










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.62 n.1 Cape Town 2024
http://dx.doi.org/10.36303/SAJS.00216
PAEDIATRIC SURGERY
A dedicated quality improvement programme can increase access to paediatric minimal access surgery in South Africa
H MangrayI; S MadzibaI; ANgobeseI; MTD SmithI; DL ClarkeI, II
IDepartment of Paediatric Surgery, Greys Hospital, University of KwaZulu-Natal, South Africa
IIDepartment of Surgery, University of the Witwatersrand, South Africa
ABSTRACT
BACKGROUND: In this project, we reviewed our experience in minimal access paediatric surgery (MAPS) at Greys Hospital over the last decade. This information would provide an overview of our experience and would enable us to identify areas where we can strengthen our surgical service and our training programme
METHOD: All surgical patients are captured in the hybrid electronic medical registry (HEMR). All patients aged 18 years or less who underwent a MAPS procedure between 2012 and 2021 were reviewed. Data collected included demographic information, type of surgery, nature of the surgery (elective or emergency), organ system operated on, whether trainees or consultants performed the surgeries and the morbidities and mortalities experienced. Statistical analysis included linear regression and ANOVA, which was performed using Jamovi software
RESULTS: A total of 1 328 MAPS procedures were performed on 994 patients over nine years. There were 359 female and 635 male patients. There was a steady increase in the number of cases performed per year. The age of the patients ranged from one day of life to 18 years, with a median of 8 years. The multiple linear regression results indicated a very strong collective significant effect between the courses performed, the number of consultants, and the MAPS cases performed. The ANOVA test for the individual factors was not statistically significant, but there was a very strong combined correlation with an r-value of 0.87 and a p-value of 0.014 using the overall model test. The consultants' training also directly impacted on the teaching and training of registrars, with progressively more cases being performed by trainees over the years. Postoperative morbidity was reported in 40 patients. The morbidity rate was three per cent. There were no mortalities
CONCLUSION: It is feasible to deliver MAPS to children in our environment. A comprehensive quality improvement strategy has yielded satisfying results. The increased use of MAPS has resulted in a general transfer of skills to junior staff. Ongoing efforts to support the rollout of MAPS in children are warranted
Keywords: paediatric surgery, minimal access surgery, training, laparoscopy
Introduction
The Lancet Commission on Global Surgery has demonstrated that there is a discrepancy in access to safe surgery across the globe. Almost five billion people, including 1.7 billion children and adolescents, who primarily reside in low to middle-income countries (LMIC), do not have access to safe surgery.1,2 Minimal access paediatric surgery (MAPS) has progressed dramatically over the last four decades and can no longer be regarded as experimental. MAPS is now a core component of safe and effective surgical care, with well-documented health outcome benefits.3 Despite these manifest benefits, there is good evidence to suggest that the uptake of MAPS is unequally distributed.
In South Africa (SA), minimal access approaches for adults and children are readily available in the private sector, but the situation is less evident in the state sector. In a review of the surgical output in KwaZulu-Natal province over a six-month period in 2015, less than half of all cholecystectomy procedures were performed laparoscopically. The situation with acute appendicitis is similar, with the majority of appendectomy procedures being performed via an open approach.3 This compromises both patient care and surgical training, as surgical training occurs in the state sector institutions. There are many reasons for this inadequate access. These include cost, lack of local training courses, travel-related expenses that limit attendance of international training courses, and lack of equipment or simulators.4
Beginning in 2015, the paediatric surgical department in Pietermaritzburg embarked on an active programme to expand access to MAPS. Initially, this involved increased attendance by the paediatric and adult surgical consultants at external training courses both abroad and at other centres in the country. In 2021 during the COVID-19 pandemic, this programme was strengthened by the rollout of a locally developed programme and skills laboratory. Industry-sponsored Telepack (Karl Storz) systems and box trainers were used to teach knot tying and other basic laparoscopic skills, and a course was developed to provide instruction.5 This course was initiated in 2021 and has been run every three months for the last two years. Considering the above, we set out to review our experience in MAPS at Greys Hospital over the last decade. It was hoped that this information would provide an overview of our experience and would enable us to identify areas where we can strengthen our surgical service and our training programme.
Method
Greys Hospital is a tertiary academic centre in Pietermaritzburg, KwaZulu-Natal, SA. Greys Hospital provides tertiary surgical services for a population of 4.5 million people. It is estimated that one-third of patients at Greys Hospital are children. The department of surgery has maintained a hybrid electronic medical registry (HEMR) since 2012. All surgical patients are captured in the HEMR. We use the World Health Organization (WHO) definition of paediatric, and all patients less than 18 years of age are considered to be paediatric - we refer to this cohort as comprising children and adolescents. All patients aged 18 years or less who underwent either a laparoscopic or thoracoscopic procedure between 2012 and 2021 were reviewed. The cases were performed by trainees and consultant surgeons. Anaesthesia was provided by specialist anaesthetists, and the cases were performed in general operating theatres using 3 mm and 5 mm instruments. Data collected included demographic information, type of surgery, nature of the surgery (elective or emergency), organ system operated on, whether trainees or consultants performed the surgeries and any morbidities and mortalities experienced. Data was compared to the number of open cases performed in the defined study period. Follow-up was for a minimum of one year but up to a maximum of 8 years. Statistical analysis was performed using Jamovi software.
Linear regression and ANOVA were used to investigate the relationship between the number of consultants, training courses performed by consultants and output in terms of the number of MAPS cases performed each year.
Results
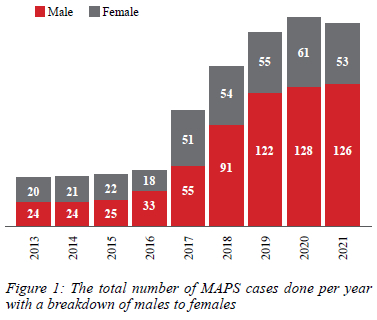
A total of 1 328 MAPS procedures were performed on 994 patients over nine years. There were 359 female and 635 male patients. There was a steady increase in the number of cases performed per year, as demonstrated in Figure 1.
The age of the patients ranged from one day of life to 18 years, with a median of 8 years. There were 315 cases performed in the infantile group. Ten cases were performed on neonates less than one week old, and the most significant number of cases were performed on infants of three months (Figure 2).
The number of cases performed for each age group of children from one to 18 years is represented in Figure 3, with the most significant number of cases performed in the one-year-old group.
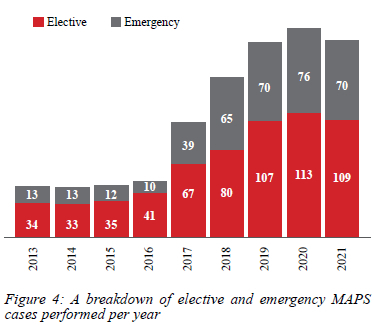
The number of elective and emergency MAPS cases increased progressively over the study period, as shown in Figure 4.
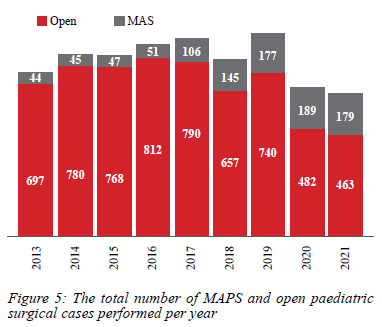
The proportion of MAPS cases performed each year of the total number of paediatric surgical cases progressively increased (Figure 5).
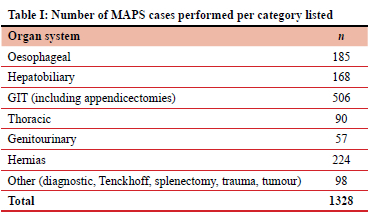
The most significant number of MAPS cases were performed on gastrointestinal tract pathology, including appendectomy, hernia repair, and oesophageal procedures. There was also a large number of hepatobiliary cases performed. Video-assisted thoracic procedures included a total of 90 cases. Splenectomy and laparoscopy for tumours comprised the smallest number of cases (Table I). A total of 68 MAPS cases were converted to an open procedure. The conversion rate was 5.1% (Table II).
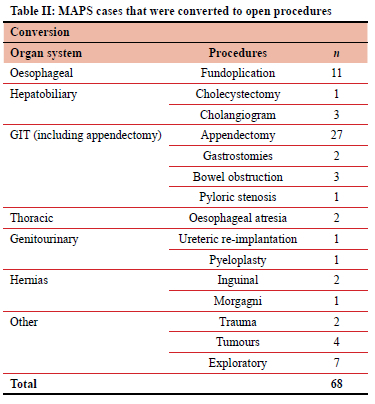
The most significant number of converted cases were for complex appendicitis (27). Oesophageal MAPS cases requiring conversion amounted to 11 cases, followed by exploratory laparoscopies seven. Postoperative morbidity, classified as Clavien-Dindo III and IV, was reported in 40 patients (Table III).
Repeat laparotomy, bowel perforation, and liver trauma were the main morbidities reported. The morbidity rate for the study group was three per cent. There were no mortalities. Figure 6 shows how increased training and exposure to MAPS have impacted on the number of MAPS cases performed.
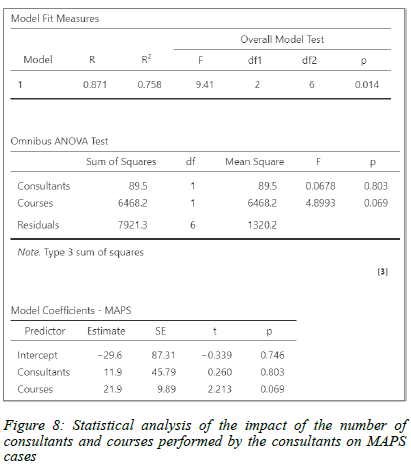
There was a steady increase in the number of MAPS cases performed by consultants, staff and trainees between 2015 and 2021. The difference between the absolute number of MAPS cases performed by consultants and trainees gradually narrowed over the five years from 2016-2021. In 2019 there was a peak in the absolute number of cases performed by attendants. By 2021 trainees performed more MAPS cases than attendants (Figure 7). The multiple linear regression results indicated a very strong collective significant effect between the courses performed, the number of consultants, and the MAPS cases performed (Figure 8). The ANOVA test for the individual factors was not statistically significant, but there was a very strong combined correlation with an r-value of 0.87 and a p-value of 0.014 using the overall model test.
Trainees who performed MAPS cases were either under the supervision of the attendant or alone. The majority of trainee-performed MAPS cases were laparoscopic appendicectomies.
Discussion
MAPS has become part of the standard of care in surgery over the last three decades. Initially, cholecystectomy and appendectomy were the most common operations performed via minimal access; however, increasingly complex operations are being performed in limited resource centres.6 The performance of MAPS cases has certainly become a routine part of the paediatric surgical practice at our institution. It has contributed to the teaching and training of surgeons and benefited patients. There remain many barriers to accessing and delivering minimal access surgery (MAS) globally in both high-income and middle- and low-income countries. Wilkinson et al. assessed the barriers that impacted laparoscopic training in LMIC and noted that funding, equipment, experienced trainers, and lack of opportunity were the major barriers.7 The current situation in SA parallels the developing world, where we have limited access to funding, equipment, and training programmes for MAPS.8-10 A recent review from Switzerland revealed nationwide discrepancies in access to MAS, which tend to discriminate against older comorbid patients, those lacking private insurance, lower-income patients, and those residing in rural areas.11 When it comes to surgery for children and adolescents, the situation is even more inequitable. In SA and sub-Saharan Africa, the demographic breakdown is heavily weighted toward young people. However, the burden of paediatric surgical disease is poorly defined, and the system of delivering surgical care to children is poorly structured and inadequate.12,13 Our data clearly showed that as the number of trainers increased, the number of MAPS cases increased. The industry-supported local course that we established was affordable and eliminated the need for travel and funding. All the above factors led to an increase in the number of cases performed by trainees, surpassing the number of cases performed by consultants. So, whilst MAPS has a significant role to play in safe and effective paediatric surgical care, its availability in the region is unclear.14
The review of our data has clearly demonstrated an increasing trend in the number of MAPS cases performed each year over the study period. There was an equivalent increase in elective and emergency cases, and more younger children had MAPS procedures. The most significant number of cases performed was in the under five-year age group, contrasted with a publication from Nigeria in 2020, where the most significant group was the 5-10 years old.6 The global COVID-19 pandemic hindered the number of MAPS cases performed during 2020 and 2021, but despite this, the number was higher compared to previous years.
The review being retrospective has inherent limitations. A more detailed review of cases performed by trainees and learning curves was beyond the scope of this study. Further studies will be required to assess the future impact of the Greys laparoscopic suturing course (GLSC).
This project has shown how a single unit has managed to deliver an increasing level of MAS to children over a decade. There is an increasing trend in the number of MAPS cases performed each year. There was an equivalent increase in elective and emergency cases and an increasing number of younger children undergoing a MAPS procedure. The largest number of cases performed was in the under-five-year age group. A wide range of procedures was performed within the thorax and abdomen, with an overall conversion rate of 5.1%, which is in keeping with the literature.6,15 A dedicated quality improvement programme designed to increase access to MAPS has delivered positive results. The establishment of a skills laboratory and a dedicated training programme, despite limited resources, has increased the absolute number as well as the type and complexity of MAPS procedures performed by both consultants, staff and trainees.
Conclusion
It is feasible to deliver MAPS to children in our environment. A comprehensive quality improvement strategy has yielded satisfying results. The increased training and use of MAPS have resulted in a general transfer of skills to junior staff. Ongoing efforts to support the rollout of MAPS in children are warranted.
Conflict of interest
The authors declare no conflict of interest.
Funding source
None.
Ethical approval
Ethical approval was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee BREC/0000/5035/2022.
ORCID
H Mangray https://orcid.org/0000-0002-5204-3542
S Madziba https://orcid.org/0000-0003-4077-3465
A Ngobese https://orcid.org/0000-0002-1024-8478
MTD Smith https://orcid.org/0000-0002-6954-153X
DL Clarke https://orcid.org/0000-0002-8467-1455
REFERENCES
1. Meara JG, Leather AJM, Hagander L, et al. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386(9993):569-624. [ Links ]
2. Mullapudi B, Grabski D, Ameh E, et al. Estimates of number of children and adolescents without access to surgical care. Bull World Health Organ. 2019;97(4):254-8. https://doi.org/10.2471/BLT.18.216028. [ Links ]
3. Yardley I, Kenny S. Minimally invasive surgery in paediatric patients. Paediatr Child Health. 2014;24(5):185-91. https://doi.org/10.1016/j.paed.2013.10.001. [ Links ]
4. Naidoo M. Trends in adoption of laparoscopic appendicectomy in a developing country: Closing the gap. World J Surg. 2022;7. https://doi.org/10.1007/s00268-022-06454-8. [ Links ]
5. Mangray H, Madziba S, Harilal S, et al. Developing a novel laparoscopic training model during the Covid-19 pandemic in a resource-limited setting. Surg Pract Sci. 2023;13:100170. https://doi.org/10.1016/j.sipas.2023.100170. [ Links ]
6. Igwe A, Talabi A, Adumah C, et al. Mitigating the challenges of laparoscopic paediatric surgery in Ile Ife: The trend so far and lessons learnt. Afr J Paediatr Surg. 2020;17(3):68. https://doi.org/10.4103/ajps.AJPS_32_20. [ Links ]
7. Wilkinson E, Aruparayil N, Gnanaraj J, Brown J, Jayne D. Barriers to training in laparoscopic surgery in low- and middle-income countries: A systematic review. Trop Doct. 2021;51(3):408-14. https://doi.org/10.1177/0049475521998186. [ Links ]
8. Jooma U, Numanoglu A, Cox S. Paediatric surgery training in South Africa: Trainees' perspectives. Pediatr Surg Int. 2020;36(12):1489-94. https://doi.org/10.1007/s00383-020-04744-7. [ Links ]
9. Patel N, Leusink AL, Singh N, Koto MZ, Luvhengo T. Registrar perceptions on general surgical training in South Africa: A report by the South African Society of Surgeons in Training (SASSiT). South Afr J Surg. 2018;56(2):10-4. [ Links ]
10. Stevens PS, Villiers MD, Niekerk MV. A survey on the current status of laparoscopic training in paediatric surgery in South Africa. 2011;49(1):3. [ Links ]
11. Schneider MA, Gero D, Müller M, et al. Inequalities in access to minimally invasive general surgery: A comprehensive nationwide analysis across 20 years. Surg Endosc. 2021;35(11):6227-43. https://doi.org/10.1007/s00464-020-08123-0. [ Links ]
12. Bickler SW, Rode H. Surgical services for children in developing countries. Bull World Health Organ. 2002;80(10):829-35. [ Links ]
13. Bickler SW, Kyambi J, Rode H. Paediatric surgery in sub-Saharan Africa. Pediatr Surg Int. 2001;17(5-6):442-7. https://doi.org/10.1007/s003830000516 [ Links ]
14. Loveland J, Numanoglu A, Hay SA. Paediatric minimally invasive surgery in Africa: limitations and current situation. Semin Pediatr Surg. 2012;21(2):160-3. https://doi.org/10.1053/j.sempedsurg.2012.01.008. [ Links ]
15. Gupta AR, Gupta R, Jadhav V, Sanghvi B, Shah HS, Parelkar SV. Minimal access surgery in children: An initial experience of 28 months. Afr J Paediatr Surg AJPS. 2009;6(2):93-7. https://doi.org/10.4103/0189-6725.54771. [ Links ]
 Correspondence:
Correspondence:
H Mangray
Email: mangrayh@ukzn.ac.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}