










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.61 no.3 Cape Town 2023
http://dx.doi.org/10.36303/sajs.3998
CASE REPORT
Trans-anal small bowel evisceration in a patient with a perforated rectal prolapse
HJ LeeI; D HendricksI; T RangakaI, II; A Abd ElrahmanI, II
IDepartment of General Surgery, Klerksdorp-Tshepong Hospital Complex, South Africa
IIDepartment of Surgery, Faculty of Health Sciences, University of the Witwatersrand
SUMMARY
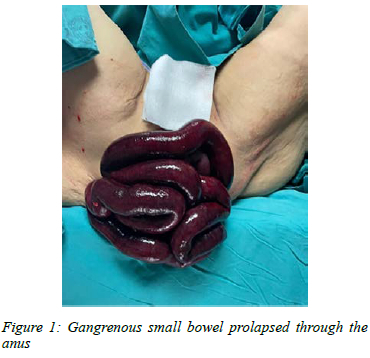
An 85-year-old lady with a history of chronic constipation presented with gangrenous small bowel protruding from the anus through a hole in a prolapsed rectum. At surgery, a resection of 125 cm of gangrenous small bowel was performed in the perineum prior to laparotomy, where rectal repair was followed by the creation of a sigmoid loop colostomy and double-barrel ileostomy. This avoided an intrabdominal anastomosis which was felt likely to complicate due to the lady's intraoperative haemodynamic instability requiring inotropic support. This tailored management of a trans-anal small bowel evisceration through a rectal prolapse resulted in recovery and a patient who was content with her stomas and preferred to live with them rather than have continuity restored.
Keywords: small bowel evisceration, rectal prolapse
Case report
An 85-year-old female with chronic constipation presented to the emergency department with prolapsed loops of bowel through the anus. She reported having taken laxatives in the evening prior to presentation. The patient noticed the prolapse after an episode of strained defecation, soon after which she developed severe abdominal pain. She had no prior history of recurrent rectal prolapse.
Six hours after symptom onset, she presented to the surgical department with a prolapsed gangrenous small bowel through the anus (Figure 1). She was pale with a pulse rate of 92 beats per minute, blood pressure of 231/ 118 mmHg and a respiratory rate of 20 breaths per minute. The patient was resuscitated, and the bowel covered in warm saline-soaked gauze.
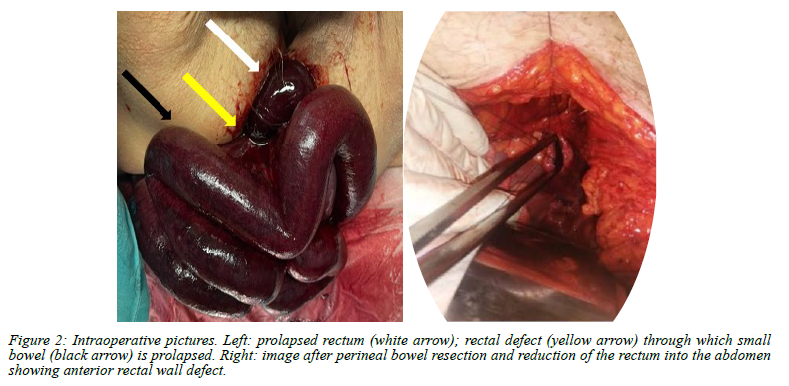
An emergency exploratory laparotomy was carried out by a lower midline incision under general anaesthesia. A 125 cm section of gangrenous small bowel was herniating through a 5 cm anterior rectal wall defect (Figure 2) at the level of the mid-rectum, which was prolapsed. A redundant sigmoid colon was noted with multiple diverticula that were full of hard faeces. The unhealthy small bowel was resected in the perineum. The mesentery was then reduced. After hot moist packaging and oxygenation, the prolapsed rectum, which was dusky and oedematous, became pink. The rectum was subsequently reduced and having closed the hole in the anterior wall was fixed to the sacral promontory and lateral abdominal wall. A sigmoid loop colostomy was performed because the colon was full of faeces and the small bowel was taken out as a double-barrel ileostomy. An anastomosis was opted against as the patient required intraoperative inotropic support.
The patient was sent to the intensive care unit for supportive care and subsequently discharged to the general ward on day two post-operation. The stoma was functional and oral feeds were started. She tolerated the ileostomy drainage well and was discharged home on day 8 post-operation. She was seen in the surgical outpatient clinic at six and eleven weeks post-operation and ileostomy reversal was discussed. However, at both visits, she refused any further intervention.
Discussion
Trans-anal evisceration of the small bowel is a rare surgical condition. Since its first description in 1827 by Brodie,1 very few cases have been reported. Most of these cases have been noted to occur in the presence of a spontaneous rupture of the rectum for which risk factors include chronic constipation, colonic or rectal malignancy and diverticular disease.2 An accompanying rectal prolapse is a common finding.3 The condition is precipitated by manoeuvres that increase intra-abdominal pressure such as coughing, vomiting, or straining while defecating.4 The reported case was an elderly lady with chronic constipation and the repeated straining resulted in rectal prolapse which was complicated by perforation and evisceration.
The primary mechanism thought to underlie this is a sliding hernia in which the Pouch of Douglas, with its visceral contents, acts as a hernial sac. With the invagination of the sac into the anterior wall of the rectum, there is subsequent ischaemia and weakening of the wall, increasing the likelihood of a rectal perforation. The perforation then allows the visceral contents, in this case the small bowel, to herniate and eviscerate through the anus.5
Reduction of the eviscerated small bowel through the anus without laparotomy is associated with high failure rate and increased mortality.6 The surgical treatment in such conditions involves resection of the gangrenous bowel, repair of the rectal perforation, rectopexy to reduce recurrence and a proximal stoma. In most reported cases and reviews,2'3,6 the gangrenous small bowel was reduced and resected depending on the viability. Primary anastomosis was done and accompanied by rectal tear repair and proximal colostomy. In some cases, a Hartmann's procedure was performed with acceptable success rates. The most similar management to that used in our case was reported in a 4-month-old child who had a resected gangrenous small bowel with exteriorisation of the two ends of the small bowel. 7 Our case had double barrel ileostomy as her age and intraoperative instability were considered too unfavourable for a primary small bowel anastomosis. Her survival attests to the safety of this approach as did her decision to cope with her stomas rather than to have continuity restored.
Acknowledgements
We would like to acknowledge the help of the Tshepong Hospital Records Department.
Conflict of interest
The authors declare no conflict of interest.
Funding source
No funding was required.
Ethical approval
Ethical approval was obtained by the University of the Witwatersrand Human Research Ethics Committee (reference number M220684).
ORCID
HJ Lee https://orcid.org/0000-0003-4268-2727
D Hendricks https://orcid.org/0000-0002-8829-0430
A Abd Elrahman https://orcid.org/0000-0002-9297-7120
References
1. Brodie BC. A case of a singular variety of hernia treated at St. George's Hospital. Lond Med Phys J. 1827;57:529-30. https://doi.org/10.1016/S0140-6736(02)81477-5. [ Links ]
2. Daniel EW, Thomas HD. Spontaneous rupture of the distal colon with evisceration of small intestine through anus: report of two cases and review of literature. Dis Colon Rectum. 1979;22:569-72. https://doi.org/10.1007/BF02587009. [ Links ]
3. Morris A, Setty S, Standage B, Hansen P. Acute trans-anal evisceration of the small bowel. Report of a case and review of the literature. Dis Colon Rectum. 2003;46:1280-3. https://doi.org/10.1007/s10350-004-6727-6. [ Links ]
4. Jeong J, Park JS, Byun CG, et al. Rupture of the rectosigmoid colon with evisceration of the small bowel through the anus. Yonsei Med J. 2000;41:289-92. https://doi.org/10.3349/ymj.2000.41.2.289. [ Links ]
5. Broden B, Snellman B. Procidentia of rectum studied with cineradiography: a contribution of causative mechanism. Dis Colon Rectum. 1968;11:330-47. https://doi.org/10.1007/BF02616986. [ Links ]
6. Berwin JT, Ho TK, D'Souza R. Small bowel evisceration through the anus - report of a case and review of literature. BMJ Case Rep. 2012;2012:bcr1220115316. https://doi.org/10.1136/bcr.12.2011.5316. [ Links ]
7. Sengar M, Neogi S, Mohta A. Prolapse of the rectum associated with spontaneous rupture of the distal colon and evisceration of the small intestine through the anus in an infant. J Pediatr Surg. 2008;43:2291-2. https://doi.org/10.1016/j.jpedsurg.2008.09.003. [ Links ]
 Correspondence:
Correspondence:
HJ Lee
Email: john6lee25@gmail.com


{kind=link}