










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Education
versión On-line ISSN 2076-3433
versión impresa ISSN 0256-0100
S. Afr. j. educ. vol.35 no.2 Pretoria may. 2015
http://dx.doi.org/10.15700/SAJE.V35N2A988
Attention Deficit Disorder (ADHD): Primary school teachers' knowledge of symptoms, treatment and managing classroom behaviour
Beryl TopkinI; Nicolette Vanessa RomanI; Kelvin MwabaII
IChild and Family Studies, Department of Social Work, Faculty of Community and Health Sciences, University of the Western Cape, South Africa. nicoletteroman@gmail.com
IIDepartment of Psychology, Faculty of Community and Health Sciences, University of the Western Cape, South Africa
ABSTRACT
ADHD is one of the most common chronic conditions of childhood. Teachers are a valuable source of information with regard to referral and diagnosis of the disorder. They also play a major role in creating an environment that is conducive to academic, social and emotional success for children with ADHD. The aim of this study was to examine primary school teachers' knowledge of the symptoms and management of children in their classrooms who were diagnosed with ADHD. The participants were 200 South African primary school teachers (178 female, 22 male; mean age = 43 years) of children enrolled in Grades One to Four. A self-administered questionnaire, the Knowledge of Attention-Deficit Disorder Scale (KADDS), which measures the misperceptions and understanding of the disorder, was used to collect the data. The results indicated that overall, 45% of the teachers correctly identified the responses to the items asked in the questionnaire. The "don't know responses" accounted for 31% of responses, while 22% of the responses were incorrectly identified. Furthermore, teachers were more knowledgeable of the general associated features of ADHD than of symptoms, diagnosis and treatment. A majority of teachers indicated that they had received training. These findings suggest a need to consider improving evidenced-based classroom interventions for ADHD among South African teachers.
Keywords: ADHD; BRICS; child development; classroom management; education; educational interventions; learning disabilities; management of ADHD; primary school teachers
Introduction
South Africa's status as a leading emerging economy in Africa is well established. The country's membership of the BRICS (Brazil, Russia, India, China and South Africa) confirms its role as an important emerging economy on the global stage. However, despite this strong economic standing, South Africa continues to grapple with major economic challenges including high unemployment, poverty, and inequalities in social and economic spheres.
One of the most glaring challenges of inequality wrought by past policies of racial discrimination is in South Africa's education system. Although much progress has been made in improving education, schools in large parts of the country are still faced with inadequate resources and poorly trained teachers.
As part of reforms designed to change the South African education landscape, the new democratic government established guidelines in the Education White Paper 6 (Department of Education, 2001) that state: "all children and youth can learn and need support and that learners' individual strengths need to be encouraged" (Nel, Nel & Hugo, 2013). The main aim of these reforms is to ensure that the country establishes an education system that is inclusive, in order to achieve a society that is based on social justice (Department of Education, 2001). Given the country's past history of racial strife and injustice, the education reforms are key to redressing historical imbalances, and to the promotion of ideals of the new political dispensation. Key to education reforms would be the training of teachers in classroom management. Classroom management becomes paramount, specifically with children who have been diagnosed with ADHD, as part of their treatment regime (Schultz, Storer, Watabe, Sadler & Evans, 2011).
Attention Deficit Disorder (ADHD) is characterised by"a chronic and pervasive pattern of developmentally inappropriate levels of inattentiveness, hyperactivity and impulsivity manifesting in early childhood" (American Psychiatric Association, 2013:103-106), which then may continue into adulthood. Individuals with ADHD often exhibit deficits in one or more areas of executive functioning, including verbal working memory, emotion regulation, behavioural inhibition, motivation, planning, strategy generation and implementation, and self-monitoring (Barkley, 2005; Willcutt, Doyle, Nigg, Faraone & Pennington, 2005). The prevalence rates of ADHD are variable. For example, a systematic review reported a worldwide prevalence rate of ADHD as 5.29% (Polanczyk, De Lima, Horta, Biederman & Rohde, 2007). Cross-cultural studies suggest that ADHD is increasing in developing countries as much as 6% to 10% in Africa (Kashala, Tylleskar, Elgen, Kayembe & Sommerfelt, 2005; Ofovwe, Ofovwe & Meyer, 2006). In South Africa, the prevalence rates were reported retrospectively in a study as 37.9% of 58 adult participants diagnosed with childhood ADHD (Mahomedy, Van der Westhuizen, Van der Linde & Coetsee, 2007) and 8% to 10% by the Attention Deficit and Hyperactivity Support Group of Southern Africa (ADHASA). However, Muthukrishna (2013) states that the prevalence of ADHD is not officially presented in South Africa.
ADHD is normally diagnosed by a psychologist or a medical practitioner (Schellack & Meyer, 2012). The diagnostic criteria in the Diagnostic and Statistical Manual for Mental Disorders, Fifth Edition (DSM-5) characterizes ADHD as:
A persistent pattern of inattention and/or hyper-activity-impulsivity that interferes with functioning or development as characterized by at least six symptoms from either (or both) the inattention group of criteria and the hyperactivity and impul-sivity criteria. These symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social educational and work settings (Sadock, Sadock & Ruiz, 2015:1170).
It is often the teacher who is important in providing the information for diagnosing ADHD (Wolraich, Lambert, Baumgaertel, Garcia-Tornel, Feurer, Bickman & Doffing, 2003).
In a survey investigating the diagnosis of ADHD, two-thirds of the survey respondents indicated that teachers most frequently made the initial referral for a child to be evaluated for ADHD (Malen, 2008). In the course of the diagnosis, the teacher and parent reports are paramount (Snider, Busch & Arrowood, 2003). Often, teachers initiate the referral for an ADHD assessment because the structured school environment means that children with problems of inattention, hyperactivity and im-pulsivity exhibit behaviours with which the other children and their teachers cannot cope.
Once a child is diagnosed with ADHD, available treatment for ADHD are psychostimulant medication, educational interventions, behaviour modification procedures, diet manipulation and supplements. The management of the disorder then becomes important, because the performance effects of the intervention strategies require close monitoring and feedback to all relevant role-players to improve the child's behaviour (DuPaul & Stoner, 2003). Behaviour therapy and classroom behaviour interventions training for parents have been shown to have positive results when it comes to the treatment of ADHD (Anastopoulos & Farley, 2003). This would then mean that the training of teachers to manage the behaviour of the child diagnosed with ADHD ought to be an important first step for classroom management. This training would need to include knowledge of symptoms and treatment of diagnosing ADHD, as well as managing the behaviour of the child in the classroom.
According to the White Paper 6 (Department of Education, 2001) on Inclusive Education, learners who have special needs, such as having a diagnosis of ADHD, should have a differentiated curriculum and evaluation system that might enable them to progress at their own rate and at their own level, while placed in mainstream classes. Mainstream educators, however, lack the understanding, tolerance and knowledge of ADHD learners (Dore, 2010). They therefore pretend not to see behavioural problems, or sometimes to shut the learner out from class lessons (Ramphal, 2010). Perold, Louw and Kleynhans (2010) found that there was substantial lack of knowledge among teachers in certain key areas of ADHD. Furthermore, teachers also indicated that they had very little or no training in ADHD and the management of ADHD in the classroom. Similarly, Hariparsad (2010) found that teachers required more training on teaching children diagnosed with ADHD, as in-service training on the matter had not been provided by the Department of Education. Research in South Africa suggests that teachers, as a means of managing their classrooms, engage learners who may have ADHD in alternative tasks such as sweeping the classroom, taking messages to other teachers or additional academic work in class (Lopes, Eloff, Howie & Maree, 2009). In the context of an inclusive classroom, teachers need to ensure that children with ADHD participate in the curriculum and classroom activities. In an emerging economy like South Africa, where there may be limited public knowledge of ADHD, teachers have a great role to play in recognising ADHD symptoms (Davies, 2010) as well as managing and supporting the learners with ADHD in the classroom. In the present study we were therefore interested to: 1) assess primary school teachers' knowledge of the symptoms and treatment of ADHD; and 2) determine strategies primary school teachers use to manage children in their classrooms diagnosed with ADHD.
Method
A cross-sectional descriptive study design was used in this study.
Participants
Permission to conduct the study was granted by the ethics review board at a university in the Western Cape, the Northern Cape Education Department, and the principals of the relevant schools. Of the 28 primary schools identified in the Kimberley area, 23 schools formed part of the sample as five schools had formed part of the pilot study. Thus the total number of teachers at the 23 schools was 300 teachers. Although all of these teachers were invited to participate in the study, in the end only 200 teachers participated, indicating a response rate of 67 percent.
Scheduled meetings were arranged in order to establish a suitable time and venue permitting accessibility to the Grade One to Five teachers. Upon request by the Department of Education, five out of eight special needs schools were added, and formed part of the sample of 23 schools from previously disadvantaged and advantaged areas. Participants could take part voluntarily. No names were used at any time during the data collection process, and in this way, they were assured that their information would remain anonymous and confidential. Participants were provided the opportunity not to participate, and to withdraw at any time during the research process without consequence. The final sample consisted of 200 participants, of whom 178 (89%) were female, and 22 (11%) were male. The Mean age of the sample was 43 years (SD = 11.01). The majority of the participants identified themselves as Black African (33.8%), married (57.6%), and had over 20 years teaching experience in a primary school.
The schools were divided or categorised according to quintiles, which indicate whether the school is an advantaged or disadvantaged school. A quintile of four or five places the school in the advantaged category, while a quintile of one or two places it in the disadvantaged category, according to the previous apartheid dispensation. The schools with a quintile of one or two will thereby qualify as no-fee paying school, and parents of children from such a school will therefore not be asked to pay school fees. These are also the schools that participate in the feeding scheme of the Department of Education. Table 1 indicates that the majority of participants taught the foundation phase grades, that is, Grades One, Two and Three. However, within the foundation phase, the majority of teachers (22.8%) were teaching Grade One. Just over 50% of the participants indicated that school fees were payable at their schools.

Measuring Instrument
The KADDS measures teachers' understanding and perceptions of ADHD (Sciutto, Terjesen & Frank, 2000). The scale consists of 36 items. The responses were indicated as 'incorrect', 'correct' and 'don't know' responses. Correct responses were indicated with a '1', while incorrect and don't know responses were indicated with a '0'. The Alpha coefficient for the current study was .89 for the total items. This alpha score indicates good reliability of the instrument and similar results were found locally (Perold et al., 2010) and internationally (Alkahtani, 2013; Sciutto, Nolfi & Bluhm, 2004).
The KADDS consists of three subscales. The first subscale measured general information related to ADHD, using 15 items. Items on the general knowledge subscale included: "Attention Deficit Disorder occurs in approximately 15% of all school-aged children", and "it is possible for an adult to be diagnosed with ADHD" (Sciutto et al., 2000).
The second subscale measures symptoms/diagnosis of ADHD using nine items. Items on the symptoms/diagnosis knowledge subscale included "Symptoms must not be present before age seven to be diagnosed with ADHD" and "children diagnosed with an attention deficit disorder tend to have poor concentration" (Sciutto et al., 2000).
The third subscale measured knowledge of the treatment of ADHD, using 12 items. Items on the treatment knowledge subscale included "Stimulant medication increases concentration" and "Electroconvulsive Therapy (ECT) is an effective treatment for Attention Deficit Disorder" (Sciutto et al., 2000).
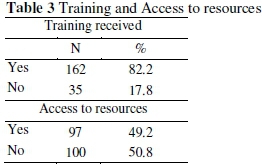
As two separate items, teachers were asked if they had received any training regarding ADHD, and whether they had access to resources concerning ADHD.
Two additional sections were added to the KADDS. These included sections for demographic information, classroom management and training received in terms of ADHD. The items in the demographic section included age, gender, ethnicity, marital status, number of years teaching, and the current grade level being taught. The section on the management of ADHD in the classroom contained 13 items, which were self-constructed, based on a review of the literature (DuPaul & Weyandt, 2006; Raggi & Chronis, 2006), to assess teachers' knowledge and level of support regarding the effectiveness of classroom interventions for children with ADHD. Participants responded to items in the classroom management section on a four-point Likert-type scale ranging from 1 = strongly disagree, to 4= strongly agree. In the data analysis process, the items were recoded to 1 = disagree, and 2 = agree. Interpretation of the responses for the items on teachers' knowledge and level of support regarding the effectiveness of classroom interventions was that higher responses or scores on the items indicated increased knowledge and support for classroom management.
Data Analysis
The data was entered, coded, cleaned and analysed by means of the Statistical Package in the Social Sciences (SPSS V21), so as to provide information in terms of percentages, frequencies, means and standard deviations. A descriptive analysis was conducted to see how responses to individual items were distributed. Percentage scores were calculated for correct responses, incorrect responses and "don't know" responses. These responses indicate knowledge of ADHD, misperceptions of ADHD and a lack of knowledge of ADHD, respectively.
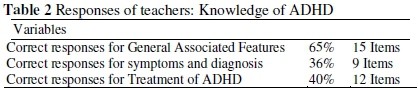
For the second subscale (see Table 2), symptoms and diagnosis of ADHD, responses were on nine items. The results suggest that 36% of the sample of teachers correctly identified the symptoms and diagnosis of ADHD in children.
The highest proportion of correct responses was given on Item 9 "children with ADHD often fidget or squirm in their seats": (86%, n = 172), while the lowest proportion of correct responses was given on Item 11: "it is common for children with ADHD to have an inflated sense of self-esteem or grandiosity". In terms of incorrect responses, the highest proportion was given on
Results
The results in Tables 2, 3 and 4 show the assessment outcome for primary school teachers' knowledge of ADHD in terms of symptoms and diagnosis, general associated features, and treatment of ADHD. The last column in this table indicates the number of items for each subscale.

Overall, 45% of the teachers correctly identified the responses to the items queried in the questionnaire. The "don't know responses" accounted for 31% of responses, while 22% of the responses were incorrectly identified.
For the first subscale (see Table 2), which is knowledge of general associated features of ADHD, responses were given for 15 items. The results indicate that 65% of the sample of teachers correctly identified the general associated features of ADHD.
The highest proportion of correct responses were given on Item 31: "children with ADHD are more distinguishable from children without ADHD in a classroom setting than in a free play situation" (76.4%, n = 152). The lowest correct responses were given on Item 30: "in very young children (less than 4 years old), the problem behaviours of ADHD children ([exempli gratia] e.g. hyperactivity, in-attention) are distinctly different from age appropriate behaviours of children without ADHD" (6%, n = 12). The highest incorrect responses were given on Item 27: "children with ADHD generally experience more problems in novel situations than in familiar situations" (63.8%, n = 127). Item 31 also received the lowest proportion of incorrect responses. The majority of teachers (59%, n = 118) selected "do not know" given on Item 6 "ADHD is more common in the 1st degree biological relatives ([id est] i.e. mother, father) of children with ADHD than in the general population".
Item 11, while the lowest proportion of incorrect responses was given on Item 16: "current wisdom about ADHD suggests two clusters of symptoms: One of inattention and another consisting of hyperactivity/impulsivity" (1%, n = 2). The majority of teachers (32.5%, n = 65) selected "do not know" for Item 11.
For the third subscale (see Table 2), treatment of ADHD, responses were given on 12 items. The results propose that 40% of the sample of teachers correctly identified the treatment for ADHD in children.
The highest proportion of correct responses were given on Item 10 "parent and teacher training in managing a child with ADHD are generally effective when combined with medication treatment" (79.5%, n = 159), while the lowest proportion of correct responses were given on Item 34: "behavioural/Psychological interventions for children with ADHD focus primarily on the child's problems with inattention" (17.1%, n = 34). The highest proportion of incorrect responses were given on Item 23: "reducing dietary intake of sugar or food additives is generally effective in reducing the symptoms of ADHD" (69.3%, n = 138), while the lowest number of incorrect responses were given on Item 10 (6%, n = 12). The majority of teachers (73.9%, n = 147) selected "do not know" for Item 35 "Electroconvulsive Therapy (i.e. shock treatment) has been found to be an effective treatment for severe cases of ADHD".
When asked if they had received any training and had access to resources regarding ADHD, the majority of teachers indicated that they had received training (82.2%). However, the frequency of responses was almost similar when asked whether or not teachers had access to resources regarding ADHD.
Table 4 presents the results of teachers' knowledge and perceptions of how children who have been diagnosed with ADHD ought to be managed in the classroom. In general, the results suggest that primary school teachers were mainly supportive of the suggestions for classroom management for children diagnosed with ADHD. Teachers were mainly supportive of using educational interventions (97%) and classroom rules (91%) for classroom management. These suggestions were followed by token reinforcement (86.9%), communication as intervention (86.4%), academic and social improvements (85%), learning expectations (84.3%), classwork broken into units (83.3%), repeating directions (82.8%), setting behavioural and learning expectations (80.8%). The least supported of the classroom management interventions were: time given for tests (58.4%); and ignoring the disruptive behaviour (66.7%) as approaches of classroom management.
Discussion
As an emerging economy, South Africa is committed to developing an education system that aims to redress barriers to learning. The adoption of inclusive education is one approach designed to ensure that children with disabilities are not excluded from the benefits of formal education (Department of Education, 2001). Inclusion in mainstream schools encourages schools (and teachers) to review the structures, approaches to teaching, student grouping and promote the schools to meet the diverse needs of all students (Farrell, 2003). One of the barriers to successful implementation of the policy of inclusive education in South Africa is a lack of teacher skills, and knowledge regarding their role in the intervention and management of disabilities such as ADHD in the classroom.
In the current study, overall, teachers responded correctly to less than 50% of the items on the KADDS. Twenty-two percent provided incorrect responses, which indicate a lack of knowledge of ADHD, while 31% had misper-ceptions regarding ADHD. When compared with findings of previous research, the results of the current study are almost similar to a previous local study (Perold et al., 2010) with slightly higher responses for knowledge and lower percentage responses for misperceptions, but the same percentage for a lack of knowledge. When compared to international research, Alkahtani (2013) found less correct responses (17.2%), incorrect responses (23%) but much higher misperceptions (59.8%) in a study conducted in Saudi Arabia, while Sciutto et al.'s (2000) study reported an average of 47.8% correct responses.
On further examination, the results suggest that teachers were more knowledgeable regarding the general associated features of ADHD than they were regarding the symptoms and diagnosis and treatment of ADHD. Across the subscales, lack of knowledge was found, particularly for "children with ADHD generally experience more problems in novel situations than in familiar situations"; "it is common for children with ADHD to have an inflated sense of self-esteem or grandiosity"; and "reducing dietary intake of sugar or food additives is generally effective in reducing the symptoms of ADHD". In terms of misperception, teachers indicated more responses for: "Electroconvulsive Therapy (i.e. shock treatment) has been found to be an effective treatment for severe cases of ADHD"; "it is common for children with ADHD to have an inflated sense of self-esteem or grandiosity"; and "ADHD is more common in the 1st degree biological relatives (i.e. mother, father) of children with ADHD than in the general population". These findings are somewhat different to previous research, but similar in particular for the mis-perception that children with ADHD have higher self-esteem, and that a high sugar diet has an effect on ADHD (Alkahtani, 2013). These responses may indicate that teachers required further training when it came to the identification of ADHD, since the teacher is often the first person to make a referral for assessment for ADHD (Malen, 2008).
For the current sample, the majority of teachers indicated that they had received training on ADHD. However, this training may have been once-off. Perhaps the training should be continuous, as teachers need to be knowledgeable not only about the etiology, diagnosis and prognosis of the disorder, but also how to manage children diagnosed with ADHD in the classroom in order to effect positive outcomes (Alkahtani, 2013; Perold et al., 2010). Furthermore, continuous training would ensure teachers are exposed to problem-solving situations, which may vary and differ for each child diagnosed with ADHD. This continuous training might also provide new approaches to managing children with ADHD in the classroom.
The majority of the current sample of teachers agreed to the suggested strategies for classroom management. These strategies included educational interventions, such as token reinforcement, communication, learning expectations, smaller units of classwork, setting behavioural and learning expectations and repetition of instructions. The least supported strategy, which is possibly the easiest and simplest to implement would be to provide more time for completion of tests. According to Emmer and Stough (2001), some features of classroom management could include: (1) an understanding of current research and theory in classroom management and its relationship to a learners' psychological and learning needs; (2) the ability to create a positive relationship between the learner and the educator and (3) instructional methods that respond to the academic needs of each learner and to the group as a class. Research suggests that there are positive interventions for effectively instructing children with ADHD in the classroom setting (DuPaul & Weyandt, 2006; Raggi & Chronis, 2006). These interventions may include behavioural (token reinforcement), social (social skills training), academic (peer tutoring) supports (DuPaul & Weyandt, 2006), computer-assisted instruction, task modifications, self-monitoring, and strategy training for the youth themselves (Raggi & Chronis, 2006). Some basic strategies for academic interventions involve choice making, which allows the student to choose between different classroom activities or tasks. The active teaching of rules including having teachers continually remind the student of classrooms rules verbally and by example, has also been shown to reduce classroom behaviour problems (DuPaul & Stoner, 2003; DuPaul & Weyandt, 2006). Studies have indicated that computer-assisted instruction may also be effective in improving the reading and mathematics skills of children with ADHD (Clar-field & Stoner, 2005; Mautone, DuPaul & Jitendra, 2005). In the United States of America (USA), school-based interventions form part of the treatment regimen for ADHD (Schultz et al., 2011). It is likely that teachers, in the current study, know which interventions can be used to effectively manage ADHD in the classroom, but there is a lower degree of support for these interventions. This could be due to many factors, which could be: 1) Lack of resources at schools, and 2) Support to teachers by making use of support personnel (students/additional assistant teachers to assist with the children with special needs in the classroom).
The findings of this study suggest that there is a need to consider school regulations that will ensure teachers in South African schools have the skills necessary to implement school-based interventions for ADHD. While a few affluent urban schools in the country have access to school counsellors, the majority of schools have no resources in terms of classroom management of ADHD. The success of inclusive education in the country can only be realised if schools are equipped to effectively deal with the diverse needs of all learners.
Conclusion
The purpose of this study was to investigate primary school teachers' knowledge of ADHD, and its management in the classroom. The results of this study may be helpful towards investigating undergraduate teacher education programmes and in-service training for ADHD, so as to determine what information teachers actually receive about this disorder. Asking teachers what steps they take when a child is exhibiting specific inappropriate behaviour may also provide information regarding teachers' knowledge, training, and application of interventions/management techniques. It would therefore be advantageous to have school psychologists work as consultants to teachers, where they might be able to observe teachers working with a child with ADHD, to help them implement interventions, and interview them about their techniques and barriers. Furthermore, since research suggests a multidisciplinary approach to working with children with ADHD, the amount of support provided to teachers would be useful to include in future studies. It would be helpful if the Department of Basic Education could either revise their decision of doing away with "special needs classes", or put in place District Support Teams to assist the teachers who have to work with children with special needs. Should management techniques be implemented, the academic and social outcomes for children with ADHD could improve. Children displaying symptoms of ADHD might therefore be assisted in order to function to their full potential and support their well-being. This could contribute to a more effective education system, which could thereby prepare all learners thoroughly in becoming productive members of our emerging economy.
Acknowledgement
We would like to thank the Northern Cape Department of Education for allowing us to conduct the study.
References
Alkahtani KDF 2013. Teachers' knowledge and misconceptions of attention deficit/hyperactivity disorder. Psychology, 4(12):963-969.doi: 10.4236/psych.2013.412139 [ Links ]
American Psychiatric Association 2013. Diagnostic and Statistical Manual of Mental Disorders (5th ed) (DSM-5). Washington: American Psychiatric Association. [ Links ]
Anastopoulos AD & Farley SE 2003. A cognitive- behavioral training program for parents of children with attention-deficit/hyperactivity disorder. In AE Kazdin & JR Weisz (eds). Evidence-based psychotherapies for children and adolescents. New York:Guilford Press. [ Links ]
Barkley RA 2005. Taking Charge of ADHD: The Complete, Authoritative Guide forParents. New York: Guilford Press. [ Links ]
Clarfield J & Stoner G 2005. The effects of computerized reading instruction on the academic performance of students identified with ADHD. School Psychology Review, 34(2):246-254. [ Links ]
Davies R 2010. Identifying a weakness in the UK education system of supporting children with complex social, emotional and behavioural difficulties/ADHD - is government policy preventing effective inclusion for some pupils? Doctoral Dissertation. United Kingdom: University of Greenwich. [ Links ]
Department of Education 2001. Educational White Paper 6: Special needs education (Building an Inclusive Education and Training System). Pretoria: DoE. Available at http://www.education.gov.za/LinkClick.aspx?fileticket=gVFccZLi/tI=. Accessed 7 March 2015. [ Links ]
Dore G 2010. Identification and coping with ADHD learners in the mainstream classroom. Presentation by psychological guidance support and educational services (PGSES), 24 May. [ Links ]
DuPaul GJ & Stoner G 2003. ADHD in the Schools. Assessment and Intervention Strategies (2nd ed). New York: Guilford Press. [ Links ]
DuPaul GJ & Weyandt LL 2006. School-based intervention for children with Attention Deficit Hyperactivity Disorder: Effects on academic, social, and behavioural functioning. International Journal of Disability, Development and Education, 53(2):161-176. doi: 10.1080/10349120600716141 [ Links ]
Emmer ET & Stough LM 2001. Classroom management: A critical part of educational psychology, with implications for teacher education. Educational Psychologist, 36(2):103-112. [ Links ]
Farrell M 2003. Understanding Special Educational Needs: A Guide for Student Teachers. London: Routledge Falmer. [ Links ]
Hariparsad SD 2010. Challenges facing educators' in the inclusion of attention deficit hyperactivity disordered (ADHD) learners in the mainstream classroom. Unpublished master's thesis. KwaZulu Natal, SA: University of Zululand. [ Links ]
Kashala E, Tylleskar T, Elgen I, Kayembe KT & Sommerfelt K 2005. Attention deficit and hyperactivity disorder among school children in Kinshasa, Democratic Republic of Congo. African Health Sciences, 5(3):172-181. [ Links ]
Lopes T, Eloff I, Howie S & Maree JG 2009. South African teachers' experiences of children in their classrooms who may have ADHD. Journal of Psychology in Africa, 19(3):347-354. doi: 10.1080/14330237.2009.10820301 [ Links ]
Mahomedy Z, Van der Westhuizen D, Van der Linde MJ & Coetsee J 2007. Persistence of attention deficit/hyperactivity disorder into adulthood: a study conducted on parents of children diagnosed with attention deficit/hyperactivity disorder. South African Psychiatry Review, 10(2):93-98. [ Links ]
Malen M 2008. Teacher ADHD referral theory modification may reduce referrals for student ADHD diagnosis. Doctoral dissertation. Minneapolis: University of Minnesota. [ Links ]
Mautone JA, DuPaul GJ & Jitendra AK 2005. The effect of computer assistedinstruction on the mathematics performance and classroom behavior of children with ADHD. Journal of Attention Disorders, 9(1):301-312. [ Links ]
Muthukrishna N 2013. The geographies of the schooling experiences of children labelled attention deficit hyperactivity disorder (ADHD). Anthropologist, 15(2):145-156. Available at http://www.krepublishers.com/02-Journals/T-Anth/Anth-15-0-000-13-Web/Anth-15-2-000-2013-Abst-PDF/T-ANTH-15-2-145-13-822-Muthukrishna-N/T-ANTH-15-2-145-13-822-Muthukrishna-N-Tx%5B4%5D.pmd.pdf. Accessed7 March 2015. [ Links ]
Nel N, Nel M & Hugo A 2013. Learner support in a diverse classroom: A guide for foundation, intermediate and senior phase teachers of language and mathematics. Pretoria: Van Schaik Publishers. [ Links ]
Ofovwe CE, Ofovwe GE & Meyer A 2006. The prevalence of attention deficit/hyperactivity disorder among school-aged children in Benin City, Nigeria. Journal of Child and Adolescent Mental Health, 18:1-5. [ Links ]
Perold H, Louw C & Kleynhans S 2010. Primary school teachers' knowledge and misperceptions of attention deficit hyperactivity disorder (ADHD). South African Journal of Education, 30(3):457- 473. [ Links ]
Polanczyk G, De Lima MS, Horta BL, Biederman J & Rohde LA 2007. The worldwide prevalence of ADHD: A systematic review and meta-regression analysis. American Journal of Psychiatry, 164(6):942-948. [ Links ]
Raggi VL & Chronis AM 2006. Interventions to address the academic impairment of children and adolescents with ADHD. Clinical Child and Family Psychology Review, 9(2):85-111. [ Links ]
Ramphal A 2010. ADHD - a child's view. Daily News, 29 July. [ Links ]
Sadock BJ, Sadock VA & Ruiz P 2015. Synopsis of psychiatry: Behavioral Sciences/Clinical Psychiatry (11th ed). New York: Wolters Kluwer. [ Links ]
Schellack N & Meyer H 2012. The management of attention deficit-hyperacivity disorder in children. South African Pharmaceutical Journal, 79(10):12- 20. Available at http://www.sapj.co.za/index.php/SAPJ/article/viewFile/1392/2181. Accessed 7 March 2015. [ Links ]
Schultz BK, Storer J, Watabe Y, Sadler J & Evans SW 2011. School based treatment of attention-deficit/hyperactivity disorder. Psychology in the Schools, 48(3):254-262. doi: 10.1002/pits.20553 [ Links ]
Sciutto MJ, Nolfi CJ & Bluhm C 2004. Effects of child gender and symptom type on referrals for ADHD by elementary school teachers. Journal of Emotional and Behavioral Disorders, 12(4):247-253. doi: 10.1177/10634266040120040501 [ Links ]
Sciutto M, Terjesen MD & Frank ASB 2000. Teachers' knowledge and misperceptions of attention- deficit/hyperactivity disorder. Psychology in the Schools, 37(2):115-122. [ Links ]
Snider VE, Busch T & Arrowood L 2003. Teacher knowledge of stimulant medication and ADHD. Remedial and Special Education, 24(1):46-56. [ Links ]
Willcutt EG, Doyle AE, Nigg JT, Faraone SV & Pennington BF 2005. Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biological Psychiatry, 57(11):1336-1346. [ Links ]
Wolraich ML, Lambert EW, Baumgaertel A, Garcia- Tornel S, Feurer ID, Bickman L & Doffing MA 2003. Teachers' screening for attention deficit/hyperactivity disorder: comparing multinational samples on teacher ratings of ADHD. Journal of Abnormal Child Psychology, 31(4):445-455. [ Links ]

