










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.61 no.4 Cape Town 2023
http://dx.doi.org/10.36303/sajs.3511
HPB SURGERY
HIV associated malignancies presenting as acute pancreatitis: a case series
F MadelaI; F AndersonI; GB NhlonziII; SR ThomsonIII
IDepartment of Surgery, Surgical Gastroenterology, University of KwaZulu-Natal, South Africa
IIDepartment of Anatomical pathology, University of KwaZulu-Natal, South Africa
IIIDivision of Gastroenterology, Department of Medicine, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: Acute pancreatitis (AP) may be the presenting symptom in a small percentage of patients harbouring pancreatic or extra pancreatic tumours. This case series aims to describe the pathological spectrum of tumours detected in two AP cohorts from a high HIV-endemic region.
METHODS: Prospectively collected databases of patients admitted with AP over two periods 2001 to 2010 and 2013 to 2015, were retrospectively evaluated to detect those with pancreatic and extra-pancreatic tumours. The diagnosis of AP was by standard criteria. HIV infection and CD4 counts were routinely tested for in the latter period and only tested on clinical grounds in the initial period. CT scan was performed when there was diagnostic doubt, predicted severe disease, and failure to improve clinically after one week. Demographic, clinical, investigative, and pathology details were collected and presented.
RESULTS: HIV-positive patients admitted with AP were 106 (17%) of 628 in the first period and 90 (38%) of 238 of the second period. No tumours were diagnosed in the HIV-negative patients. Seven of the HIV-positive patients had tumours diagnosed at endoscopy, CT scan, and endoscopic retrograde cholangiography. Of the seven HIV-positive patients with tumours, two patients had a CD4 count above 200. There were four patients with lymphoma involving the pancreatic head, three having associated cholestasis, and three patients with Kaposi's Sarcoma. One Kaposi's sarcoma patient died three months after presentation. One patient with lymphoma died on day 14 and another two months after initial presentation, and the remaining four patients were referred to oncology.
CONCLUSION: Despite their rarity (< 4%), when HIV-positive patients with low CD4 count and cholestasis present with AP, tumours should be suspected and evaluated by cross sectional imaging and endoscopic ultrasound.
Keywords: Acute pancreatitis, HIV, AIDS defining malignancies
Introduction
Pancreatic malignancies may present as acute pancreatitis (AP) in 2% of cases.1 The malignancies are diagnosed at initial presentation or over a varying period thereafter.1 Non-pancreatic malignancies may also be associated with hyperamylasaemia.2,3,4 In HIV-positive patients, there is an association with AIDS defining malignancies (Kaposi's sarcoma, high grade B-cell non-Hodgkin's lymphoma).5,6,7 The advent of highly active antiretroviral therapy (HAART) has seen a decline in the overall incidence of Kaposi's sarcoma and non-Hodgkin's lymphoma, and an increase in non-AIDS defining tumours.7,8,9,10 This case series aims to describe the pathological spectrum of tumours detected in combined prospective AP cohorts accrued over the last two decades from a high HIV-endemic region.
Methods
Two prospectively collected datasets (2001 to 2010 and 2013 to 2015), whose primary analysis was to study the outcomes of hyperlipidaemia in AP11 and the effect of HIV infection on the predictors of severity in AP,12 respectively, were used to identify those with pancreatic and extra pancreatic tumours. Demographic, clinical, investigative, and pathology details were collected and presented. The diagnosis of pancreatitis was by clinical criteria plus an amylase or lipase of > 3 times the upper limit of normal, urine amylase > 1000 U/L, or evidence of AP on CT scan or at surgery. In the initial period, HIV infection and CD4 counts were documented from the medical history and in the second period, patients were routinely counselled and tested for HIV infection. CT scan was performed when there was diagnostic doubt, predicted severe disease, and failure to improve clinically after 1 week.
Patient information was de-identified and descriptive statistics were used.
Ethical approval for the analysis was obtained from the Biomedical Research Ethics Committee of the University of Kwazulu-Natal, BE222/11.
Results
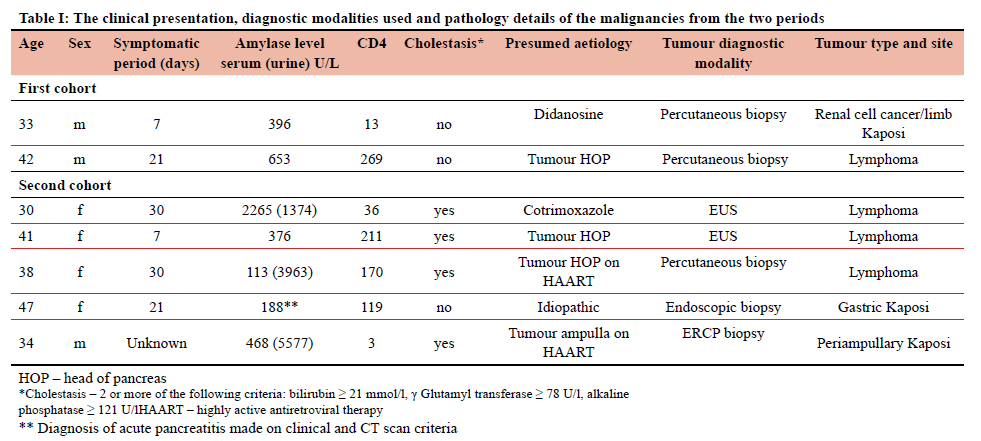
A total of 628 and 238 patients had AP in the first and second periods, respectively. Of these, 17% (106) and 38% (90) were HIV-positive, respectively. Tumours were detected in two patients from the first period and five patients from the second period. Table 1 describes the clinical presentation, diagnostic modalities used and pathology details of the malignancies from the two periods. In the first period 48% (51) of the HIV-positive patients had CD4 counts of less than 200 cells/mm3 (mean 220 cells/mm3), and in the second period there were 30% (27) (mean 335 cells/mm3). The number of patients on HAART in each period was 60% and 59%, respectively. No tumours were diagnosed in the HIV-negative patients. The tumours were predominantly diagnosed by CT scan and EUS. In the first period, 179 CT scans were performed (60 HIV-positive and 119 HIVnegative), and in the second period, 33 CT scans were performed (16 HIV-positive and 17 HIV-negative). Most patients were younger than 40 years, and symptom duration ranged from 7 to 30 days. Five patients with malignancies had CD4 counts less than 200 cells/mm3. Three of the four patients with non-Hodgkin's lymphoma (NHL) involving the head of the pancreas had associated cholestasis. One patient with Kaposi's sarcoma (KS) and renal cell carcinoma died within 3 months of presentation. Two lymphoma patients died shortly after presentation, at 2 and 8 weeks, while the outcomes of the others who were referred for oncological therapy are unknown.
Discussion
This case series provides insight into the clinical presentation of HIV associated malignancies that will be encountered while managing patients with AP. In this dataset, cross sectional imaging was only performed in patients with diagnostic doubt or severe disease potentially resulting in an underestimate of the number of patients harboring tumours. In this sizeable, combined cohort there were no patients who had tumours of a pancreatic exocrine cell lineage. Previous studies have reported variable frequencies of pancreatic malignancies associated with AP. In a population-based study in the US, there is a reported association of AP with all-types pancreatic cancers of 0.15% in 945 253 patients in the period from 2002 to 2005, and 0.26% in 1070792 patients in the period from 2009 to 2012 (p = < 0,001) suggesting either an increase in incidence or better detection.13 In a series reporting on the corollary, 24 (13.8%) of 174 patients operated on for pancreatic cancer presented with AP.14 In the same study, hyperamylasaemia without clinical pancreatitis was observed in a further 17 patients (9.8%) with pancreatic cancers.14 This is in stark contrast to another case series of 302 patients with pancreatic cancers in which only 3% (10) had prior AP. 15
Primary pancreatic lymphoma (PPL) is rare, and the clinical and diagnostic criteria includes a predominant mass involvement of the pancreas with lymph node spread confined to the peripancreatic region.16,17,18 A systematic review of 107 eligible papers on PPL from 2001 to 2020 yielded 266 patients. Information on diagnostic procedures was available in 224. Sixty-eight (30.3%) were diagnosed on percutaneous biopsy, 39 (17.4%) with endoscopy, 33 (14.8%) with FNA, and 26 (11.6%) at surgery. Of the 218 patients with a complete dataset, 56 (26%) presented with AP. The predominant histological subtype was diffuse large B cell lymphoma (56%) in the age above 18 years, and Burkitt lymphoma (52.4%) in the age group below 18 years. Two of these patients were immunosuppressed following renal and pancreatic transplants. The HIV status of these 218 patients was not reported in the systematic review and the association with HIV infection is confined to case reports.19,20,21
In our case series, all the cases were NHL in HIV-positive patients, although NHL has been reported as a cause of AP in HIV-negative individuals.10,19 The frequencies of non-exocrine pancreatic malignancies in our study was 0.5% of 866 in the overall cohort, and 2% in 196 of the HIV-positive cohort.
Several non-pancreatic cancers of the kidney, ovary, cervix, lung, adrenal phaeochromocytomas and multiple myeloma are known to secrete amylase.14,15,16,17 In the present series, one of the patients presented with stage four renal cell carcinoma which was diagnosed by CT scan following symptoms of AP that persisted beyond one week.
Kaposi's sarcoma (KS), a malignancy of the vascular endothelium, is found in the skin and other organs. Human Herpes virus 8 is established as an important factor in the development of KS irrespective of HIV status.22 In a Tanzanian study of 248 patients with KS, 49% had AIDS; 12 (3.1%) involved the viscera (4 rectal, 6 intestinal and 2 gastric).23 In the present series, the KS lesion at the ampulla of Vater was thought to be the cause of the pancreatitis and the extra pancreatic lesions were thought to be incidental findings.
Three of the seven patients were on HAART and showed features of treatment failure with all having CD4 counts less than 200 (CD4 counts of 3, 13 and 170 respectively). The rest of the patients were below the threshold for HAART in 2014. This reveals that there are patients not on HAART despite advanced HIV infection. This low number of patients on HAART (less than two thirds), in combination with treatment failure, is likely to result in persistence of AIDS defining malignancies.
Conclusion
In these combined cohorts of patients with AP, it is notable that cancers of pancreatic exocrine cell lineage were not observed, regardless of HIV status. However, routine CT scan based on clinical grounds rather than routinely may have resulted in under detection. Despite this limitation, HIV-positive patients with a low CD4 count presenting with AP and cholestasis, are most likely to harbour a PPL. In this group of patients more liberal use of cross-sectional imaging and endoscopic ultrasound is indicated to evaluate for an AIDS defining malignancy as potential aetiology.
Conflict of interest
The authors declare no conflict of interest.
Funding source
None
Ethics
Ethical approval for the analysis was obtained from the Biomedical Research Ethics Committee of the University of Kwazulu-Natal, BE222/11.
ORCID
F Madela https://orcid.org/0000-0002-5663-3160
F Anderson https://orcid.org/0000-0002-9055-8037
GB Nhlonzi https://orcid.org/0000-0002-5478-7078
SR Thomson https://orcid.org/0000-0002-9485-997X
REFERENCES
1. Gislason H, Horn A, Hoem D, et al.Acute Pancreatitis in Bergen, Norway. Scandinavian Journal of Surgery. 2004;93(1):29-33. https://doi.org/10.1177/145749690409300106 [ Links ]
2. Srivastava R, Fraser C, Gentleman D, et al. Hyperamylasaemia: not the usual suspects: British Medical Journal. 2005;331(7521):890-891. https://doi.org/10.1136/bmj.331.7521.890 [ Links ]
3. Ho ET, Gardner DS. Paraganglioma with acute hyperamylasaemia masquerading as acute pancreatitis. Singapore Medical Journal. 2011;52(12):e251-4. PMID: 22159946 [ Links ]
4. Calvo-Villas JM, Alvarez I, Carretera E, et al. Paraneoplastic Hyperamylasaemia in Association with Multiple Myeloma. Acta Haematolologica. 2007;117(4):242-245. https://doi.org/10.1159/000100931 [ Links ]
5. Hermans P. Opportunistic AIDS-associated malignancies in HIV-infected patients. Biomedicine and Pharmacotherapy 2000;54(1):32-40. https://doi.org/10.1016/S0753-3322(00)88638-2 [ Links ]
6. Bower M, Palmieri C, Dhillon T. AIDS-related malignancies: changing epidemiology and the impact of highly active antiretroviral therapy. Current Opinions in Infectious Diseases. 2006;19(1):14-19. https://doi.org/10.1097/01.qco.0000200295.30285.13 [ Links ]
7. Bernstein W, Little R, Wilson W, et al. Acquired Immunodeficiency Syndrome-Related Malignancies in the Era of Highly Active Antiretroviral Therapy. International Journal of Hematology. 2006;84(1):3-11. https://doi.org/10.1532/IJH97.06088 [ Links ]
8. Simard EP, Pfeiffer RM, Engels EA. Cumulative incidence of cancer among individuals with acquired immunodeficiency syndrome in the United States. Cancer. 2011;117(5):1089-1096. https://doi/10.1002/cncr.25547 [ Links ]
9. Burgi A, Brodine S, Wegner S, et al. Incidence and risk factors for the occurrence of non-AIDS-defining cancers among human immunodeficiency virus-infected individuals. Cancer 2005;104(7):1505-1511. https://doi/10.1002/cncr.21334 [ Links ]
10. Anderson JH, Morran CG, Anderson JR, et al. Acute pancreatitis and non-Hodgkin's lymphoma. Postgraduate Medical Journal. 1987;63(736):137-139. https://doi.org/10.1136/pgmj.63.736.137 [ Links ]
11. Anderson F, Thomson SR. Pancreatitis in a high HIV prevalence environment. South African Medical Journal. 2017; 107(8):706-709. https://doi.org/10.7196/samj.2017.v107i8.10296. [ Links ]
12. Anderson F, Madiba TE, Thomson SR. Prognosis in acute pancreatitis associated with HIV infection. HPB. 2022; 24(11):1989-1993. https://doi.org/10.1016/j.hpb.2022.06.010 [ Links ]
13. Krishna SG, Kamboj AK, Hart PA, et al. The Changing Epidemiology of Acute Pancreatitis Hospitalizations. Pancreas. 2017;46(4):482-488. https://doi.org/10.1097/MPA.0000000000000783 [ Links ]
14. Kohler H, Lankisch PG. Acute Pancreatitis and Hyperamylasaemia in Pancreatic Carcinoma1. Pancreas. 1987;2(1):117-9. https://doi.org/10.1097/00006676-198701000-00018 [ Links ]
15. Lin A. Pancreatic Carcinoma as a Cause of Unexplained Pancreatitis: Report of Ten Cases. Annals of Internal Medicine. 1990;113(2):166. https://doi/10.7326/0003-4819-113-2-166 [ Links ]
16. Grimison PS, Chin MT, Harrison ML, et al. Primary pancreatic lymphoma - pancreatic tumours that are potentially curable without resection, a retrospective review of four cases. BMC Cancer. 2006;6(1):117. https://doi.org/10.1186/1471-2407-6-117 [ Links ]
17. Nayer H, Weir EG, Sheth S, et al. Primary pancreatic lymphomas: a cytolpathologic analysis of a rare malignancy. Cancer. 2004;102(5):315-321. https://doi/10.1002/cncr.20488 [ Links ]
18. Behrns KE, Sarr MG, Strickler JG. Pancreatic Lymphoma: Is It a Surgical Disease? Pancreas. 1994 Sep 1;9(5):662-7. PMID: 7809023 [ Links ]
19 . Loots E, Anderson FF, R Thomson FS, Eng F. Primary pancreatic lymphoma in an HIV patient: Dilemmas in diagnosis and management. South African Journal of Surgery. 2008 Feb;46(1):28-9. PMID: 18468421 [ Links ]
20. Facchinelli D, Boninsegna E, Visco C, et al. Primary Pancreatic Lymphoma: Recommendations for Diagnosis and Management. Journal of Blood Medicine. 2021;12:257-267. https://doi.org/10.2147/JBM.S273095 [ Links ]
21. Jones WF, Sheikh MY, McClave SA. AIDS-related non-Hodgkin's lymphoma of the pancreas. American Journal of Gastroenterology. 1997:92(2);335-338. PMID: 9040219 [ Links ]
22. Gramolelli S, Schulz TF. The role of Kaposi sarcoma-associated herpesvirus in the pathogenesis of Kaposi sarcoma. The Journal of Pathology. 2015;235(2):368-380. https://doi/10.1002/path.4441 [ Links ]
23. Chalya PL, Mbunda F, Rambau PF, et al. Kaposi's sarcoma: a 10-year experience with 248 patients at a single tertiary care hospital in Tanzania. BMC Research Notes. 2015;8(1):440. https://doi.org/10.1186/s13104-015-1348-9 [ Links ]
 Correspondence:
Correspondence:
email: fmadela@gmail.com


{kind=link}