clinical samples in inpatient settings in Western settings (Darche, 1990; DiClemente, Ponton & Hartley, 1991). Other South African studies have also recorded higher than average prevalence rates (e.g., Lippi, 2014), indicating that NSSI may be a serious problem in our context. The finding that the majority of the sample reported mild to severe depressive symptoms may help to explain this association. In addition, the fact that nearly 80% of the sample endorsed more than one type of NSSI suggests that the behaviour may be more deliberate than suggested by current perceptions that self-harm may be an innocuous developmental preoccupation. Given the rapid socio-political and economic change that the country has experienced, these high rates may indicate a cohort of young individuals struggling to find a sense of self in an uncertain political and social climate. Zhang et al. (2011) suggest that strain theory (Merton, 1938), which posits that strain results from society pressurising individuals to achieve socially accepted goals, although they don't have access to the resources to do so, may be a useful model to explain self-harm behaviour in such contexts, as opposed to the more popular psychiatric model adopted in the West. Further research is however indicated to further understand this complex interplay of social and political dynamics in the development of NSSI in the South African context.
The finding of no gender association in endorsement of NSSI behaviour is consistent with some studies using community samples (Gratz, 2001; Idemudia, Maepa & Moamogwe, 2016; Lippi, 2014). The literature, however, reports a higher prevalence among females compared to males over the years (Pillay & Pillay, 1987; Ross & Heath, 2002; Whitlock, Muehlenkamp, Eckenrode, Purington, Abrams, Barreira & Kress, 2013). This finding suggests that NSSI in this sample may be related less to biological differences and more to contextual similarities.
Consistent with other research (Bheamadu et al., 2012; Kortge, Meade & Tennant, 2013; Nock & Prinstein, 2004), the period of first onset of NSSI in this sample was during early adolescence; only a small percentage reported first onset in the period approaching young adulthood. The period during which they were most at risk for self-harm was between the ages of 10 and 16 years. There was also an age effect on intrapersonal functions in the present study; 15 to 16 year olds engaged in NSSI to regulate intrapersonal needs significantly more than the 17 to 20 year age group. This may be related to the former age cohort also having a higher percentage of participants with moderate to severe BDI scores compared to the latter group. The most common types of NSSI found in this sample (interfering with wounds, pulling hair, banging or hitting self, and cutting) is consistent with those of other studies (Hamza & Willoughby, 2013; Kortge et al., 2013; Tatnell, Hasking, Newman, Taffe & Martin, 2017).
It would appear that for most participants, their engagement in self-harm behaviour was to meet the intrapersonal needs of affect regulation, marking distress, self-punishment, and regulating suicidal and dissociative feelings, rather than interpersonal needs like communicating distress, maintaining boundaries, bonding with peers, and sensation seeking, as measured by the ISAS. This finding is consistent with those of other studies (Klonsky 2007; Kortge et al., 2013, Nock & Prinstein, 2004). The higher correlation found between the Intrapersonal scale and BDI scores as compared to that between the Interpersonal scale and BDI scores, supports the literature, which indicates that NSSI behaviour is associated with affect regulation (Klonsky & Glenn, 2009; Tatnell et al., 2017). Paradoxically, although NSSI would appear to serve the purpose of regulating suicidal feelings (Klonsky & Glenn, 2009), engagement in self-injury has been shown to be a gateway to later suicidal behaviour (Whitlock et al., 2013). Through repeated self-injury over time, an individual may develop the capability to enact a suicide attempt and once developed, the acquired capability for suicide is not easily amenable to therapeutic modification (Van Orden, Witte, Cukrowicz, Braithwaite, Selby & Joiner, 2010). The literature suggests that the two latent dimensions of acquired capability, lowered fear of death and elevated physical pain tolerance, develop through habituation and opponent processes are likely to remain relatively stable over time (Joiner, 2005; Van Orden et al., 2010). It is evident then that interventions to prevent the development of suicidal feelings in the first instance may break this feedback loop. Joiner (2005) suggests that interventions to reduce perceptions of burdensomeness and thwarted belongingness (theorised to lead to the development of suicidal ideation) and which have been shown to be amenable to therapeutic efforts, are necessary to mitigate this risk.
The finding of a significant race effect on endorsement of interpersonal functions and higher scores on the BDI (Black participants reported higher scores than Indian participants for interpersonal functions and a higher rate of severe depressive scores compared to the other race groups) suggests a cultural element in the association between race, NSSI, and depression. In a country in which opportunities for Blacks remain limited, it is easy to understand how sustained deprivation can lead to depressive states. It is also likely that for these young people, having traditionally been raised within extended family systems, NSSI serves the purpose of communicating their emotional distress in order to activate support systems. The finding suggests that the implementation of multi-sectoral interventions designed to foster known protective factors among Blacks (Flisher, Liang, Laubscher & Lombard, 2004) is required to moderate their engagement in NSSI. South African studies have found that improved social support helped to reduce self-harm behaviour (Idemudia et al., 2016; Pretorius, 2011).
The finding of a significantly higher incidence of some of the more lethal forms of NSSI behaviour (cutting, swallowing dangerous substances) among students of the mixed-race group appears to be a cause for some concern. The finding that this cohort (together with Black participants) also evidenced higher rates of moderate depression intensifies this concern. There was, however, a small number of mixed-race participants in this sample, and future research should more fully explore this finding with a larger, more representative sample of mixed-race students.
The finding that the majority of participants were alone at the time of self-harm and engaged in the act less than an hour after contemplating it, suggests an element of impulsivity that needs to be addressed. Restricting the means to self-harm (knives, dangerous substances) has been shown to reduce this behaviour, and this intervention, particularly for high risk individuals, needs to be given more consideration (Anestis & Bryan, 2013). In addition, better monitoring by family members and significant others may help to mitigate this risk.
An encouraging finding was that the majority of participants reported that they would like to stop harming themselves. This suggests that better social support and psychoeducation may help to reduce the alarming rate of NSSI in this context. Given the early onset of NSSI, schools are in a prime position to teach preadolescents and adolescents life orientation lessons that build self‑esteem, enhance adaptive coping and communication skills, deal with depressive symptoms, and how to access psychological support when needed. School and university psychologists can use dialectical behaviour therapy, which has been shown to reduce both self-harm and depressive symptoms (Mehlum, Tørmoen, Ramberg, Haga, Diep, Laberg, Larsson, Stanley, Miller, Sund & Grøholt, 2014). Although it is acknowledged that routine screening for self-harm behaviour in schools has human resources and financial implications, and has sometimes been shown to yield false positives (Lake & Gould, 2011), it may go a long way towards reducing what appears to be a highly prevalent phenomenon in our context.
The findings of the present study may have been compromised by the inclusion of a university sample that may represent a high-risk group for NSSI. In addition, the use of a single endorsement of NSSI to distinguish injurers from non-injurers may have led to the high prevalence reported in this study. For example, at least one study excluded interfering with wounds (the most prevalent NSSI behaviour in the present study) from analyses and this affected NSSI prevalence rates (Lloyd-Richardson et al., 2007). Future research needs to more fully explore the nuances that characterise definitions of deliberate self-harm. Finally, the use of self-report measures for NSSI and depressive symptoms may have resulted in social desirability issues which may have compromised the findings. Strengths of the study are the relatively large sample size, and this being the first attempt to describe the functions of NSSI in the South African context.
Acknowledgements
The author wishes to acknowledge the assistance of postgraduate psychology students of the University of KwaZulu-Natal in the data collection for this study.
Notes
i. In this study "students" refers to both high school and university participants.
ii. Published under a Creative Commons Attribution Licence.
iii. DATES: Received: 11 May 2018; Revised: 2 October 2018; Accepted: 11 March 2019; Published: 31 August 2019.
References
American Psychiatric Association 2013. Diagnostic and statistical manual of mental disorders: DSM-5 (5th ed). Arlington, VA: Author. https://doi.org/10.1176/appi.books.9780890425596 [ Links ]
Andover MS, Primack JM, Gibb BE & Pepper CM 2010. An examination of non-suicidal self-injury in men: Do men differ from women in basic NSSI characteristics? Archives of Suicide Research, 14(1):79-88. https://doi.org/10.1080/13811110903479086 [ Links ]
Anestis MD & Bryan CJ 2013. Means and capacity for suicidal behavior: A comparison of the ratio of suicide attempts and deaths by suicide in the US military and general population. Journal of Affective Disorders, 148(1):42-47. https://doi.org/10.1016/j.jad.2012.11.045 [ Links ]
Beck AT, Steer RA & Brown GK 1996. Beck depression inventory. San Antonio, TX: The Psychological Corporation. [ Links ]
Bheamadu C, Fritz E & Pillay J 2012. The experiences of self-injury amongst adolescents and young adults within a South African context. Journal of Psychology in Africa, 22(2):263-268. https://doi.org/10.1080/14330237.2012.10820528 [ Links ]
Briere J & Gil E 1998. Self-mutilation in clinical and general population samples: Prevalence, correlates, and functions. American Journal of Orthopsychiatry, 68(4):609-620. https://doi.org/10.1037/h0080369 [ Links ]
Darche MA 1990. Psychological factors differentiating self-mutilating and non-self-mutilating adolescent inpatient females. Psychiatric Hospital, 21(1):31-35. [ Links ]
DiClemente RJ, Ponton LE & Hartley D 1991. Prevalence and correlates of cutting behavior: Risk for HIV transmission. Journal of the American Academy of Child & Adolescent Psychiatry, 30(5):735-739. https://doi.org/10.1016/S0890-8567(10)80007-3 [ Links ]
Flisher AJ, Liang H, Laubscher R & Lombard CF 2004. Suicide trends in South Africa, 1968 - 90. Scandinavian Journal of Public Health, 32(6):411-418. https://doi.org/10.1080%2F14034940410029469 [ Links ]
Glenn CR & Klonsky ED 2011. One-year test-retest reliability of the Inventory of Statements about Self-Injury (ISAS). Assessment, 18(3):375-378. https://doi.org/10.1177/1073191111411669 [ Links ]
Gratz KL 2001. Measurement of deliberate self-harm: Preliminary data on the deliberate self-harm inventory. Journal of Psychopathology and Behavioral Assessment, 23(4):253-263. https://doi.org/10.1023/A:1012779403943 [ Links ]
Hamza CA & Willoughby T 2013. Nonsuicidal self-injury and suicidal behavior: A latent class analysis among young adults. PLoS ONE, 8(3):e59955. https://doi.org/10.1371/journal.pone.0059955 [ Links ]
Hoff ER & Muehlenkamp JJ 2009. Nonsuicidal self‐injury in college students. The role of perfectionism and rumination. Suicide and Life-Threatening Behavior, 39(6):576-587. https://doi.org/10.1521/suli.2009.39.6.576 [ Links ]
Idemudia E, Maepa M & Moamogwe K 2016. Dynamics of gender, age, father involvement and adolescents' self-harm and risk-taking behaviour in South Africa. Gender & Behaviour, 14(1):6846-6859. Available at https://www.researchgate.net/profile/Mokoena_Maepa/publication/331648682_Dynamics_of_Gender_Age_Father_Involvement_and_Adolescents%27_Self-harm_and_Risk-taking_Behaviour_in_South_Africa/links/5c8640e5458515831f9b5227/Dynamics-of-Gender-Age-Father-Involvement-and-Adolescents-Self-harm-and-Risk-taking-Behaviour-in-South-Africa.pdf. Accessed 25 July 2019. [ Links ]
Joe S, Stein DJ, Seedat S, Herman A & Williams DR 2008. Prevalence and correlates of non-fatal suicidal behaviour among South Africans. The British Journal of Psychiatry, 192(4):310-311. https://doi.org/10.1192/bjp.bp.107.037697 [ Links ]
Joiner T 2005. Why people die by suicide? Cambridge, MA: Harvard University Press. [ Links ]
Kim HY 2013. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restorative Dentistry & Endodontics, 38(1):52. https://doi.org/10.5395/rde.2013.38.1.52 [ Links ]
Kim J 2015. How to choose the level of significance: A pedagogical note. Available at https://mpra.ub.uni-muenchen.de/69992/10/MPRA_paper_69992.pdf. Accessed 23 July 2019. [ Links ]
Klonsky ED 2007. The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review, 27(2):226-239. https://doi.org/10.1016/j.cpr.2006.08.002 [ Links ]
Klonsky ED & Glenn CR 2009. Assessing the functions of non-suicidal self-injury: Psychometric properties of the Inventory of Statements About Self-injury (ISAS). Journal of Psychopathology and Behavioral Assessment, 31(3):215-219. https://doi.org/10.1007/s10862-008-9107-z [ Links ]
Kortge R, Meade T & Tennant A 2013. Interpersonal and intrapersonal functions of deliberate self-harm (DSH): A psychometric examination of the Inventory of Statements About Self-Injury (ISAS) scale. Behaviour Change, 30(1):24-35. https://doi.org/10.1017/bec.2013.3 [ Links ]
Lake AM & Gould MS 2011. School-based strategies for youth suicide prevention. In RC O'Connor, S Platt S & J Gordon (eds). International handbook of suicide prevention: Research, policy and practice. Malden, MA: John Wiley & Sons, Ltd. [ Links ]
Law S & Liu P 2008. Suicide in China: Unique demographic patterns and relationship to depressive disorder. Current Psychiatry Reports, 10(1):80-86. https://doi.org/10.1007/s11920-008-0014-5 [ Links ]
Lippi C 2014. An exploratory study of the relationship between deliberate self-harm and symptoms of depression and anxiety among a South African university population. MAClinPsych dissertation. Pretoria, South Africa: University of Pretoria. Available at https://repository.up.ac.za/bitstream/handle/2263/46113/Lippi_Exploratory_2015.pdf?sequence=1&isAllowed=y. Accessed 31 July 2019. [ Links ]
Lloyd-Richardson EE, Perrine N, Dierker L & Kelley ML 2007. Characteristics and functions of non-suicidal self-injury in a community sample of adolescents. Psychological Medicine, 37(8):1183-1192. https://doi.org/10.1017/S003329170700027X [ Links ]
Mäkinen IH 2000. Eastern European transition and suicide mortality. Social Science & Medicine, 51(9):1405-1420. https://doi.org/10.1016/S0277-9536(00)00105-2 [ Links ]
Makowska I, Kropiwinicki P & Gmitrowicz A 2016. Social and family risk factors of self-injury in Polish population of psychiatrically hospitalized adolescents. European Psychiatry, 33:S140. https://doi.org/10.1016/j.eurpsy.2016.01.190 [ Links ]
Mangnall J & Yurkovich E 2008. A literature review of deliberate self‐harm. Perspectives in Psychiatric Care, 44(3):175-184. https://doi.org/10.1111/j.1744-6163.2008.00172.x [ Links ]
Mehlum L, Tørmoen AJ, Ramberg M, Haga E, Diep LM, Laberg S, Larsson BS, Stanley BH, Miller AL, Sund AM & Grøholt B 2014. Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior: A randomized trial. Journal of the American Academy of Child & Adolescent Psychiatry, 53(10):1082-1091. https://doi.org/10.1016/j.jaac.2014.07.003 [ Links ]
Merton RK 1938. Social structure and anomie. American Sociological Review, 3(5):672-682. Available at https://www.jstor.org/stable/pdf/2084686.pdf?casa_token=LSRndTzVbx4AAAAA:Dv3OCAKPrc4OWU19abJ3hrec8DVNufSMtCNZoXpcyqsTQnZCzPJotn9yzp9llzlLjLcpHq7KmWOI8vaeuubeiUa6XHuGOkqd0Lv2wLs_cT-BRRhOfNs. Accessed 16 August 2019. [ Links ]
Muehlenkamp JJ & Gutierrez PM 2007. Risk for suicide attempts among adolescents who engage in non-suicidal self-injury. Archives of Suicide Research, 11(1):69-82. https://doi.org/10.1080/13811110600992902 [ Links ]
Nock MK 2009. Why do people hurt themselves? New insights into the nature and functions of self-injury. Current Directions in Psychological Science, 18(2):78-83. https://doi.org/10.1111%2Fj.1467-8721.2009.01613.x [ Links ]
Nock MK, Joiner TE Jr, Gordon KH, Lloyd-Richardson E & Prinstein MJ 2006. Non-suicidal self-injury among adolescents: Diagnostic correlates and relation to suicide attempts. Psychiatry Research, 144(1):65-72. https://doi.org/10.1016/j.psychres.2006.05.010 [ Links ]
Nock MK & Prinstein MJ 2004. A functional approach to the assessment of self-mutilative behavior. Journal of Consulting and Clinical Psychology, 72(5):885-890. https://doi.org/10.1037/0022-006X.72.5.885 [ Links ]
Pillai A, Andrews T & Patel V 2009. Violence, psychological distress and the risk of suicidal behaviour in young people in India. International Journal of Epidemiology, 38(2):459-469. https://doi.org/10.1093/ije/dyn166 [ Links ]
Pillay AL & Pillay YG 1987. A study of deliberate self-harm at a Pietermaritzburg general hospital. South African Medical Journal, 72(4):258-259. [ Links ]
Pretorius S 2011. Deliberate self-harm among adolescents in South African children's homes. MA thesis. Pretoria, South Africa: University of Pretoria. Available at https://repository.up.ac.za/bitstream/handle/2263/26696/dissertation.pdf?sequence=1. Accessed 2 August 2019. [ Links ]
Rancans E, Salander Renberg E & Jacobsson L 2001. Major demographic, social and economic factors associated to suicide rates in Latvia 1980-98. Acta Psychiatrica Scandinavica, 103(4):275-281. https://doi.org/10.1034/j.1600-0447.2001.00007.x [ Links ]
Ross S & Heath N 2002. A study of the frequency of self-mutilation in a community sample of adolescents. Journal of Youth and Adolescence, 31(1):67-77. https://doi.org/10.1023/A:1014089117419 [ Links ]
Segal DL, Coolidge FL, Cahill BS & O'Riley AA 2008. Psychometric properties of the Beck Depression Inventory II (BDI-II) among community-dwelling older adults. Behavior Modification, 32(1):3-20. https://doi.org/10.1177/0145445507303833 [ Links ]
Shilubane HN, Ruiter RAC, Van den Borne B, Sewpaul R, James S & Reddy PS 2013. Suicide and related health risk behaviours among school learners in South Africa: Results from the 2002 and 2008 national youth risk behaviour surveys. BMC Public Health, 13:926. https://doi.org/10.1186/1471-2458-13-926 [ Links ]
South African Depression and Anxiety Group 2014. Suicide takes its toll. Available at http://www.sadag.org/index.php?option=com_content&view=article&id=2246:suicide-takes-its-toll&catid=92&Itemid=154. Accessed 11 July 2019. [ Links ]
Tatnell R, Hasking P, Newman L, Taffe J & Martin G 2017. Attachment, emotion regulation, childhood abuse and assault: Examining predictors of NSSI among adolescents. Archives of Suicide Research, 21(4):610-620. https://doi.org/10.1080/13811118.2016.1246267 [ Links ]
Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA & Joiner TE Jr 2010. The interpersonal theory of suicide. Psychological Review, 117(2):575-600. https://doi.org/10.1037/a0018697 [ Links ]
Whisman MA, Perez JE & Ramel W 2000. Factor structure of the Beck Depression Inventory-Second Edition (BDI‐ii) in a student sample. Journal of Clinical Psychology, 56(4):545-551. https://doi.org/10.1002/(SICI)1097-4679(200004)56:4%3C545::AID-JCLP7%3E3.0.CO;2-U [ Links ]
Whitlock J, Eckenrode J & Silverman D 2006. Self-injurious behaviors in a college population. Pediatrics, 117(6):1939-1948. https://doi.org/10.1542/peds.2005-2543 [ Links ]
Whitlock J & Knox KL 2007. The relationship between self-injurious behavior and suicide in a young adult population. Archives of Pediatrics & Adolescent Medicine, 161(7):634-640. https://doi.org/10.1001/archpedi.161.7.634 [ Links ]
Whitlock J, Muehlenkamp J, Eckenrode J, Purington A, Abrams GB, Barreira P & Kress V 2013. Nonsuicidal self-injury as a gateway to suicide in young adults. Journal of Adolescent Health, 52(4):486-492. https://doi.org/10.1016/j.jadohealth.2012.09.010 [ Links ]
Yates TM, Tracy AJ & Luthar SS 2008. Nonsuicidal self-injury among "privileged" youths: Longitudinal and cross-sectional approaches to developmental process. Journal of Consulting and Clinical Psychology, 76(1):52-62. https://doi.org/10.1037/0022-006X.76.1.52 [ Links ]
Zetterqvist M 2015. The DSM-5 diagnosis of nonsuicidal self-injury disorder: A review of the empirical literature. Child and Adolescent Psychiatry and Mental Health, 9:31. https://doi.org/10.1186/s13034-015-0062-7 [ Links ]
Zetterqvist M, Lundh LG, Dahlström Ö & Svedin CG 2013. Prevalence and function of non-suicidal self-injury (NSSI) in a community sample of adolescents, using suggested DSM-5 criteria for a potential NSSI disorder. Journal of Abnormal Child Psychology, 41(5):759-773. https://doi.org/10.1007/s10802-013-9712-5 [ Links ]
Zhang J, Wieczorek WF, Conwell Y & Tu XM 2011. Psychological strains and youth suicide in rural China. Social Science & Medicine, 72(12):2003-2010. https://doi.org/10.1016/j.socscimed.2011.03.048 [ Links ]


{kind=link}
{kind=link}