










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Education
versión On-line ISSN 2076-3433
versión impresa ISSN 0256-0100
S. Afr. j. educ. vol.36 no.2 Pretoria may. 2016
http://dx.doi.org/10.15700/saje.v36n2a1285
HIV/AIDS infected mothers' experience of a group intervention to enhance their children's behavior
Irma EloffI; Michelle FinestoneI; Brian ForsythII
IDepartment of Educational Psychology, Faculty of Education, University of Pretoria, South Africa. irma.eloff@up.ac.za
IIDepartment of Pediatrics, Yale University School of Medicine, New Haven, Connecticut, United States of America and Extraordinary Professor of Paediatrics, University of Pretoria, South Africa
ABSTRACT
A secondary study was conducted within a broader National Institutes of Health (NIH)-funded longitudinal study on resilience in South African mothers and children affected by HIV/AIDS (Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome). The aim of this study was to evaluate the effect of a 24-week support group intervention programme, which was designed to enhance adaptive behaviour of latent-phase children affected by maternal HIV/AIDS as reported by the mother participants. The study was embedded in a concurrent nested mixed-method design, with a quasi-experimental and a nested multiple case study approach. The mother and child dyads (n = 139) were purposefully selected from amongst previously identified HIV-positive women (n = 220), with children between the ages of 6 and 10 years at clinics in the Tshwane region, South Africa. Data were collected over a period of five years in multiple waves of intervention implementation. The data collection strategies comprised of mother psychological questionnaires and quality assurance questionnaires. The quantitative data were analysed by means of a paired-sample t-test for within-group comparisons. The qualitative text was analysed for themes to establish defined categories. The findings of the study showed that the mothers reported that the child support group intervention sessions decreased the children's withdrawal-, social-, attention-, rule-breaking- and aggressive behavioural problems. The findings suggest that the use of support groups should be incorporated into intervention programmes dealing with latent-phase children affected by HIV/AIDS to enhance adaptive behaviour.
Keywords: child behavior; group intervention; HIV/AIDS; latency age children
Introduction
Sub-Saharan Africa has 10% of the global population but carries over 69% of the HIV/AIDS burden (Joint United Nations Programme on HIV/AIDS (UNAIDS), 2012). Van der Heijden and Swartz (2010) estimate that 15% of children in South Africa under the age of 15 years of age are directly affected by HIV/AIDS.
Researchers (Cluver & Gardner, 2007; Ebersöhn & Eloff, 2006; Fang, Li, Stanton, Hong, Zhang, Zhao, Zhao, Lin & Lin, 2009) are in agreement that the impact of parental HIV on children is devastating. In South Africa, as in many other developing countries, HIV initiatives initially focused on meeting the basic needs of children living in households affected by HIV. The reason behind this was that the children's immediate material needs were seen as more important than their need for long-term counseling. HIV/AIDS research has, however, shifted focus over the years to include the psychosocial needs of vulnerable children. The psychosocial impact on these children is significant and can include grief, lowered self-esteem and behavior problems.
The middle-childhood years are specifically described by developmentalists (Collins, Madsen & Susman-Stillman, 2002; Wolfe & Mash, 2016) as a dormant phase, where the child experiences relative stability in his/her development before entering the sometimes tumultuous adolescent phase. The middle-childhood years are also referred to as the latent-phase, and span from the ages of 6-10 years. Children in this phase are nonetheless vulnerable to stressors, due to marked changes in competences and distinctive behaviours, which may have long-term implications for adolescent and adult behavioral patterns (Collins et al., 2002; Huston & Ripke, 2006).
Research emphasises the need for rigorously researched theory-based programmes that are culturally appropriate for addressing the psychosocial needs of young children (King, De Silva, Stein & Patel, 2009). In the South African context, research is critical to investigating the protective processes of children who are affected by HIV/AIDS, as the 'disease burden' in South Africa is high. However, the activity of long-term mixed-methods research in this field has been sorely neglected (Betancourt, Meyers-Okhi, Charrow & Hansen, 2013).
The impact of parental illness on a child depends on several factors (Armistead, Klein & Forehand, 1995). Variables pointed out by Spath (2007) are: developmental age, gender of the child and the ill parent, parent/sibling response to illness, and family characteristics. Mother-child relationships generally differ from father-child relationships as the mother typically spends more time with the child. Maternal illness in a singleparent family thus has a remarkable impact on a child's development (Annunziato, Rakotomihamina & Rubacka, 2007; Helseth & Ulfsst, 2003). Factors that play a role in maternal illness are depression, physical incapability of being with a child, and episodes of intense pain (Ferro & Boyle, 2015; Johnston, Martin, Martin & Gumaer, 1992). Research focusing on children in families where the mother is depressed indicates emotional and behavioral difficulties, attachment and academic problems, self-regulation difficulties and problematic peer relationships (Collins et al., 2002; Spath, 2007). These findings indicate that parental illness could be related to psychological distress, and manifested in children's problematic behaviour. Internalising problems include anxiety, rumination, social isolation, depression and low self-esteem, whereas externalising problems include behaviour problems such as bullying and aggressiveness (Van der Heijden & Swartz, 2010).
The presence of parental illness does not per se lead to inescapable psychopathology in children (Korneluk & Lee, 1998). Maternal optimism and positive parenting are protective mechanisms for a child in a single-parent family with a chronic illness (Annunziato et al., 2007). These mechanisms also contribute to a lowering of externalising and internalising behavioural problems. Individual factors, such as age, gender, child and parental coping styles, and protective variables/resilience are further identified as factors that may influence a child's adjustment to parental illness (Korneluk & Lee, 1998). In an attempt to explain why some children affected by HIV develop psychological problems and other children do not, Hough, Brumitt, Templin, Saltz and Mood (2003) refer to factors having a profound effect on children with HIV-infected mothers. The social support structures of the mother, the sociodemographic characteristics of the family, the child's social support structures, the HIV-associated maternal stressors, the mother's coping strategies, the child's coping strategies, and the quality of the mother-child relationship, are all factors ultimately affecting the child's psychosocial adjustment.
King et al. (2009) studied the effectiveness of interventions with the main aim of improving the psychosocial well-being of children affected by HIV/AIDS. They made use of electronic databases and reviewed 1,038 studies. Of these studies, only 11 studies indicated a clearly defined intervention. King et al. (2009:2) came to the conclusion that "no studies of interventions for improving the psychosocial well-being of children affected by HIV and AIDS were identified' and as such recommended "the systematic review has identified the need for high quality intervention studies''. The researchers mention that a reason for this lack of quality studies is that psychosocial intervention for children affected by HIV/AIDS is a relatively new concept.
Researchers continue to aim to demonstrate a need for psychosocial interventions. Psychosocial intervention is a difficult and complex concept, especially in Sub-Saharan Africa, where the impact of HIV/AIDS is immense (King et al., 2009). A people-centred approach is critical in ending the AIDS-epidemic in the post-2015 era (UNAIDS, 2014). The primary aim of this study, therefore, was to investigate the effect of a support group intervention on the internalised and externalised behaviour of children affected by maternal HIV/AIDS as reported by their mothers.
Background
The study reported here is part of a larger NIH funded longitudinal study, also referred to as the Kgolo Mmogo Project. The primary aims of the broad study were to indicate the psychosocial effects of parental HIV disease on young children in South Africa (6-10 year-old children); to assess the effectiveness of a theory-based support intervention for mothers and their children; and to identify maternal, medical and psychological factors and child-related mediating variables that contributed to adaptive functioning of children with HIV-infected mothers (Forsyth, 2005). The conceptual model for the NIH intervention study utilised components of interventions previously used in African communities. The theory-based conceptual model, as designed by Forsyth (2005), regards maternal HIV/AIDS and unsafe social environments as risk factors for negative child behavior outcomes.
The study reported here focuses on the effectiveness of the theory-based support intervention for mothers and their children - specifically as it relates to the adaptive behaviour of the children.
Participants
Sample characteristics. The study sample consisted of 139 children (76 boys, 63 girls) from two districts in the Tshwane region. Although 220 mother-and-child pairs were initially randomly selected to the intervention (treatment) groups, only 161 mother-and-child dyads attended the group sessions. Due to the unequal number of mothers and children returning to the 6-month follow-up interviews, it was necessary to balance the number of responses in each interview group. The mean age of the children was 8.2 years (98.5 months) (SD = 17.9). The mean age of the mothers was 33.3 years (SD = 6.1) and 69.1% mothers had at minimum a Grade 10 educational level. A percentage of 78.4% mothers were unemployed at the start of the intervention sessions. A total of 18.7 % of mothers were married, and 46% of mothers were not married, but had a partner. Only 12.2% mother participants indicated that they (or others) had disclosed to their children that they were infected with the HIV-virus.
Eligibility
The eligibility criteria for the children with HIV-positive mothers were: (1) the child has a mother who is HIV-positive; (2) the child is not infected by HIV him/herself; (3) the child is between the ages of 6-10 years old; (4) the child is cared for by his/her mother for at least 5 days a week; and (5) the child stays in the Tshwane area.
Recruitment
The process of participant selection for the study involved HIV/AIDS volunteer counsellors at selected clinics and hospitals in the Tshwane region. They identified HIV-positive women with children between the ages of 6-10 years. After the objectives of the study were explained to the HIV-positive women, they were asked if their children and they would be interested to partake in study.
Procedure
The HIV-positive women whose children complied with the eligibility criteria, were asked if their telephone numbers could be distributed to the research team. The mothers were assured of confidentiality. The interested mothers were telephoned by the research assistants of the intervention study and they and their children were invited to the nearest site. The research assistants explained the study in detail to the mothers in their home languages. The interested mothers were then asked to complete a consent form. The consent forms were translated into Sepedi, isiZulu, Setswana and Sesotho. The mother could voice her concerns and had the opportunity to ask questions regarding the project. The child was asked to sign an easy-to-understand and culturally friendly assent form, after the mother indicated that she would be willing to participate in the project with her child. The research assistants explained the assent form to the children and gave them the opportunity to indicate whether or not they wanted to take part in the project. Each mother and child pair received a unique study identity number.
The randomisation process of the NIH study was explained to the mothers. A computer probability programme was used to allocate the mother and child pairs to the treatment or no treatment groups. The researchers pre-decided that for each wave of 30 participants, mother/child pairs were selected where 15 pairs received the treatment and 15 pairs did not. Each mother/child pair had an equal opportunity to either receive the treatment or not.
Intervention
A six-month intervention period followed the baseline interviews, where HIV-positive mothers and their children engaged in a structured support group intervention that focused on the enhancement of adaptive behaviour. The intervention was presented in small group format (Forsyth, 2005). In total, 12 groups or waves of mothers and children participated in the intervention support sessions.
There were, on average, eight participants in each wave who attended the support groups.
The intervention programme was developed in collaboration with a team of child development experts from University X and University Y. The intervention was specifically developed to be age appropriate for children 6-10 years old. The children attended the sessions with their mothers on a weekly basis for six months. The mothers and children attended 14 separate sessions and 10 joint sessions. The child group intervention sessions followed a manual that was culturally tailored and focused on coping, problem-solving, emotional intelligence, social skills, and a positive future orientation. The mother sessions focused on coping with their HIV diagnosis, parenting skills, child development and a positive future orientation. The skills learnt in both the mother and child sessions were practiced in the joint sessions. The study had initially intended for care workers from the community to facilitate the group process in order for the intervention to be sustainable in the community. The manual was developed to take this level of accessibility into account. Care workers who facilitated the intervention groups received intensive training and weekly supervision from a psychologist and social worker. The care workers were proficient in all the languages the children spoke, namely Sepedi, Setswana, Isizulu and Sesotho. The manual is an open access resource and available at: http://tinyurl.com/KgoloMmogo InterventionManual (Finestone, 2014).
Interviewer training
Data collection was executed by a team of experienced research assistants, who received additional training in general interviewing methods, specialised child interviewing methods and ethical conduct.
Measures
Kgolo Mmogo sociodemographic questionnaire
Sociodemographic information (e.g., age of child, age of mother, education, marriage status of mother, disclosure to child) was obtained from the mother.
Child Behavior Check List (CBCL)
The CBCL is a widely used and standardised 90-item (items selected according to international recommendations) checklist for school-aged children (school-age version 6-18 years). The measure has an internationally acceptable test-retest reliability (above r > .80). The norming sample for the school-age CBCL was collected in 40 US states and the District of Columbia, with a sample of 1,753 children between the ages of 6-18 years (Achenbach & Rescorla, 2001). It has internal consistency (broad domains alpha > .70) and is valid in detecting clinical significant behavioural and emotional problems in children. The checklist is designed to be user-friendly and to be utilised in assessing children in diverse settings. The mother reports behavioral and/or emotional problems of the child on this checklist. A three point scale is anchored by "0 = not true" and "2 = very true". The items are summed to yield eight syndrome scores and two broadband category scores (Achenbach, 1991). The total internalising t-score (anxious/ depressed and withdrawn behaviour) and Externalising t-score (somatic complaints, social problems, attention problems, rule-breaking behavior aggressive behaviour) were the only scores used in the paired-samples t-test analysis for this investigation. The rationale for this decision was to focus the analysis on broad behavioural categories (e.g. internal and external), rather than fine-grained behavioral patterns.
Mother quality assurance questionnaire
The mothers completed an evaluation form, compiled by the research team, regarding their experience of the support sessions. Two questions were extracted from the mother evaluation feedback form relating to the groups their children attended. The questions were, "what effect has your involvement in Kgolo Mmogo had on your ability to be a parent and why"; and "what effect has your involvement in Kgolo Mmogo had on your child's behavior and why?" The evaluation form was translated and the research assistants asked the questions to the mothers during their 6-month follow-up interviews.
Analysis Strategy
This study included both quantitative and qualitative data collection. The data were collected at two points, at baseline and at 6-months. Both quantitative and qualitative data of the 12 groups were collected in the study to address the possibility that other variables, which were not measured in a single-group pre-post-test design, may have an effect on the children's behaviour (Mark & Reichardt, 2009). For this study, a concurrent nested mixed-method design was chosen and the quantitative and qualitative data were analysed separately, before comparing the two sets of data. The data were extracted from the population using qualitative and quantitative measures and were analysed separately before being theoretically integrated.
The rationale for combining the quantitative and qualitative data in study was to better understand the efficaciousness of a group-based resilience intervention programme for HIV-affected young children by triangulating both broad numeric tendencies from quantitative research and the detail of qualitative research (Creswell, 2003). The quasi-experimental comparison base was established through the inclusion of pre- and post-treatment observations of the treatment group and is referred to as a one-group pretest-posttest design as described by Fouché and De Vos (2001). A baseline interview preceded the introduction of the independent variable (treatment) and a post-test followed at the six-month scheduled interviews. The statistical analysis of the quantitative results was conducted using SPSS (Version 20) (International Business Machines Corporation (IBM), 2011).
In the qualitative phase, the text obtained through the interviews was coded and analysed for themes. A basic coding style was used for analysis to identify emerging themes. The themes of the emergent concepts were then re-coded to establish improved defined categories. The collection of data continued until saturation was reached and the research questions could be answered.
Results
Child Behavior Checklist (CBCL)
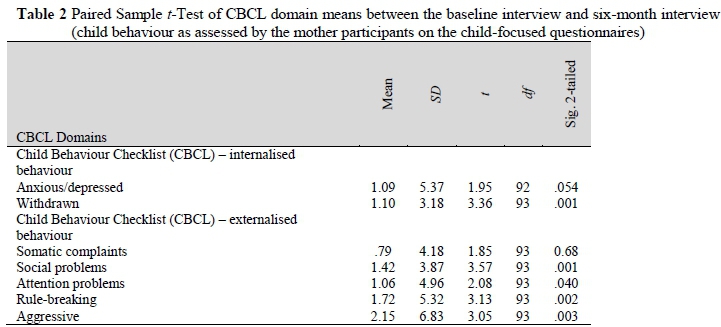
Table 1 outlines the means and standard deviations of the pre-treatment and post-treatment internalised and externalised behavioural problems, as reported by the mother participants on the CBCL. Table 2 outlines the paired sample t-test of CBCL domain means between the baseline interview and six-month interview of the child-focused questionnaires, as reported by the mother participants.
The average scale sores of the reported withdrawn behavioural problems of children on the CBCL before and after treatment, showed a 1.10 point decrease as well as a decrease in the standard deviation. An analysis of the comparison of the mean using a two-tailed, paired t-test (a = 0.05) level revealed a significant difference in the withdrawn behavioural problems reported by the mothers, t (93) = 3.36, p = 0.001. There was furthermore a 1.42 point decrease in the reported social problems, and a decrease in the standard deviation. An analysis revealed a significant difference in the social problems reported by the mothers, t (93) = 3.57, p = 0.001. A significant decrease in the attention behavioural problems were reported by the mothers with a 1.06 point decrease, t (94) = 2.08, p = 0.04. A 1.72 point decrease was indicated in the reported rule-breaking behavioural problems. Likewise, a significant difference in the rule-breaking behavior domain was indicated by the mothers, t (93) = 3.13, p =.002.
The 2.15 point decrease in reported aggressive behavior amounted to a significant difference as reported by the mothers, t (93) = 3.05, p = 003. An analysis of the comparison of the mean using a two-tailed, paired t-test (a = 0.05) level did not reveal significant differences on the anxious/ depressed- and somatic complaints- problem domains as reported by the mothers.
Mother Evaluation Questionnaire
The majority of mothers who completed the evaluation feedback form indicated that they experienced their parenting to be easier after the group support sessions (95%). Only 5% of the mothers indicated that the support sessions made no difference to their parenting. The mothers indicated that the support sessions improved their communication with their children (KM 382 "now I know I have to communicate with my son and ask him some questions I would not have if I didn't came to KM") to such an extent that they were able to discuss their illness with them (KM 202 "I can now explain to my kids about my status'"), as they were emotionally closer to their children after the sessions (KM 460 "My child and I were not very close, but now we are"). The mothers reported enhanced parenting skills (KM 236 "The support I got from KM made me a real parent"), supported them to have more patience with their children (KM 467 "I was tough and impatient to my children, but now I am able to connect with them, give them the love they need and we are close"), to be more supportive of their children (KM 549 "I received support on how to spend time with my kids and support them"), and to use more meaningful discipline practices (KM 438 "I learned to be a better parent and to reprimand them. When I was angry I used to beat them, but since I come to KM I try to control myself").
The majority of the mothers (79%) who completed the mother evaluation form indicated that they experienced their children's behaviour as more positive after the group intervention. A small group of the mothers (21%) indicated that the group had no effect on their child and that their child was either 'always a good child' or 'hasn't changed'. None of the mothers indicated that the child group had a negative effect on their child's behaviour.
The aspects extracted from the mother evaluation questionnaires regarding the effect of the support sessions on the children's behaviour, according to their mothers, are listed as follows:
Mothers indicated that their children's communication skills had improved. They displayed better communication skills with their mothers and with their friends (KM 622 "My son communicates easily with me about his school work. He talks to me about anything, even HIV" and KM 388 "He can now play friendly with other children, even his school performance has increased positively"). The mothers mentioned that the children now listened to them more, as indicated by KM191 ("I have a good relationship with my son now, we spend a lot of time together and he listens when I talk to him. Nowadays he cares much about me and prefers to spend more time with me rather than with his friends"), showed more respect for others (KM 358 "His behaviour has improved a lot and he now shows a lot of respect for me and other people"), had a more trusting relationship with them (KM 545 "He is more easy to communicate with. He received my disclosure to him with understanding") and were more obedient (KM 421 "...because my child can now listen to me when I give him advice"). The mothers reported that their children's selfconfidence had improved (KM 297 "she was shy, but ever since we came to KM she is now open, she told her teacher that we are in the KM project, she told me that she is seeing improvement in my daughter"), as well as their behaviour (KM320 "his behaviour of stealing money and food at home is getting better"). Changes in the children's behaviour, as described by the mothers, were that their children took more responsibility at home (KM 202 "her school performance has improved. My daughter is more responsible, she washes her clothes when I am not at home, she cooks and cleans, she didn't do this before we came to KM") and they were more caring (KM 580 "he is more responsible and more caring. He is no longer rough at play, he is now softer").
Other aspects that emerged in the mother evaluation forms were that their children's schoolwork included improvement (KM 269 "Her concentration at school has improved and now she even listens to me") and their children's behaviour changed, where they rather chose to stay at home rather than to play in the streets (KM 149 "he used to be away from home for the whole day and did not listen when I talked to him, but now he listens and prefers staying at home"). Some mothers reported that their children were less aggressive (KM 414 "she was an angry child before coming to KM. Now she has improved a lot") and less stressed (KM 157 "he has become more open and is now able to talk to me about anything. He does not seem to stress a lot about his brother's behaviour of abusing substances like before"). Some mothers evaluated their children's social behaviour as more appropriate (KM 701 "my child no longer fights with other kids as he used to do before he started attending KM support groups") and they described their children's behaviour as more emphatic (KM 411 "he is more understanding and cares about other's feelings"). The impact of the support sessions was seen in the children's behaviour at home and at school.
Discussion
The mother support group sessions purposely focused on coping with HIV and parenting. The mothers in the support group intervention related their child's improved behaviour to their own improved parenting skills. They mentioned that they experienced their parenting role becoming easier as their communication skills improved, their discipline practices becoming more meaningful and in their improved understanding of their children' s development they became more tolerant of their children's behaviour. The group sessions brought them emotionally closer to their children, made them more supportive of their children and a more trusting relationship developed between them. Armstrong, Birnie-Lefcovitch and Ungar (2005) point to the important relationship between the quality of parenting and a child's ability to cope during adversity. Good parenting has the effect that many risk factors in a child's life can be mediated, taking into consideration the child's characteristics and behaviour. Building a trusting relationship is an important aspect of being resilient (Williams, Lindsey, Kurtz & Jarvis, 2001). In Condly's (2006) review of the literature, a child with a positive feeling towards his/her parent, where the parent is part of the child's daily life, reacts better to trauma.
The mothers reported that they experienced the child support group intervention sessions as positive. This finding confirms the positive effect on adaptive behaviour in children, which is evident from the CBCL results. A latent phase child's development is influenced notably by the groups surrounding them. The group context provides children with modeling opportunities to imitate positive behaviour and observe the problemsolving behaviour of their peers (Akos, 2000). The children's intervention sessions specifically focused on emotional intelligence, problem-solving skills, coping skills and social skills. Hughes-d'Aeth (2002) places emphasis on the inclusion of qualitative aspects in monitoring an intervention. The current study concurs with this perspective. The mothers reported on both the quantitative and qualitative measurements incorporated in this study, noting that their children' s behaviour changed positively. They displayed a decrease in their externalised behavioural problems in specific relationship to their social behaviour, attention, rule-breaking behaviour and aggressive behaviour. The mothers described a further decrease in their children's internalised behaviour in regard to withdrawn behaviour. The children subsequently displayed an improvement in their communication skills and self-confidence, according to the mothers. They listened more to their mothers, and showed more respect and responsibility. The mothers reported that this behaviour was not just observed at home, but also reported by the children's teachers. Despite this, the children's anxiety/depression and somatic complaints were not significantly different from their baseline and 6-month interviews, where the children exhibited an overall improvement in their adaptive behaviour.
Risk and resilience are multifaceted, and expressed in different behaviours in different contexts (Rutter, 2013). This study purported to capture these behavioural complexities by means of multiple data collection strategies. Childhood resilience is observed in the competence displayed by the child in the school, social and behavioural arenas, and as such, needs to be analysed by both quantitative and qualitative means. Resilience is not an 'all or nothing' personal characteristic, but rather a situation and a context within which a child can deal with certain kinds of adversity, whilst having difficulties in dealing with others. It is implausible that children will show resilience across all adverse situations. Masten and Obradovic (2006) caution researchers to take into account that some risks and adversities are so overwhelming for a child's development that resilience is not possible. This study focused on children in severe adversity, and the findings indicate that resilience can be evident in multiple behavioural domains during and after the implementation of a theory-based group intervention.
Some children exposed to multiple stressors and adversities such as parental illness, poverty and violence, do not only survive, but thrive (Condly, 2006; Liebenberg & Ungar, 2009). The main objective of an intervention is to enhance resilience opportunities and adaptive behaviour and to lessen possible risks (Gilgun & Abrams, 2005). The findings from this study indicate a positive effect on a number of behavioural domains in the latent phase children participating in this study. The joint support group intervention sessions in this study gave an opportunity to the mothers and children to practice their skills and to apply the knowledge they learnt in the intervention sessions in a fun way. The group sessions provided the necessary opportunities for both the mothers and children to develop effective relationships. This interaction allowed the mothers to better know their children and to make more accurate observations of their behaviour. The supportive role of the mothers facilitated therefore opportunities for the children to display adaptive behaviour.
There is an intervention need for mothers and their school-aged children, other than medicine adherence and prevention interventions. An intervention programme can provide a child with strong adult and peer attachments, which are reported in resilience research to be an indicative protective factor. Support groups for parents, group sessions for children and group activities are the most powerful interventions in a non-medical context (Kmita, Baranska & Niemiec, 2002; Murphy & Marelich, 2008; Murphy, Marelich, Armistead, Herbeck & Payne, 2010). In addition, from this study it seems that support groups for parents seem to have a positive impact on a child's psychosocial development. The support group intervention for both the mothers and children in this study addressed communication, coping and problem-solving skills that were beneficial to children displaying non-adaptive behaviour, as they were taught how to communicate, how to solve problems and other life skills.
Limitations of the Study
There are several limitations to the study. The study reported here only focuses on the results of the treatment group. Findings from the broader study have been disseminated elsewhere (Boeving Allen, Finestone, Eloff, Sipsma, Makin, Triplett, Ebersöhn, Sikkema, Briggs-Gowan, Visser, Ferreira & Forsyth, 2014; Sipsma, Eloff, Makin, Finestone, Ebersöhn, Visser, Sikkema, Boeving Allen, Ferreira & Forsyth, 2013). The authors also acknowledge the psychological phenomenon that behavioural improvement can often occur during psychological intervention by mere virtue of the fact that challenges are being addressed within a structured format and receiving the attention of professional healthcare service providers. Nevertheless, the statistically significant findings reported in this study do point to some pertinent, domain-specific behavioural improvement in latency age children. Furthermore, the study leaned heavily on data generated by the mother participants. This was due to significant language barriers within this young vulnerable population. Within the broader study, additional analysis was done on data collection with child participants and it has also been reported elsewhere (Ebersöhn, Eloff, Fine-stone, Van Dullemen, Sikkema & Forsyth, 2012). Finally, intervention research with vulnerable populations often creates ethical challenges for researchers - especially when retrospectively there has been positive effects. During the study, a team of care workers, two social workers and a registered psychologist ensured that the non-treatment group in this study received optimal support and appropriate references to relevant healthcare services available in the context in which the study was conducted. During the pilot phase of the five-year project, challenges in healthcare services were however identified and reported (Eloff, Forsyth, Finestone, Ebersöhn, Visser, Ferreira, Boeving & Sikkema, 2011).
Conclusion
The theory-based group intervention in this study enhanced the children's internal and external behaviour. The group sessions reduced the children's withdrawal-, social-, attention-, rule-breaking- and aggressive behavioural problems. The joint sessions of the intervention seemed to have enhanced communication between the mother and child pairs and the qualitative findings indicate that the group-based intervention programme was efficacious to enhance adaptive behaviour in these vulnerable children.
Acknowledgements
This primary research was supported by a grant from the National Institute of Mental Health (Grant Number: 5R01MH076442).
References
Achenbach TM 1991. Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Burlington, VT: Department of Psychiatry, University of Vermont. [ Links ]
Achenbach TM & Rescorla LA 2001. Manual for the ASEBA school-age forms & profiles: an integrated system of multi-informant assessment. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families. [ Links ]
Akos P 2000. Building emphatic skills in elementary school children through group work. The Journal of Specialists in Group Work, 25(2):214-223. doi: 10.1080/01933920008411462 [ Links ]
Annunziato RA, Rakotomihamina V & Rubacka J 2007. Examining the effects of maternal chronic illness on child well-being in single parent families. Journal of Developmental & Behavioral Pediatrics, 28(5):386-391. doi: 10.1097/DBP.0b013e3181132074 [ Links ]
Armistead L, Klein K & Forehand R 1995. Parental physical illness and child functioning. Clinical Psychology Review, 15(5):409-422. doi: 10.1016/0272-7358(95)00023-I [ Links ]
Armstrong MI, Birnie-Lefcovitch S & Ungar MT 2005. Pathways between social support, family well being, quality of parenting, and child resilience: What we know. Journal of Child and Family Studies, 14(2):269-281. doi: 10.1007/s10826-005-5054-4 [ Links ]
Betancourt TS, Meyers-Okhi SE, Charrow A & Hansen N 2013. Annual research review: Mental health and resilience in HIV/AIDS-affected children - a review of the literature and recommendations for future research. Journal of Child Psychology and Psychiatry, 54(4):423-444. doi: 10.1111/j.1469-7610.2012.02613.x [ Links ]
Boeving Allen A, Finestone M, Eloff I, Sipsma H, Makin J, Triplett K, Ebersöhn L, Sikkema K, Briggs-Gowan M, Visser M, Ferreira R & Forsyth BWC 2014. The role of parenting in affecting the behavior and adaptive functioning of young children of HIV-infected mothers in South Africa. AIDS and Behavior, 18(3):605-616. doi: 10.1007/s10461-013-0544-7 [ Links ]
Cluver L & Gardner F 2007. The mental health of children orphaned by AIDS: a review of international and southern African research. The Journal of Child & Adolescent Mental Health, 19(1):1-17. doi: 10.2989/17280580709486631 [ Links ]
Collins WA, Madsen SD & Susman-Stillman A 2002. Parenting during middle childhood. In MH Bornstein (ed). Handbook of parenting: Children and parenting (Vol. 1, 2nd ed). Mahwah, NJ: Lawrence Erlbaum Associates. Available at https://saidnazulfiqar.files.wordpress.com/2008/04/07-handbook-of-parenting-2nd-vol-1-children-and-parenting.pdf. Accessed 11 May 2016. [ Links ]
Condly SJ 2006. Resilience in children. A review of literature with implications for education. Urban Education, 41(3):211-236. doi: 10.1177/0042085 906287902 [ Links ]
Creswell JW 2003. Research design: Qualitative, quantitative, and mixed methods approaches (2nd ed). Thousand Oaks, CA: Sage Publications. [ Links ]
Ebersöhn L & Eloff I 2006. Identifying asset-based trends in sustainable programmes which support vulnerable children. South African Journal of Education, 26(3):457-472. Available at http://www.sajournalofeducation.co.za/index.php/saje/article/view/86/48. Accessed 12 May 2016. [ Links ]
Ebersöhn L, Eloff I, Finestone M, Van Dullemen I, Sikkema K & Forsyth B 2012. Drawing on resilience: piloting the utility of the Kinetic Family Drawing to measure resilience in children of HIV-positive mothers. South African Journal of Education, 32(4):331-348. Available at http://www.sajournalofeducation.co.za/index.php/saje/article/view/660/310. Accessed 12 May 2016. [ Links ]
Eloff I, Forsyth B, Finestone M, Ebersöhn L, Visser M, Ferreira R, Boeving A & Sikkema K 2011. Intervention groups for HIV-infected women: the need for additional services. South African Journal of Psychology, 41(1):38-51. [ Links ]
Fang X, Li X, Stanton B, Hong Y, Zhang L, Zhao G, Zhao J, Lin X & Lin D 2009. Parental HIV/AIDS and psychosocial adjustment among rural Chinese children. Journal of Pediatric Psychology, 34(10):1053-1062. doi: 10.1093/jpepsy/jsp006 [ Links ]
Ferro MA & Boyle MH 2015. The impact of chronic physical illness, maternal depressive symptoms, family functioning, and self-esteem on symptoms of anxiety and depression in children. Journal of Abnormal Child Psychology, 43(1):177-187. doi: 10.1007/s10802-014-9893-6 [ Links ]
Finestone M (ed.) 2014. Intervention programme for the enhancement of children's resilience. Pretoria, South Africa: Faculty of Education, University of Pretoria. Available at http://tinyurl.com/KgoloMmogoInterventionManual. Accessed 21 April 2016. [ Links ]
Forsyth B 2005. Promoting resilience in young children of HIV-infected mothers in South Africa. Research proposal submitted to the National Institutes of Health, April. [ Links ]
Fouché CB & De Vos AS 2001. Selection of a research design. In AS de Vos (ed). Research at grass roots: A primer for the caring professions. Pretoria, South Africa: Van Schaiks. [ Links ]
Gilgun J & Abrams L 2005. Gendered adaptations, resilience, and the perpetration of violence. In M Ungar (ed). Handbook for working with children and youth: Pathways to resilience across cultures and contexts. Thousand Oaks, CA: Sage Publications. [ Links ]
Helseth S & Ulfsst N 2003. Having a parent with cancer: Coping and quality of life of children during serious illness in the family. Cancer Nursing, 26(5):355-362. [ Links ]
Hough ES, Brumitt G, Templin T, Saltz E & Mood D 2003. A model of mother-child coping and adjustment to HIV. Social Science & Medicine, 56(3):643-655. doi: 10.1016/S0277-9536(02)00061-8 [ Links ]
Hughes-d'Aeth A 2002. Evaluation of HIV/AIDS peer education projects in Zambia. Evaluation and Program Planning, 25(4):397-407. doi: 10.1016/S0149-7189(02)00051-4 [ Links ]
Huston AC & Ripke MN 2006. Middle childhood. Contexts of development. In AC Huston & MN Ripke (eds). Developmental contexts in middle childhood: Bridges to adolescence and adulthood. Cambridge, UK: Cambridge University Press. [ Links ]
International Business Machines Corporation (IBM) Corporation 2011. IBM SPSS Statistics 20 Core System User's Guide. Armonk, NY: IBM Corporation. Available at https://www.csun.edu/sites/default/files/statistics20-core-system-guide-64bit.pdf. Accessed 17 May 2016. [ Links ]
Johnston M, Martin C, Martin M & Gumaer J 1992. Long-term parental illness and children: Perils and promises. The School Counselor, 39(3):225-231. [ Links ]
King E, De Silva M, Stein A & Patel V 2009. Interventions for improving the psychosocial wellbeing of children affected by HIV and AIDS. Cochrane Database of Systematic Reviews, 2: Art. No. CD006733. doi: 10.1002/14651858.CD006733.pub2 [ Links ]
Kmita G, Baranska M & Niemiec T 2002. Psychosocial intervention in the process of empowering families with children living with HIV/AIDS - a descriptive study. AIDS Care: Psychological and Sociomedical Aspects of AIDS/HIV, 14(2):279-284. doi: 10.1080/09540120120076959 [ Links ]
Korneluk YG & Lee CM 1998. Children's adjustment to parental physical illness. Clinical Child and Family Psychology Review, 1(3):179-193. doi: 10.1023/A:1022654831666 [ Links ]
Liebenberg L & Ungar M (eds.) 2009. Researching resilience. Toronto, Canada: University of Toronto Press. [ Links ]
Mark MA & Reichardt CS 2009. Quasi-experimentation. In L Bickman & DJ Rog (eds). The SAGE handbook of applied social research methods (2nd ed). Thousand Oaks, CA: Sage Publications, Inc. [ Links ]
Masten AS & Obradovic J 2006. Competence and resilience in development. Annuals of the New York Academy of Sciences, 1094:13-27. doi: 10.1196/annals.1376.003 [ Links ]
Murphy DA & Marelich WD 2008. Resiliency in young children whose mothers are living with HIV/AIDS. AIDS Care: Psychological and Socio-medical Aspects of AIDS/HIV, 20(3):284-291. doi: 10.1080/09540120701660312 [ Links ]
Murphy DA, Marelich WD, Armistead L, Herbeck DM & Payne DL 2010. Anxiety/stress among mothers living with HIV: effects on parenting skills and child outcomes. AIDS Care: Psychological and Socio-medical Aspects of AIDS/HIV, 22(12):1449-1458. doi: 10.1080/09540121.2010.487085 [ Links ]
Rutter M 2013. Resilience: Causal pathways and social ecology. In M Ungar (ed). The social ecology of resilience. New York, NY: Springer. [ Links ]
Sipsma H, Eloff I, Makin J, Finestone M, Ebersöhn L, Visser MJ, Sikkema KJ, Boeving Allen CA, Ferreira R & Forsyth B 2013. Behavior and psychological functioning of young children of HIV positive mothers in South Africa. AIDS Care: Psychological and Socio-medical Aspects of AIDS/HIV, 25(6):721-725. doi: 10.1080/09540121.2013.779627 [ Links ]
Spath ML 2007. Children facing a family member's acute illness: A review of intervention studies. International Journal of Nursing Studies, 44(5):834-844. doi: 10.1016/j.ijnurstu.2006.05.008 [ Links ]
Joint United Nations Programme on HIV/AIDS (UNAIDS) 2012. Global report: UNAIDS report on the global AIDS epidemic 2012. Geneva, Switzerland: UNAIDS. Available at http://www.unaids.org/sites/default/files/media_asset/20121120_UNAIDS_Global_Report_ 2012_with_annexes_en_1.pdf. Accessed 10 May 2016. [ Links ]
UNAIDS 2014. The gap report. Geneva, Switzerland: UNAIDS. Available at http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/ unaidspublication/2014/UNAIDS_Gap_report_en.pdf. Accessed 10 May 2016. [ Links ]
Van der Heijden I & Swartz S 2010. Bereavement, silence and culture within a peer-led HIV/AIDS-prevention strategy for vulnerable children in South Africa. African Journal of AIDS Research, 9(1):41-50. doi: 10.2989/16085906.2010.484563 [ Links ]
Williams NR, Lindsey EW, Kurtz PD & Jarvis S 2001. From trauma to resiliency: Lessons from former runaway and homeless youth. Journal of Youth Studies, 4(2):233-253. doi: 10.1080/13676260123589 [ Links ]
Wolfe DA & Mash EJ 2016. Abnormal child psychology (6th ed). Belmont, CA: Wadsworth Cengage Learning. [ Links ]


{kind=link}
{kind=link}