










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.61 no.2 Cape Town 2023
http://dx.doi.org/10.36303/SAJS.3851
GENERAL SURGERY
Adult corrosive ingestions in the Pietermaritzburg Metropolitan Surgical Service
AN Mthethwa; M Govender; DL Clarke
Department of Surgery, University of KwaZulu-Natal, South Africa
ABSTRACT
BACKGROUND: There is a paucity of data around corrosive ingestion in South Africa over the last three decades. As such, we set out to review our experience with adult corrosive ingestion in our tertiary gastrointestinal surgical service
METHODS: A retrospective, quantitative review was performed. The parameters analysed were demographics, substance ingestion, ingestion time to first presentation to a healthcare facility, clinical presentation, severity of injury based on endoscopic classification, computed tomography (CT) findings, management and outcomes. Patients presenting within 72 hours with alarm symptoms underwent flexible upper endoscopy and injury severity grading. In patients presenting after 72 hours, a water-soluble contrast study was obtained prior to upper endoscopy. Patients with signs of sepsis, surgical emphysema or physiological instability were referred for urgent CT to exclude oesophageal perforation and mediastinitis
RESULTS: Between January 2012 and January 2019, a total of 64 patients presented with a history of corrosive ingestion - 40 (31%) were males and 24 (19%) females. The average time from ingestion to presentation was 72 hours. In 78% of patients, the agents were intentionally ingested, whilst 22% claimed accidental ingestion. A quarter of the patients (21%) presented to the unit clinically unstable, requiring emergent cardiorespiratory support. Eight (12%) patients required urgent surgical intervention due to the extent of injury. Nine (14%) patients demised during the acute admission. Of this group, three patients had undergone surgical intervention, and six were managed conservatively. Eighty-five per cent of all patients survived their initial admission
CONCLUSION: This paper has highlighted the problem of corrosive ingestion in our setting. It remains a complicated problem to manage associated with significant morbidity and mortality rates. The current trend in the assessment of these patients is increased use of CT scan to assess the extent of transmural necrosis. Our algorithms should change to reflect this contemporary approach
Keywords: corrosive ingestion, Zargar classification, endoscopy
Introduction
The dramatic social changes in the first two decades of the new millennium have produced significant social stressors which enable and contribute to mental illness. Self-harm has emerged as a major problem globally, in both high-income countries (HIC) and low- and middle-income countries (LMICs).1 Self-harm places a significant burden on acute care surgical and trauma services. South Africa is an upper middle-income country with major discrepancies in wealth and access to health care.2 There is evidence which suggests that mental illness and self-harm are increasing in South Africa. Numerous mechanisms are associated with self-harm, including firearm-related injuries, hanging, jumping from heights, self-poisoning and the ingestion of corrosive substances.3 Corrosive ingestion may result in complex injuries to the upper gastrointestinal tract which necessitate prolonged and complex surgical procedures and interventions. Little has been written about corrosive ingestion in South Africa over the last three decades. The literature has mostly focused on the paediatric group.4-7 However, corrosive ingestion in adults is rising in South Africa, particularly in the indigent population. In light of this, we set out to review our experience with adult corrosive ingestion in our tertiary gastrointestinal surgical service. It was hoped that this would reignite multidisciplinary interest in this area and help us refine our algorithms to ensure that they are contemporary and appropriate.
Clinical setting
Greys Hospital is a tertiary level hospital situated in Pietermaritzburg, in KwaZulu-Natal (KZN) Province, South Africa. The hospital services the city of Pietermaritzburg and the western part of KZN. This is a largely rural area and has a population of around three million people. There are 19 district hospitals and three regional hospitals in the area. Health districts in KZN score poorly in various poverty indices.2,8,9
Management of corrosive injuries
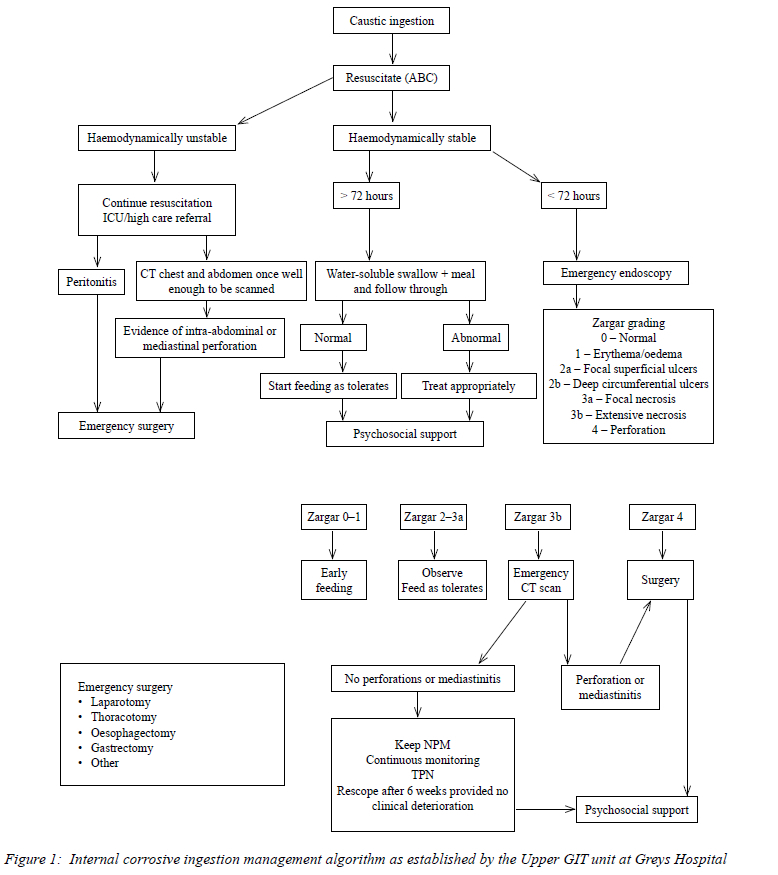
All patients who present to Greys Hospital with an acute history of corrosive ingestion were resuscitated and managed under the direction of the upper gastrointestinal surgery subspecialist team, according to their internal algorithm (Figure 1). Patients presenting within 72 hours undergo flexible upper endoscopy and the severity of the injury is graded according to the Zargar classification.10 In those who present with signs of sepsis, surgical emphysema or physiological instability, urgent contrast enhanced computed tomography (CT) scan is obtained to exclude oesophageal perforation and mediastinitis, as well as to assess the extent of the mural necrosis. The CT grading system described by Hoffmann and colleagues is used to grade the severity of the caustic ingestion.13 If patients present after 72 hours, a water-soluble oral contrast study is obtained. The rationale is to limit the risk of oesophageal perforation from flexible endoscopy due to the highly friable mucosa in the acute phase of corrosive ingestions.
Methods
The initial data source was the hybrid electronic medical registry (HEMR) which has been maintained at Grey's Hospital since 2012. All surgical admissions have been recorded in this registry since 2012 and the data is quality checked by the staff of the department on a regular basis. The HEMR has been validated repeatedly over the last decade.11,12
All patients with a primary diagnosis of corrosive ingestion who presented acutely between January 2012 to January 2019 were included. The time frame for the acute admission period was from date of corrosive ingestion up to two weeks post ingestion. Repeat admissions and patients with complications from previous corrosive injuries were not included in this review. Data obtained for the study included admission entries, discharge entries, operative notes and imaging and endoscopy reports during the period assessed. A retrospective, quantitative review was performed. The following parameters were analysed - demographics, substance ingested, reason for ingestion (deliberate or accidental), time from ingestion to first presentation to a healthcare facility, severity of injury based on endoscopic classification and CT findings, management algorithm inclusive of surgical and non-surgical intervention, type of surgical intervention received as well as inpatient outcomes including mortality. The data captured were tabulated and depicted graphically.
Results
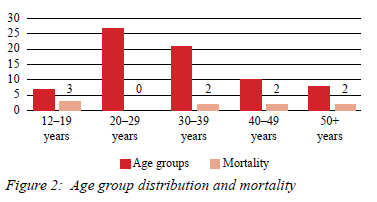
Between the period of January 2012 to January 2019, 64 patients presented with a history of corrosive ingestion. There were 40 (62%) males and 24 (37%) females. The average age was 27 (Figure 2). Seventy-eight per cent (50) of patients ingested the agents intentionally; in the remainder, the ingestion was accidental. Alkali household agents were the most common ingested substance. Forty-one patients ingested an alkali substance, 18 ingested an acidic substance and in five patients, the nature of the ingested substance was unclear.
The average time from ingestion to presentation to Grey's Hospital was between nine to 72 hours. Twenty-one per cent (14) of patients required resuscitation on arrival. Seven had respiratory compromise with three requiring endotracheal intubation, four patients had a metabolic acidosis and two had an acute kidney injury. Four patients were hypotensive on presentation, but responsive to resuscitative efforts and three patients arrived in septic shock.
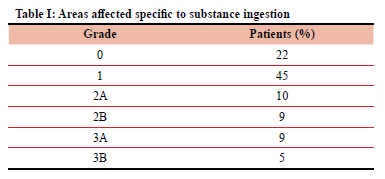
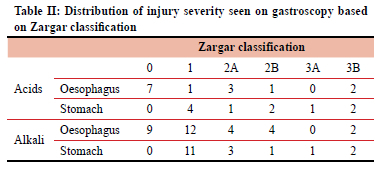
Fifty-one patients underwent flexible upper endoscopy as they presented within 72 hours of whom five had CT scans as they had higher grade injuries based on the Zargar classification on flexible endoscopy. Table I demonstrates the distribution of injury identified on flexible upper endoscopy based on the Zargar classification. A CT grading system was employed to estimate injury severity in those patients who underwent a CT scan.13 Sixteen water-soluble contrast studies were done for patients who presented after 72 hours. Table II depicts the distribution of injury, the substance ingested and findings on gastroscopy as per the Zargar classification grading.
Surgery
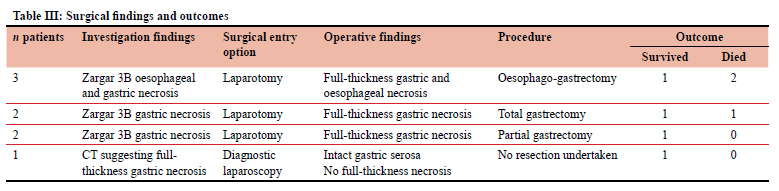
Eight patients (12%) proceeded to urgent surgery. The findings and type of surgery performed are documented in Table III. All patients went to the intensive care unit (ICU) postoperatively for ongoing physiological support.
Outcomes
Eighty-five per cent (55) of patients survived their index admission, with an inpatient average stay of three to five days. Nine patients (14%) died - all these patients presented with a metabolic acidosis and leucocytosis of varying severity. Two of these patients were palliated due to instability for surgical intervention in light of a failed response to resuscitative physiological support. Four patients died with endoscopic or CT findings not indicative for surgical intervention. Three died post-surgery in ICU, due to overwhelming physiological derangement.
Discussion
Corrosive ingestion is not an uncommon form of self-harm in our environment, and between 2012 and 2019, Grey's Hospital treated an average of nine new patients annually. Our study demonstrated that corrosive ingestion has a high mortality rate (14%) in the acute phase. In other series, it is reported that survivors face significant long-term morbidity and repeated endoscopic management or complex reconstructive surgery.14 Hall et al.1 noted that the commonest ingested substance was acidic, whereas in our series, alkali agents were more common.15 In addition, whilst a recent retrospective review from North America found that the vast majority of corrosive ingestions (83.8%) were accidental and only 16.2% had suicidal intention, in our setting this ratio is the exact inverse with most cases being deliberate and intentional.15,16 In our environment household cleaning agents, which are alkali in nature, were the most commonly used agent. This explains the anatomical distribution of the injuries in our series as the oesophageal mucosa is more susceptible to alkali agents. The alkali group therefore had a higher-grade oesophageal injury than the acid ingestion group, a finding corroborated in the literature.17 In addition, there was a much higher grade of injury at the oesophageal and pyloric sphincters, as these structures delay transit resulting in pooling of the ingested substance, so increasing the exposure of the mucosa in these areas to the ingested substance. Overall, alkali agents tended to have a more diffuse impact on the entire upper gastrointestinal tract, albeit with many areas of low-grade involvement, as depicted graphically in Tables I and II. With acid ingestion, the distribution of injury was predominantly the gastric mucosa. Similar findings have been reported in the literature.14,18 As in this series, the literature suggests that both mortality and morbidity are higher in the alkali ingestion group.17
The acute management of patients with a corrosive ingestion, involves resuscitation and stabilisation followed by aggressive investigation.15 A subset of patients with high-grade injuries will need urgent surgery. In our series, eight patients were offered surgical intervention as part of their treatment protocol, as they presented with signs of sepsis or imaging demonstrating full-thickness necrosis. A retrospective study published by Javed et al. demonstrated similar findings.20 Patients not requiring surgery will require supportive therapy followed by long-term management which may involve both endoscopic and surgical procedures.16,20-22
Flexible endoscopy is a safe, reliable tool for diagnosing and prognosticating corrosive injuries and gentle endoscopic parameters must be endeavoured in experienced hands. Fifty-two patients in this study underwent flexible endoscopy on presentation to our centre within 72 hours post ingestion, as it was the investigation of choice, relying mainly on the assistance of the Zargar classification to delineate the most appropriate treatment for these patients. However, there has been a change in the assessment of patients with acute corrosive ingestion away from flexible upper endoscopy, towards the use of CT scan. Modern CT scan avoids the small but well-described risk of iatrogenic perforation associated with flexible upper endoscopy and can assess the extent of trans mural necrosis. It is the investigation of choice in patients with marked physiological derangement, suspected mediastinitis or transmural necrosis as it outperforms flexible upper endoscopy. The more recent guidelines advocate a much greater role for CT scan in the assessment of corrosive injuries.15 This has precipitated a review of our clinical algorithm for the assessment and management of these patients, in order to align them more closely with current guidelines and recommendations.
In our study, there was a high mortality rate (14%) associated with corrosive ingestion, and similar to literature reports, we found that the severity of injury corresponds to outcome.23-25 Mortality in the patients with endoscopically lower-grade injuries occurred in those who presented with multi-organ failure, possibly from other toxic substances ingested at the same time, and who did not respond to resuscitation.
Patients who underwent operative intervention had endoscopic or CT findings suggestive of full-thickness necrosis, or presented clinically with signs of sepsis and surgical emphysema. In principle, acute surgery for corrosive ingestion involves resection of the injured segment followed by wide drainage and establishment of a route for enteral nutrition. Primary anastomosis is suggested in the physiologically stable patient. Patients who cannot withstand ongoing surgical intervention at the index surgery may require an oesophagostomy with a feeding jejunostomy as a temporary enteral feeding portal.
This audit has identified areas for potential improvement of our clinical algorithms. Flexible upper endoscopy allows for grading of the mucosal injury according to the Zargar classification and is an essential part of the assessment of these patients. The limitation of flexible endoscopy is that it does not allow for assessment of the transmural injury and is invasive.
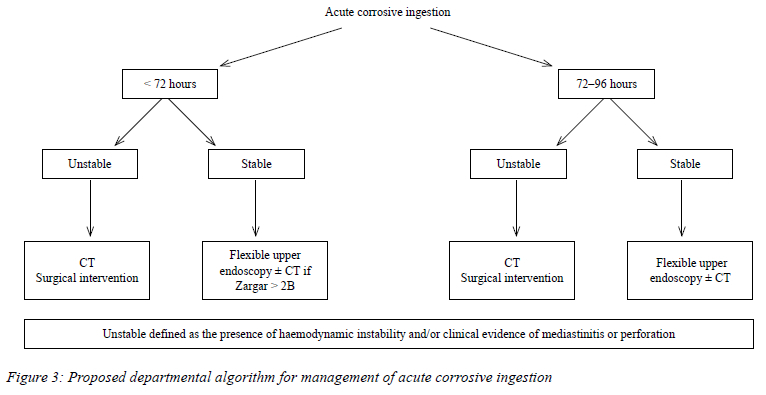
Modern cross-sectional CT scan has become more important in the assessment of these patients. Our algorithm for patients presenting with corrosive ingestion is evolving, and currently we feel that the use of CT and not a water-soluble contrast study, should be the next investigation after flexible endoscopy which can usually be performed up to 96 hours post ingestion.15 The proposed updated internal algorithm is shown in Figure 3.
Study limitations
This study is a retrospective review of prospectively collected data and as such shares many of the limitations inherent to a retrospective audit.
This audit has not provided insight into why there is a specific inclination to ingest corrosive agents for suicidal purposes in some cultures. Further research is strongly recommended.
The aim of this audit was to identify and assess the outcomes of our cohort in the acute setting, further research will be required to assess this group of patients for long-term complications.
Conclusion
This paper has provided insight into the problem of corrosive ingestion in our setting and how, in contrast to high-resource settings, ingestion is predominantly deliberate rather than accidental. This suggests social and mental health care issues not addressed in this report that require further investigation. The current trend in the assessment of these patients is towards the increased use of CT scan to assess the extent of transmural necrosis. Our revised algorithm reflects this contemporary approach.
Acknowledgements
Mr Vishendran Govindasamy, Ms Wanda Bekker and Mr John Bruce for assisting with data collection for the review.
Conflict of interest
The authors declare no conflict of interest.
Funding source
No funding was required.
Ethical approval
Ethical approval was obtained from the Biomedical Research Ethics Committee (BREC) based at the University of KwaZulu-Natal (BE221/13 and BE207/09).
ORCID
M Govender https://orcid.org/0000-0002-4066-0156
DL Clark https://orcid.org/0000-0002-8467-1455
REFERENCES
1. Hall AH, Jacquemin D, Henny D, et al. Corrosive substances ingestion: a review. Crit Rev Toxicol. 2019;49(8):637-69. https://doi.org/10.1080/10408444.2019.1707773. [ Links ]
2. Provincial Government. Province of KwaZulu-Natal SocioEconomic Review and Outlook. 2019/2020. p. 22-23. [ Links ]
3. Moffatt SE, Kong VY, Weale RD, et al. The spectrum of self-inflicted injuries managed at a major trauma centre in South Africa. Trauma Surg. 2019;57(2):65-69. [ Links ]
4. Arnold M, Numanoglu A. Caustic ingestion in children - a review. Sem Pediatr Surg. 2017;26(2):95-104. https://doi.org/10.1053/j.sempedsurg.2017.02.002. [ Links ]
5. Millar AJW, Cox SG. Caustic injury of the oesophagus. Pediatr Surg Int. 2015;31(2):111-21. https://doi.org/10.1007/s00383-014-3642-3. [ Links ]
6. Van As AB, Du Toit N, Wallis L, et al. The South African experience with ingestion injury in children. Int J Pediatr Otorhinolaryngol. 2003;67(Suppl 1):S175-8. https://doi.org/10.1016/j.ijporl.2003.08.021. [ Links ]
7. Arévalo-Silva C, Eliashar R, Wohlgelernter J, Elidan J, Gross M. Ingestion of caustic substances: a 15-year experience. Laryngoscope. 2006;116(8):1422-6. https://doi.org/10.1097/01.mlg.0000225376.83670.4d. [ Links ]
8. William B. Overcoming poverty and inequality in South Africa. An assessment of drivers, constraints and opportunities. International Bank for Reconstruction and Development/The World Bank; 2018. p. 16-17. [ Links ]
9. Department of Statistics South Africa. Poverty in perspective statistics South Africa; mid-year 2020. [ Links ]
10. De Lusong MAA, Timbol ABG, Tuazon DJS. Management of oesophageal caustic injury. World J Gastrointest Pharmacol Ther. 2017;8(2):90-98. https://doi.org/10.4292/wjgpt.v8.i2.90. [ Links ]
11. Laing G, Bekker W, Bruce J, Clarke D. Reflections on the development of the Hybrid Electronic Medical Registry in Pietermaritzburg. S Afr J Surg. 2022;60(2):146-7. https://doi.org/10.17159/2078-5151/SAJS3919. [ Links ]
12. Laing GL, Bruce JL, Skinner DL, et al. Development, implementation, and evaluation of a hybrid electronic medical record system specifically designed for a developing world surgical service. World J Surg. 2014;38(6):1388-97. https://doi.org/10.1007/s00268-013-2438-2. [ Links ]
13. Hoffmann R, Burns M, Gosselin S. Ingestion of caustic substances. N Engl J Med. 2020;382:1739-48. https://doi.org/10.1056/NEJMra1810769. [ Links ]
14. Kamat R, Gupta P, Reddy YR, et al. Corrosive injuries of the upper gastrointestinal tract: a pictorial review of the imaging features. Indian J Radiol Imaging. 2019;29(1):6-13. https://doi.org/10.4103/ijri.IJRI_349_18. [ Links ]
15. Chirica M, Kelly MD, Siboni S, et al. Oesophageal emergencies: WSES guidelines. World J Emerg Surg. 2019;14:26. https://doi.org/10.1186/s13017-019-0245-2. [ Links ]
16. Acehan S, Satar S, Gulen M, Avci A. Evaluation of corrosive poisoning in adult patients. Am J Emerg Med. 2021;39:65-70. https://doi.org/10.1016/j.ajem.2020.01.016. [ Links ]
17. Hollenbach M, Tünnemann J, Struck MF, et al. Endoscopic findings and outcome in caustic ingestion of acidic and alkaline agents in adults: a retrospective analysis. Medicine (Baltimore). 2019;98(35):e16729. https://doi.org/10.1097/MD.0000000000016729. [ Links ]
18. Contini S, Scarpignato C. Caustic injury of the upper gastrointestinal tract: a comprehensive review. World J Gastroenterol. 2013;19(25):3918-30. https://doi.org/10.3748/wjg.v19.i25.3918. [ Links ]
19. Cheng HT, Cheng CL, Lin CH, et al. Caustic ingestion in adults: the role of endoscopic classification in predicting outcome. BMC Gastroenterol. 2008;8:31. https://doi.org/10.1186/1471-230X-8-31. [ Links ]
20. Javed A, Pal S, Krishnan EK, Sahni P, Chattopadhyay TK. Surgical management and outcomes of severe gastrointestinal injuries due to corrosive ingestion. World J Gastrointest Surg. 2012;4(5):121-5. https://doi.org/10.4240/wjgs.v4.i5.121. [ Links ]
21. Ducoudray R, Mariani A, Corte H, et al. The damage pattern to the gastrointestinal tract depends on the nature of the ingested caustic agent. World J Surg. 2016;40(7):1638-44. https://doi.org/10.1007/s00268-016-3466-5. [ Links ]
22. Methasate A, Lohsiriwat V. Role of endoscopy in caustic injury of the oesophagus. World J Gastrointest Endosc. 2018;10(10):274-82. https://doi.org/10.4253/wjge.v10.i10.274. [ Links ]
23. Hashmi M, Ali M, Ullah K, Aleem A, Khan IH. Clinico-epidemiological characteristics of corrosive ingestion: a cross-sectional study at a tertiary care hospital of Multan, South-Punjab Pakistan. Cureus. 2018;10(5):e2704. https://doi.org/10.7759/cureus.2704. [ Links ]
24. Kalayarasan R, Ananthakrishnan N, Kate V. Corrosive ingestion. Indian J Crit Care Med 2019;23(Suppl 4):S282-6. https://doi.org/10.5005/jp-journals-10071-23305. [ Links ]
25. Zargar SA, Kochhar R, Mehta S, Mehta SK. The role of fiberoptic endoscopy in the management of corrosive ingestion and modified endoscopic classification of burns. Gastrointest Endosc. 1991;37(2):165-9. https://doi.org/10.1016/S0016-5107(91)70678-0. [ Links ]
 Correspondence:
Correspondence:
AN Mthethwa
Email: bugz.any@gmail.com


{kind=link}
{kind=link}
{kind=link}