










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.61 no.2 Cape Town 2023
http://dx.doi.org/10.36303/SAJS.3857
GENERAL SURGERY
The utility of the bedside index of severity in acute pancreatitis at prognosticating adverse outcomes
TN MakofaneI; DL ClarkeI; F Anderson†,II; L FerndaleIII
IDepartment of Surgery, University of KwaZulu-Natal, South Africa
IIClinical Unit Surgical Gastroenterology, Inkosi Albert Luthuli Central Hospital, South Africa
IIIClinical Unit Surgical Gastroenterology, Grey's Hospital, University of KwaZulu-Natal, South Africa
ABSTRACT
BACKGROUND: Identification of at-risk patients with acute pancreatitis (AP) early on in the course of hospital admission remains a challenge. Early identification of these patients can facilitate early referral to tertiary hospitals with skilled multidisciplinary teams (MDTs) and high-dependency health care facilities. This study retrospectively reviewed the ability of the bedside index of severity in acute pancreatitis (BISAP) score and other biochemical markers to predict organ failure and mortality in acute pancreatitis
METHODS: All patients presenting to Grey's Hospital with AP between 2012 and 2020 were included in the study. The BISAP score and other biomarkers were evaluated at presentation in predicting organ failure (> 48 hours duration) and mortality
RESULTS: A total of 235 patients were included in the study. A total of 144 (61%) were male and 91 (39%) were female. Alcohol (81%) and gallstones (69%) were the commonest aetiological factors amongst males and females respectively. A total of 42 (29%) males and 10 (11%) females developed organ failure during their hospital stay. The mortality rate was 11.8% for males, 6.59% for females, with an overall mortality of 9.8%. A BISAP score of 2 had a sensitivity of 87.98% and specificity of 59.62% at predicting organ failure (positive predictive value [PPV] = 88.46%, negative predictive value [NPV] = 58.49%, 95% confidence interval [CI], p = 0.001). A BISAP score of 3 and above had a sensitivity of 98.11% and specificity of 69.57% at predicting mortality (PPV = 96.74%, NPV = 80%, 95% CI, p = 0.001). A multivariate analysis of biomarkers bicarbonate, base excess, lactate, urea and creatinine either failed to reach statistical significance or had specificity that is too low to prognosticate organ failure and mortality
CONCLUSION: The BISAP score has limitations at predicting organ failure, but it is a reliable tool for predicting mortality in AP. Due to its simplicity of use, it should be used in resource-constrained settings to triage at-risk patients in smaller hospitals, for early referral to tertiary hospitals
Keywords: acute pancreatitis, BISAP score, organ failure, mortality, biomarkers
Introduction
Acute pancreatitis (AP) is a common emergency condition. Whilst most incidents of AP are self-limiting, a subset of patients will develop severe AP. As the severity of pancreatitis increases, so does the morbidity, mortality and healthcare costs. In KwaZulu-Natal, AP carries a mortality risk of 5.7-9%.1,2 Most of the deaths occur within the first two weeks following admission. This contrasts with high-income countries where most deaths occur later than two weeks.2 Patients with severe AP are more likely to require intensive care unit (ICU) admission, organ support and surgery than patients with mild attacks.3 The clinical challenge is that this process evolves over time and severity may not always be apparent on admission.3 This is problematic as many patients present at district hospitals with limited capacity for organ support. A simple scoring system would be helpful to prioritise patients who may require early transfer for eventual organ support. Available prognostic scoring systems for AP, including the Ranson, Glasgow and acute physiology and chronic health evaluation II (APACHE-II) scores all have limitations.4 The bedside index of severity in acute pancreatitis (BISAP) score can be performed on admission. It includes blood urea nitrogen, the Glasgow coma scale, systemic inflammatory response syndrome (SIRS) criteria, age and the presence of a pleural effusion, which are all readily available at district hospitals.4 When the APACHE-II and BISAP scores were evaluated in the same patient cohort, they showed similar efficacy in predicting adverse outcomes.4 The aim of this study was to evaluate the ability of the BISAP score to identify patients at increased risk of prolonged organ failure and mortality in a patient that presented with AP to our institution.
Patients and methods
A retrospective chart review of all patients with AP who were prospectively entered into the hybrid electronic medical record (HEMR) database at Grey's Hospital, South Africa, between 14 December 2012 and 31 October 2020 were included. The following inclusion criteria were used:
i. A primary admission diagnosis of AP according to the revised Atlanta classification.3
ii. Patients 13 years and older transferred to Grey's Hospital from another healthcare institution less than 72 hours after being diagnosed with AP.
iii. Patients known with chronic pancreatitis with acute exacerbation as diagnosed by a lipase or amylase level three times the upper limit of normal, typical chronic pancreatitis pain, and/or radiological features of acute-on-chronic pancreatitis.
The following patients were excluded:
i. Patients with post endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis.
ii. Patients with incomplete data.
Admission clinical data, including parameters such as age, gender, length of hospital stay, live or deceased state upon discharge, lactate, PaO2, PCO2, standard bicarbonate (HCO3-), base excess (BE), urea, creatinine, haematocrit (HCT), red cell distribution width (RCDW) and white cell count (WCC) were transferred onto a dedicated Microsoft Excel spreadsheet for analysis. The BISAP score was retrospectively calculated. Organ failure was retrospectively determined by calculating the modified Marshall score at 48 hours after admission. A modified Marshall score of 2 or more at 48 hours was regarded as confirming the presence of prolonged organ failure.
The ability of the BISAP score at predicting organ failure and mortality at index admission for AP was calculated. A univariate analysis of RCDW, HCT, BE, HCO3-, lactate, urea and creatinine was performed to determine their ability to prognosticate both organ failure and mortality. The individual biomarkers that predicted outcomes with statistical significance were included in a multivariate analysis. These were then compared to the BISAP score's ability to predict the same outcomes.
Statistical analysis
Descriptive statistics were used to summarise the data for univariate and multivariate analysis. Categorical variables were presented as a number and continuous variables as a mean (standard deviation [SD]) and median (range). Two outcomes were classified, the first being live versus deceased discharges, and the second being the presence of prolonged organ failure beyond 48 hours or not. Comparisons of the BISAP score and other biochemical markers by outcome were done using chi-square and Fisher's exact tests. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and p-values of the respective variables at predicting the outcomes were reported. The Mann-Whitney U-test was used to compare continuous variables. The data was analysed in Stata Standard Edition version 17. A p-value < 0.05 was considered statistically significant.
Results
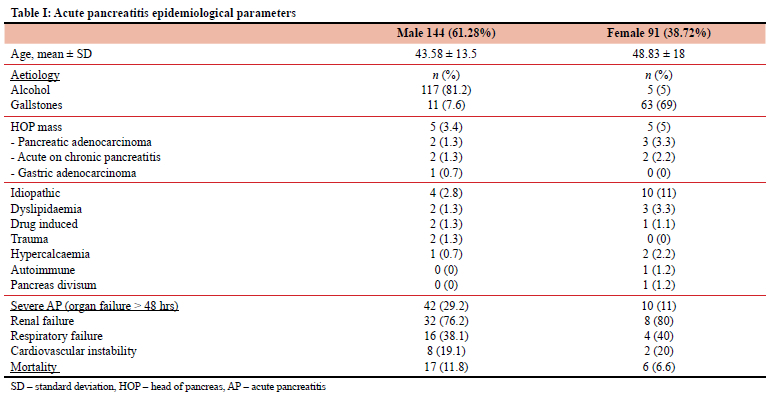
A total of 291 patients with AP were referred from other institutions. Of these, 56 (19%) were excluded as they were referred beyond 72 hours of admission, of whom 24 (42.8%) succumbed to complications. Alcohol was the most common aetiological factor amongst males, followed by gallstones and head of pancreas (HOP) mass. Gallstones were the most common aetiological factor amongst females, followed by idiopathic causes and alcohol/HOP mass. A total of 42 males and 10 females developed organ dysfunction lasting more than 48 hours. The overall mortality rate was 9.8% and higher in males than females. Renal failure was the most common organ dysfunction in both males and females, followed by respiratory and cardiovascular failure (Table I).
Organ failure and mortality prediction
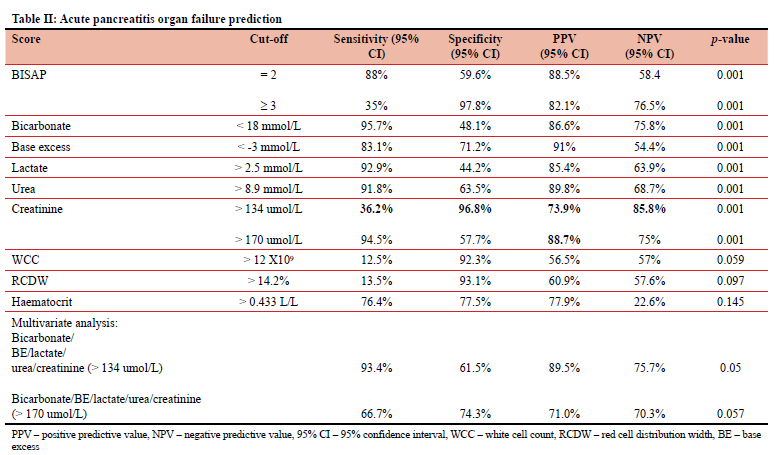
A BISAP score of 2 had a sensitivity of 88% and specificity of 59.6% for predicting organ failure, with a PPV of 88.5% and an NPV of 58.5%. However, a BISAP score > 3 had a sensitivity of 35%, specificity of 97.8%, a PPV of 82.1% and an NPV of 76.5% for predicting organ failure (Table II). The BISAP score had a p-value of 0.001 at prognosticating organ failure, which is statistically significant.
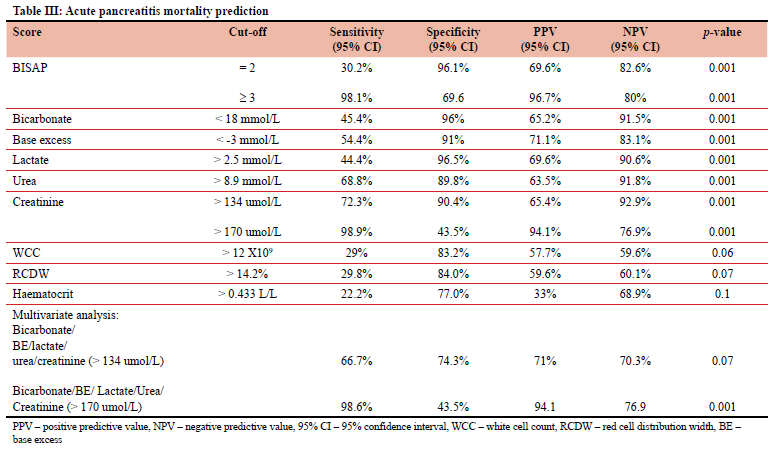
A univariate analysis of a creatinine level above 170 umol/L (Marshall score of 2) demonstrated a sensitivity of 94.5% and specificity of 57.7% for predicting organ failure (PPV = 88.7%, NPV = 75%, p = 0.001). A BISAP score of 2 had a sensitivity of 30.2% and a specificity of 96.1% for predicting mortality (PPV = 69.6%, NPV = 82.5%, p = 0.001). A multivariate analysis of the biomarkers: HCO3, BE, lactate, urea and creatinine (> 170 umol/L) had a sensitivity of 66.7% and specificity of 74.3% at predicting organ failure (PPV= 80.0%, NPV = 70.3%, p = 0.057, 95% CI), however this was not statistically significant (Table II).
A BISAP score of 3 and above had a sensitivity of 98.1% and specificity of 69.6% for predicting mortality (PPV = 96.7%, NPV = 80.0%, p = 0.001) (Table III).
A multivariate analysis of the biochemical markers (including a creatinine above 170 umol/L) had a statistically significant (p = 0.001) a sensitivity of 98.6%, specificity of 43.5% at predicting mortality (PPV = 94.1%, NPV = 76.9% (Table III). The WCC, RCDW and HCT did not show statistically significant correlation with any of the two outcomes, with p-values above 0.05 (Tables II and III).
Discussion
The spectrum and outcome of AP has not changed in the fifteen years since the report of Anderson et al.2 Of the 235 (81%) patients included in the study, 144 (61%) were males and 91 (39%) were females. Alcohol is the most common aetiological factor amongst males, whilst gallstones predominate as an aetiological factor amongst females. AP remains associated with a high mortality rate of 9.8% in the studied cohort, compared to 1-3% internationally.5 Identifying patients at risk for organ failure and associated mortality remains difficult.4 The most commonly used clinical system for grading AP severity is the Ranson criteria, which requires a number of clinical and biochemical parameters to be calculated on admission and 48 hours post admission.4 This makes it both cumbersome and reactive. The Glasgow score has similar shortcomings.5 The APACHE score has been demonstrated to have a high sensitivity and specificity at prognosticating severe AP but it is also a complex system with many variables and adjustments for variations in FIO2.4 The more recently described BISAP score which does not require data points 48 hours after admission has been shown to be a reliable early prognostic marker for mortality, with a sensitivity of 57.1-71.4% and specificity of 87.6% when calculated within 24 hours of admission.46 Our data showed that a BISAP score of 2 is sensitive enough to predict organ failure, although it is limited by a lower specificity and NPV. It should therefore be used with caution when triaging patients at risk of organ failure for referral to tertiary healthcare centres. A creatinine level above 170 umol/L performed slightly better at predicting organ failure, although it was also limited by a low specificity. In other studies, an elevated creatinine has been shown to be reliable in predicting pancreatic necrosis in patients with AP.7 An elevated creatinine is currently not part of the BISAP score but may be useful and should be considered for inclusion in future scoring systems, especially for predicting organ failure.
Our study showed a BISAP score of > 3 to be reliable for predicting mortality in AP and could be used to triage patients at risk of mortality for early referral to tertiary healthcare centres. Patients who were referred to our tertiary hospital beyond 72 hours of admission demonstrated a very high mortality rate. This is postulated to be attributable to under-resuscitation, delayed diagnosis or lack of expertise at the referring hospitals. A multivariate analysis of biochemical parameters was either not statistically significant or had a specificity that was too low to predict both organ failure and mortality. Unlike studies from Turkey, the USA and China,8,9 we could not show any prognostic value for the RCDW. Similarly, we could not show any statistically significant correlation between the haematocrit level and outcome, contrary to what was found in a Japanese study.10
Conclusion
The BISAP score on the day of admission appears to be a reliable tool to prognosticate mortality in AP, but it has limitations with regard to prognosticating organ failure. The BISAP score remains a simple prognostic tool compared to other scoring systems for AP. We thus recommend that it should be used on admission to triage patients with AP, and that patients with a BISAP score of 2 and above should be transferred to tertiary healthcare facilities and high-dependency wards for close monitoring and management.
This is particularly pertinent in our environment where patients who were referred from other institutions after 72 hours had a higher mortality rate, highlighting the need for early identification and referral of at-risk patients. Further studies are required to evaluate whether early referral of patients based on a BISAP score of > 2 can lead to improved outcomes in AP.
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
Ethical approval was obtained from the ethics committees of the Department of Health and the University of KwaZulu-Natal (BREC/00002906/2021).
ORCID
TN Makofane https://orcid.org/0000-0002-1241-6711
DL Clarke https://orcid.org/0000-0002-8467-1455
F Andersen https://orcid.org/0000-0002-9055-8037
L Ferndale https://orcid.org/0000-0003-1644-3124
REFERENCES
1. Anderson F, Thomson SR. Pancreatitis in a high HIV prevalence environment. S Afr Med J. 2017;107(8):706-9. https://doi.org/10.7196/SAMJ.2017.v107i8.10296. [ Links ]
2. Anderson F, Thomson SR, Clarke DL, Loots E. Acute pancreatitis: demographics, aetiological factors and outcomes in a regional hospital in South Africa. S Afr J Surg. 2008;46:83-86. [ Links ]
3. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis-2012: revision of Atlanta classification and definitions by international consensus. Gut. 2013;62:102-11. https://doi.org/10.1136/gutjnl-2012-302779. [ Links ]
4. Papachristou GI, Muddana V, Yadav D, et al. Comparison of BISAP, Ranson's, APACHE-II, and CTSI scores in predicting organ failure, complications, and mortality in acute pancreatitis. Am J Gastroenterol. 2010;105(2):435-41. https://doi.org/10.1038/ajg.2009.622. [ Links ]
5. Leppäniemi A, Tolonen M, Tarasconi A, et al. 2019 WSES guidelines for the management of severe acute pancreatitis, World J Emerg Surg. 2019;14:27-47. https://doi.org/10.1186/s13017-019-0247-0. [ Links ]
6. Di MY, Liu H, Yang ZY, et al. Prediction models of mortality in acute pancreatitis in adults: a systematic review. Ann Intern Med. 2016;165:482-90. https://doi.org/10.7326/M16-0650. [ Links ]
7. Lankisch PG, Weber-Dany B, Maisonneuve P, Lowenfels AB. High serum creatinine in acute pancreatitis: a marker for pancreatic necrosis? Am J Gastroenterol. 2010;105:1196-200. https://doi.org/10.1038/ajg.2009.688. [ Links ]
8. Gravito-Soares M, Gravito-Soares E, Gomes D, Almeida N, Tomé L. Red cell distribution width and red cell distribution width to total serum calcium ratio as major predictors of severity and mortality in acute pancreatitis. BMC Gastroenterol. 2018;18(1):108-16. https://doi.org/10.1186/s12876-018-0834-7. [ Links ]
9. Hu ZD, Wei TT, Tang QQ, et al. Prognostic value of red blood cell distribution width in acute pancreatitis patients admitted to intensive care units: an analysis of a publicly accessible clinical database MIMIC II. Clin Chem Lab Med. 2016;54(7):195-7. https://doi.org/10.1515/cclm-2015-1021. [ Links ]
10. Jinno N, Hori Y, Naitoh I, et al. Predictive factors for the mortality of acute pancreatitis on admission. PLoS One. 2019;14(8):e0221468. https://doi.org/10.1371/journal.pone.0221468. [ Links ]
 Correspondence:
Correspondence:
TN Makofane
Email: tende285@gmail.com
† Deceased 2 January 2023


{kind=link}
{kind=link}
{kind=link}