










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.61 n.2 Cape Town 2023
http://dx.doi.org/10.36303/SAJS.3945
CASE REPORT
The vagaries of diagnosis and management of traumatic lumbar artery pseudoaneurysm
VC Ntola; SKS Ntloko
Department of General Surgery, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, South Africa
SUMMARY
This report details a patient who sustained a posterior stab to a lumbar artery. The diagnosis was challenging and could have been easily missed if a high index of suspicion were not maintained. In a trauma context, this injury is missed due to focus on other concomitant injuries. We discuss the merits of computed tomography angiography (CTA) to identify the arterial blush which led to onward referral for successful catheter-directed arterial embolotherapy.
Keywords: lumbar artery, lumbar artery injury, lumbar artery pseudoaneurysm, endovascular coil
Case presentation
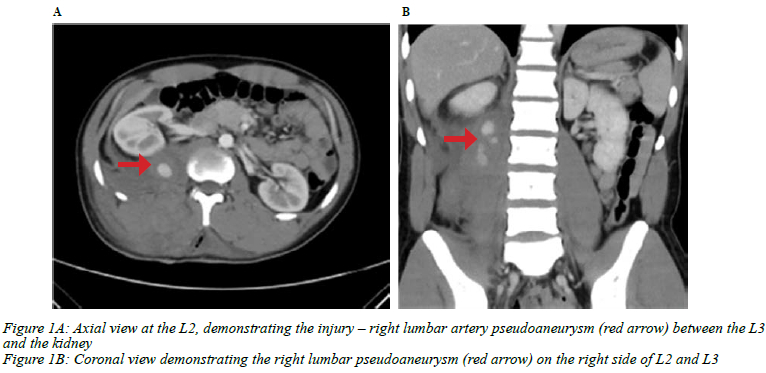
A 26-year-old male was stabbed in the back with a knife about 10 hours prior to presentation at base hospital. The medical and surgical history was unremarkable. On arrival he had a blood pressure (BP) of 91/51 mmHg, a pulse of 132 beats per minute (bpm) and a haemoglobin (Hb) of 7.8 g/dl. He responded to resuscitation with intravenous fluids and blood transfusion. He had a deep wound at the back on the right side of the midline at L2. Presence of free peritoneal blood was excluded with a transabdominal ultrasound. In view of his unstable initial presentation, he had a computed tomography angiography (CTA) that showed the right lumbar artery pseudoaneurysm, shown in Figures 1A and B.
Based on the CTA findings, he was transferred to the vascular unit at Inkosi Albert Luthuli Central Hospital (IALCH) for endovascular intervention. On arrival he had stabilised with a BP of 143/76 mmHg, a pulse of 99 bpm and oxygen saturation 100% on room air. His Hb was 8.3 g/dl, with normal urea and electrolytes.
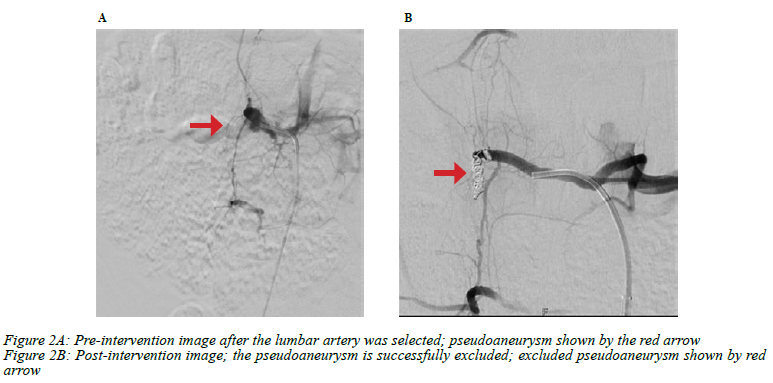
In the supine position under general anaesthesia, a right transfemoral artery approach was used for access. An 18-gauge needle was used to puncture the right groin via ultrasound guidance and using a Seldinger technique a pigtail catheter was inserted into the aorta. The powered angiogram was done through the pigtail. The images were not clear to identify the lumbar branches. Subsequently, a lumbar branch was selected just below the right renal artery and showed a right-sided pseudoaneurysm at the level of L2 and L3 (Figure 2A). This was super selected and coil embolised, distal to the pseudoaneurysm, into the sac and proximal, with 3 Nester coils: 1(4x7 mm) and 2(3x7 mm). Post-intervention image (Figure 2B) showed that the pseudoaneurysm was successfully excluded and the procedure was concluded.
Post procedure there was a pulse on the access site and the distal pulses were palpable. There was no evidence of bleeding on the stab site. Two days post intervention, the patient was discharged. A month later, he was well, and a surveillance CTA showed no evidence of pseudoaneurysm. He was discharged from further follow-up.
Discussion
Penetrating wounds in the posterior abdomen are known to cause injuries to the retroperitoneal structures, particularly the colon and kidney and less commonly the vascular structures. These injuries may be occult, requiring a high index of suspicion to be detected.1 Lumbar artery injury may result from blunt or penetrating trauma. In rare cases, the injury may be due to surgical procedures such as spinal surgery or renal biopsy.2 Frequently, the initial injury to the lumbar artery is missed and manifests as an expanding pseudoaneurysm in the retroperitoneum whose location results in an absence of symptoms and signs until it enlarges and ruptures.3-5 We would like to highlight that the doctors at the base hospital carried out the most appropriate investigation, a CTA. This investigative pathway was based on the patient's initial presentation with shock, in the absence of free intraperitoneal fluid on ultrasound, which created a high index of suspicion that a vascular injury needed to be excluded. Had they after stabilisation only observed the patient for 24 hours and discharged him, the lumbar artery pseudoaneurysm would have been missed with a potentially lethal outcome. This difficulty in diagnosis is well described by Udobi and Childs who reported, on similar injury to the one described here, a delayed diagnosis 14 days post discharge in a patient who had a concomitant caecal injury. Lumbar embolisation was performed first, followed by laparotomy to address the caecal injury.6 This report highlights the challenge in managing these injuries when there is a concomitant intra-abdominal injury, and one must decide whether to address the intra-abdominal injuries or the lumbar artery injury first. If the lumbar artery is bleeding, that injury should be addressed first by endovascular intervention avoiding concomitant exploratory laparotomy and retroperitoneal exploration.7
Approaching these injuries via retroperitoneal exploration at open surgery is challenging as identifying and controlling the source of bleeding is very difficult due to the many collaterals supplying this region and the posterolateral origin of the lumbar arteries from the aorta. This also pertains to angiographic control when it is extremely important to selectively evaluate nearby vessels above and below an injured lumbar artery.8 This is due to a high probability of multiple injuries from the initial trauma and the need to prevent collateral retrograde supply to the proximally embolised lumbar.5 These variations include intercostal artery supply of the 1st lumbar artery and collaterals from iliac vessels supplying the inferior lumbar artery. Of even greater importance is avoidance of embolisation of the artery of Adamkiewicz that arises from posterior intercostal artery or the 1st or 2nd lumbar artery and may result in spinal cord infarction and paralysis. Identification of the presence of this vessel and embolising the injured lumbar artery as distal as possible is crucial to avoid anterior spinal cord infarction.9,10 The problematic control of bleeding at open surgery and the complexity of the anatomy have resulted in endovascular embolotherapy being the preferred treatment.10
After lumbar artery embolisation, creatinine kinase and potassium levels should be assessed to diagnose lumbar muscles infarction and rhabdomyolysis that can lead to renal failure.10
This report highlights the value of CTA in the scenario of shock from a retroperitoneal injury in the absence of free fluid in the abdomen to exclude or diagnose a vascular injury in retroperitoneum. This is particularly true for referring hospitals who do not have interventional angiography facilities or expertise on site. This allows for a timely transfer to an institution which can carry out advanced embolotherapy to definitively treat the injury and avoid the challenges and morbidity of open surgery.
Conflict of interest
The authors declare no conflict of interest.
Funding source
No funding source to be declared.
Ethical approval
The author/s declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010.
Prior to commencement of the study ethical approval was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee: BREC/00003897/2022.
ORCID
VC Ntola https://orcid.org/0000-0002-9667-1591
SKS Ntloko https://orcid.org/0000-0001-5048-2114
REFERENCES
1. Kong VY, Oosthuizen GV, Clarke DL. The spectrum of injuries resulting from posterior abdominal stab wounds: a South African experience. Ann R Coll Surg Engl. 2015;97(4):269-73. https://doi.org/10.1308/003588415X14181254789204. [ Links ]
2. Santillan A, Patsalides A, Gobin YP. Endovascular embolisation of iatrogenic lumbar artery pseudoaneurysm following extreme lateral interbody fusion (XLIF). Vasc Endovasc Surg. 2010;44(7):601-3. https://doi.org/10.1177/1538574410374655. [ Links ]
3. Hamid RS, Chishti I, Azeemuddin M. Post traumatic avulsion of lumbar artery: a rare cause of retroperitoneal haemorrhage treated by glue embolisation. J Pak Med Assoc. 2010;60(6):487. [ Links ]
4. Kessel BJ, Habib FA, Thompson B, Bayajo DE, Shatz D. Lumbar artery pseudoaneurysm. Eur J Trauma. 2004;30(3):187-90. https://doi.org/10.1007/s00068-004-1348-2. [ Links ]
5. Marty B, Sanchez LA, Wain RA, et al. Endovascular treatment of a ruptured lumbar artery aneurysm: case report and review of the literature. Ann Vasc Surg. 1998;12(4):379-83. https://doi.org/10.1007/s100169900172. [ Links ]
6. Udobi KF, Childs EW. Traumatic lumbar artery pseudo-aneurysm presenting with massive lower gastrointestinal tract bleeding. J Trauma Acute Care Surg. 2003;55(1):154-7. https://doi.org/10.1097/01.TA.0000079008.05677.90. [ Links ]
7. Yuan K-C, Hsu Y-P, Wong Y-C, et al. Management of complicated lumbar artery injury after blunt trauma. Ann Emerg Med. 2011;58(6):531-5. https://doi.org/10.1016/j.annemergmed.2011.07.002. [ Links ]
8. Sofocleous CT, Hinrichs CR, Hubbi B, et al. Embolisation of isolated lumbar artery injuries in trauma patients. Cardiovasc Interv Radiol. 2005;28(6):730-5. https://doi.org/10.1007/s00270-003-0117-7. [ Links ]
9. Doppman JL, Di Chiro G. Paraspinal muscle infarction. A painful complication of lumbar artery embolisation associated with pathognomonic radiographic and laboratory findings. Radiology. 1976;119(3):609-13. https://doi.org/10.1148/119.3.609. [ Links ]
10. Ceyhan M, Belet Ü, Aslan S, et al. Traumatic lumbar artery pseudoaneurysm: the role of CT angiography in diagnosis and treatment. Diagn Interv Radiol. 2010;16(2):162-4. https://doi.org/10.4261/1305-3825.dir.1925-08.2. [ Links ]
 Correspondence:
Correspondence:
VC Ntola
Email: vuyolwe@yahoo.com


{kind=link}
{kind=link}